|
 
 |
| ORIGINAL ARTICLE |
|
| Year : 2014 | Volume
: 9
| Issue : 1 | Page : 11-14 |
|
Surgical management of male breast cancer patients referred to the national cancer institute: University of Gezira; the forgotten lesson
Ahmed M Elhaj1, Ahmed A Alshaikh2, Dafalla O Abuidris1, Algaylani A Eltayeb1
1 Department of Oncology, National Cancer Institute University of Gezira, Wad Madani, Sudan
2 Department of Surgery, Faculty of Medicine, University of Gezira, Wad Madani, Sudan
| Date of Web Publication | 13-Nov-2014 |
Correspondence Address:
Ahmed M Elhaj
National Cancer Institute, University of Gezira, Wad Madani, PO Box 20
Sudan
  | Check |
DOI: 10.4103/1858-5000.144646 
Background: Male breast cancer (MBC) is a rare disease accounting for about 1% of breast cancer patients worldwide. There is a lack of data about MBC patients and their management in Sudan. Patients and Methods: Medical records of all cancer patients treated at the Department of Oncology, National Cancer Institute-University of Gezira (NCI-UG), Wad Medani, Gezira State, Sudan, in the period from April 1999 to December 2010, were reviewed with regard to MBC. Variables assessed were individual, clinical characteristics, and initial surgical treatment. Results: There were 1,505 (19.2%, 1505/7836) Sudanese breast cancer patients treated at the NCI-UG from April 1999 to December 2010. The MBC frequency was 2.3% (34/1505); all were included in the current study. Eighteen patients underwent upfront surgery and these patients formed the subjects for the current study. Mastectomy and axillary clearance (AC) was performed for 11 (32.4%) patients. The rest- 7 patients- underwent total mastectomy only. The incidence of positive surgical margins is remarkable (27%). Only one of those with positive surgical margin was subjected to re-excision. Among those who underwent AC only two had adequate axillary lymph nodes clearance. Discussion: The results have been compared with similar studies and showed similar approach in management with minor differences Conclusion: These results indicated inadequate surgical management and urgent needs for improvement in the treatment of this rare type of cancer. Keywords: Male breast cancer, Sudan, surgery
How to cite this article:
Elhaj AM, Alshaikh AA, Abuidris DO, Eltayeb AA. Surgical management of male breast cancer patients referred to the national cancer institute: University of Gezira; the forgotten lesson. Sudan Med Monit 2014;9:11-4 |
How to cite this URL:
Elhaj AM, Alshaikh AA, Abuidris DO, Eltayeb AA. Surgical management of male breast cancer patients referred to the national cancer institute: University of Gezira; the forgotten lesson. Sudan Med Monit [serial online] 2014 [cited 2018 Mar 20];9:11-4. Available from: http://www.sudanmedicalmonitor.org/text.asp?2014/9/1/11/144646 |
| Introduction | |  |
Breast cancer constitutes a major public health issue globally with over 1 million new cases diagnosed annually, resulting in over 400,000 annual deaths and about 4.4 million women living with the disease. It is the most common site specific malignancy affecting women and the most common cause of cancer mortality in women worldwide. [1],[2],[3]
Breast cancer accounted for about one-fifth of all cancer patients treated in Sudan and is the most frequent site-specific malignancy seen at both Radiation and Isotopes Center in Khartoum (RICK) (20%, i.e., 2,084/10,410 recorded cancer patients during the period 1967-1984) and National Cancer Institute of University of Gezira (NCI-UG) (19%, i.e., 1,009⁄5,236 recorded cancer patients during the period 1999-2008). [2],[4],[5],[6],[7],[8],[9],[10],[11] Similar frequencies were observed across different studies during the period 1935-2006 (16%, 4,005/25,064) as reviewed by Awadelkarim et al. [12] This may partly reflect awareness bias, as breast masses or ulcerated lesions are readily evident to the patients themselves, as well as hospitalization bias, given the presence of radiotherapy facilities at RICK and NCI-UG. [12]
Male breast cancer (MBC) is a rare disease accounting for about 1% of breast cancer patients. [13],[14],[15],[16] However, its incidence is reportedly higher in populations of African origin. [16],[17],[18],[19],[20] Owing to its rarity there is worldwide lack of studies dealing specifically with MBC. [14],[21],[22],[23] In fact, randomized controlled studies in MBC patients are almost not existing and management guidelines were extrapolated from studies conducted in females. [14],[15],[19],[22],[23],[24]
Published data on MBC from Sudan is lacking. A recent study by Elhaj et al. [25] investigated the current status of MBC in Sudan by focusing on individual and clinical/pathological characteristics, treatment and follow-up, and treatment outcome parameters of MBC patients attending NCI-UG in the period from April 1999 to December 2010.
The current study is expanding the data published on the management of MBC in NCI-UG by concentrating mainly on the surgical management. Elhaj et al. published an article on the improvement in managing breast cancer in Sudan and showed a progress in this aspect, but unfortunately many surgeons in the region failed to follow what they have already learned in female breast cancer when managing MBC.
| Patients and methods | | |
Medical records of all cancer patients treated at the Department of Oncology, NCI-UG, Wad Medani, Gezira State, Sudan, in the period from April 1999 to December 2010, were reviewed with regard to MBC. Variables assessed were individual, clinical characteristics, and initial surgical treatment.
| Results | | |
There were 1,505 (19.2%, 1,505/7,836) Sudanese breast cancer patients treated at the NCI-UG from April 1999 to December 2010. The MBC frequency was 2.3% (34/1,505); all were included in the current study. The mean age at MBC diagnosis was 56.5 ± 15.8 years (age range: 22-85 years). The mean period between complaint awareness and MBC diagnosis was 25.3 ± 46 months (median, 8 months; range: 1-240 months). Most patients presented with large breast lump (mean lump size, 6.8 ± 3.0 cm; range: 2-12 cm). Breast lump was the presenting symptom in 21 patients (61.8%). Breast lump and ulceration were seen in 8 patients (23.6%). Other 3 (8.8%) patients presented with symptoms indicating metastatic disease and 1 (2.9%) was a recurrence (initial complain was not available). Disease presentation data was not available for one patient (2.9%). The disease was affecting the left breast in 19/34 (55.9%) and only 1 (2.9%) patient presented with bilateral disease. Two (5.2%) MBC patients reported past history of trauma. Nipple discharge was reported in 7/34 (20.6%) patients and nipple retraction in 1 (2.9%) patient. Stage I was documented in 1 (2.9%) patient, stage II in 6 (17.6%) patients, stage III in 12 (35.3%) patients, stage IV in 9 (26.5%) patients and 5 (14.7%) patients were with unknown stage.
Surgical management
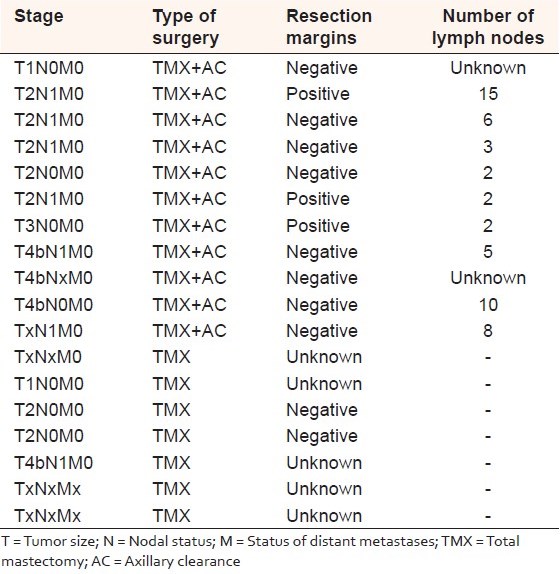
Eighteen patients underwent upfront surgery and these patients formed the subjects for the current study. Mastectomy and axillary clearance (AC) was performed for 11 (32.4%) patients. The tumors were classified as T1 to T4 and lymph nodes as N0 or N1. Three patients in this group end with positive surgical margins (3/11-27.2%) and one of them underwent re-excision. Among those who underwent AC only two had adequate axillary lymph nodes clearance (total number of lymph nodes harvested was 15 and 10) and the total number of lymph nodes ranged between 15 and 2. Positive lymph nodes detected in 8 patients (8/11-72.7%) and their number ranged between 1 and 3 lymph nodes.
The rest- 7 patients- underwent total mastectomy (TMX) only. Tumors were classified as T1, T2, T4 or unknown with N0 (3 patients), N1 (one patient) or Nx (3 patients) axillary lymph nodes. There were no data on the status of surgical margins for 5 of them and the other 2 patients had uninvolved surgical margins [Table 1].
| Discussion | | |
Male breast cancer is a rare disease. Published data on its occurrence in Sudan is lacking. A recent article published on this topic by Elhaj et al. has characterized it in central Sudan. [25]
Recent published data suggest that the incidence of MBC appears to be rising. Review of Surveillance, Epidemiology and End Result (SEER) data indicate a rise in the incidence of MBC, from 1.0/100,000 men in the late 1970s to 1.2/100,000 men from 2000 to 2004. A similar analysis of the United Kingdom Association of Cancer Registries database identified a parallel trend, with the incidence of MBC rising steadily between 1985 and 2004. Furthermore, while it is widely cited that MBC accounts for <1% of all cases of breast malignancy, these figures are highly discrepant among series, possibly varying due to differences in geography and race. With respect to race, SEER data indicates that African American males have a significantly higher likelihood of developing breast cancer when compared to whites or Asian Americans/Pacific Islanders. Thus, with the incidence of MBC on the rise and the prevalence potentially underestimated, there is a need to better understand the clinicopathological features of this disease. Furthermore, it appears that males have derived lesser benefits from the substantial advances in breast cancer therapy made over the past several decades. [26]
As with female breast cancer, for most of the 20 th century the standard treatment for localized breast cancer in men was radical mastectomy, which has now been superseded by less invasive procedures such as modified radical or simple mastectomy, with no detectable decline in survival. Wide excision in MBC will almost always include resection of the nipple due to the small amount of breast tissue, and there is some evidence that this is not the most effective method of local control. For invasive MBC, axillary dissection is usually done, either sampling or clearance. To establish axillary status in clinically node-negative cases evidence building up of the accuracy and low morbidity associated with sentinel-node biopsy. The technique has also been used in men with similarly encouraging results and sentinel node biopsy will probably become standard practice in the future for node-negative MBC. [21]
During the last years, there has been a noticeable progress in surgical management of female breast cancer in Sudan; [27] unfortunately, this has not been reflected on surgical management of MBC at least on cases reported here.
By reviewing the available data on this series of patients, many patients were found to be not suitable for upfront surgery (47%). This indicates advanced stage at presentation which is also the case in other cancers, including female's breast cancer in Sudan. [28] Almost half of the patients (53%) underwent upfront surgery. Unfortunately many of them (39%) underwent mastectomy only without any axillary surgery. This could reflect the management that many surgeons undertake when dealing with male breast lumps. In fact, this problem is also encountered in management of female breast cancer. [27]
The rest underwent TMX and AC (61% 11/18). The incidence of positive surgical margins is remarkable (27%). Only one of those with positive surgical margin was subjected to re-excision.
Only 2 patients underwent adequate AC (10 or more lymph nodes dissected). The number of patients with positive lymph nodes was eight (8/11) and the number of positive lymph nodes were 1-3. Adequate axillary dissection is important in node positive patients both to ensure removal of all involved nodes to optimize local control and to obtain the maximum prognostic information. [29] Warren and Tompkins were the first to demonstrate that the risk of loco-regional failure was directly proportional to the extent of axillary lymph node involvement with tumor at the time of diagnosis. [30] Other studies have shown the risk of relapse increasing from <8% in patients with no axillary node involvement to 27% in patients with nodes with positive findings. [31]
None of the 18 patients was considered to receive neoadjuvant chemotherapy (NACT) which is a common practice nowadays when managing locally advanced female breast cancer. Use of NACT allows an early initiation of systemic treatment, inhibition of postsurgical growth spurt, delivery of chemotherapy through intact tumor vasculature, in vivo assessment of response, and down-staging of primary tumor and lymph node metastases to facilitate less radical loco-regional therapy with safe surgical margins and adequate axillary dissection. [32]
| Conclusion | | |
Initial surgical management of MBC in Gezira area is inadequate and need to be improved. Existing national management guidelines for females with breast cancer could easily and correctly be applied when managing males with same disease.
| References | | |
| 1. | Veronesi U, Boyle P, Goldhirsch A, Orecchia R, Viale G. Breast cancer. Lancet 2005;365:1727-41.  |
| 2. | Parkin DM, Bray F, Ferlay J, Pisani P. Global cancer statistics, 2002. CA Cancer J Clin 2005;55:74-108. |
| 3. | Ferlay J, Bray F, Pisani P, Parkin DM. GLOBOCAN 2002: Cancer Incidence, Mortality and Prevalence Worldwide. Lyon: IARC Press; 2004. |
| 4. | Awadelkarim KD, Arizzi C, Elamin EO, Hamad HM, De Blasio P, Mekki SO, et al. Pathological, clinical and prognostic characteristics of breast cancer in Central Sudan versus Northern Italy: Implications for breast cancer in Africa. Histopathology 2008;52:445-56. |
| 5. | Awadelkarim KD, Aceto G, Veschi S, Elhaj A, Morgano A, Mohamedani AA, et al. BRCA1 and BRCA2 status in a Central Sudanese series of breast cancer patients: Interactions with genetic, ethnic and reproductive factors. Breast Cancer Res Treat 2007;102:189-99. |
| 6. | Hamad HM. Cancer initiatives in Sudan. Ann Oncol 2006;17 Suppl 8:viii32-6. [ PUBMED] |
| 7. | INMO Annual Report. Information and Research Center, Statistic Unit, Department of Oncology, Institute of Nuclear Medicine Molecular Biology and Oncology (INMO), Wad Medani, Sudan; 2006. |
| 8. | INMO Annual Report. Information and Research Center, Statistic Unit, Department of Oncology, Institute of Nuclear Medicine Molecular Biology and Oncology (INMO), Wad Medani, Sudan; 2001. |
| 9. | Ferlay J, Bray P, Parkin DM. Globocan 2002: Cancer Incidence, Mortality ad Prevalene Worldwide. Lyon: IARC Press; 2004. |
| 10. | Ahmed HG, Ali AS, Almobarak AO. Frequency of breast cancer among Sudanese patients with breast palpable lumps. Indian J Cancer 2010;47:23-6. [ PUBMED]  |
| 11. | Hidayatalla A, Rahman EA. The radiation and isotope centre, Khartoum. 1967-1984. In: Parkin DM, editor. Cancer Occurrence in Developing Countries. Lyon: IARC; 1986. p. 82-7. |
| 12. | Awadelkarim KD, Mariani-Costantini R, Elwali NE. Cancer in the Sudan: An overview of the current status of knowledge on tumor patterns and risk factors. Sci Total Environ 2012;423:214-28. |
| 13. | Comet B, Cutuli B, Penault-Llorca F, Bonneterre J, Belkacémi Y. Male breast cancer: A review. Bull Cancer 2009;96:181-9. |
| 14. | Agrawal A, Ayantunde AA, Rampaul R, Robertson JF. Male breast cancer: A review of clinical management. Breast Cancer Res Treat 2007;103:11-21. |
| 15. | Gómez-Raposo C, Zambrana Tévar F, Sereno Moyano M, López Gómez M, Casado E. Male breast cancer. Cancer Treat Rev 2010;36:451-7. |
| 16. | Sasco AJ, Lowenfels AB, Pasker-de Jong P. Review article: Epidemiology of male breast cancer. A meta-analysis of published case-control studies and discussion of selected aetiological factors. Int J Cancer 1993;53:538-49. |
| 17. | Rachid S, Yacouba H, Hassane N. Male breast cancer: 22 case reports at the National Hospital of Niamey-Niger (West Africa). Pan Afr Med J 2009;3:15. |
| 18. | O'Malley C, Shema S, White E, Glaser S. Incidence of male breast cancer in california, 1988-2000: Racial/ethnic variation in 1759 men. Breast Cancer Res Treat 2005;93:145-50. |
| 19. | Ravandi-Kashani F, Hayes TG. Male breast cancer: A review of the literature. Eur J Cancer 1998;34:1341-7. |
| 20. | Fentiman IS, Fourquet A, Hortobagyi GN. Male breast cancer. Lancet 2006;367:595-604. |
| 21. | Thalib L, Hall P. Survival of male breast cancer patients: Population-based cohort study. Cancer Sci 2009;100:292-5. |
| 22. | Barh D. Biomarkers, critical disease pathways, drug targets, and alternative medicine in male breast cancer. Curr Drug Targets 2009;10:1-8. [ PUBMED] |
| 23. | Korde LA, Zujewski JA, Kamin L, Giordano S, Domchek S, Anderson WF, et al. Multidisciplinary meeting on male breast cancer: Summary and research recommendations. J Clin Oncol 2010;28:2114-22. |
| 24. | Rudlowski C. Male Breast Cancer. Breast Care (Basel) 2008;3:183-89. [ PUBMED] |
| 25. | Elhaj A, Ismaeel A, Awadelkarim K. Male breast cancer patients: A retrospective study of patients characteristics and treatment outcome at the National Cancer Institute (NCI-UG) - Central Sudan. Pan Arab J Oncol 2012;5:18-23. |
| 26. | Onami S, Ozaki M, Mortimer JE, Pal SK. Male breast cancer: An update in diagnosis, treatment and molecular profiling. Maturitas 2010;65:308-14. |
| 27. | Elhaj A, Ismail A, Awadelkarim K. National guidelines for management of breast cancer: For enforcement or persuasion? Sudan Med J 2012;48:213-8. |
| 28. | Hamad HM. Cancer initiatives in Sudan. Eur Soc Med Oncol 2006;17 Suppl 8: vii-32-vii-36. |
| 29. | Byrne BE, Cutress RI, Gill J, Wise MH, Yiangou C, Agrawal A. The axillary nodal harvest in breast cancer surgery is unchanged by sentinel node biopsy or the timing of surgery. Int J Breast Cancer 2012;2012:467825. |
| 30. | Warren S, Tompkins VN. Significance of the extent of axillary metastases in carcinoma of the female breast. Surg Gynecol Obstet 1943;76:327-30. |
| 31. | Yildirim E. Locoregional recurrence in breast carcinoma patients. Eur J Surg Oncol 2009;35:258-63. [ PUBMED] |
| 32. | Rustogi A, Budrukkar A, Dinshaw K, Jalali R. Management of locally advanced breast cancer: Evolution and current practice. J Cancer Res Ther 2005;1:21-30. |
[Table 1]
|









 Search Pubmed for
Search Pubmed for