|
 
 |
| REVIEW ARTICLE |
|
| Year : 2014 | Volume
: 9
| Issue : 2 | Page : 87-90 |
|
Characterization of coronary artery obstruction and related findings in ischemic heart patients using cardiac scintigraphy
Eltayeb Wagiallah Eltayeb1, Yousif Mohamed Y Abdallah2, Mohamed E Gar-Elnabi3, Mohamed Ahmed Ali4
1 Department of Nuclear Medicine, Radiation and Isotopes Center of Khartoum; Department of Nuclear Medicine, Elnileen Medical Center, Khartoum, Sudan
2 Department ofRadiotherapy and Nuclear Medicine, College of Medical Radiological Science, Sudan University of Science and Technology, Khartoum, Sudan; Department ofRadiotherapy and Nuclear Medicine, College of Applied Medical Science, Al Majmah University, Riyadh, Saudi Arabia
3 Department of Nuclear Medicine, Elnileen Medical Center, Khartoum, Sudan
4 Department ofRadiotherapy and Nuclear Medicine, College of Medical Radiological Science, Sudan University of Science and Technology, Khartoum, Sudan; Department ofRadiotherapy and Nuclear Medicine, College of Medical Radiological Science, Al Qasim University, Al Qasim, Buraidah, Saudi Arabia
| Date of Web Publication | 9-Dec-2014 |
Correspondence Address:
Yousif Mohamed Y Abdallah
College of Medical Radiological Science, Sudan University of Science and Technology, Khartoum, Sudan
  | Check |
DOI: 10.4103/1858-5000.146582 
This study conducted to characterize of coronary artery obstruction and related findings in ischemic heart patients using cardiac scintigraphy for the identification of myocardial ischemia, 146 patients were studied at basal conditions and also asked for fasting after night till the intravenous injection of the radiopharmaceutical, after the injection time about 15-20 min the patient should eat a fatty meal and chocolate for the good excretion of the gall bladder, to evaluate the performance and regional wall motion of the lef ventricle. The results showed that the body mass index percentage in this sample was in the range of 43.05-61.05. The number of patients who were catheter candidate was 56 patients with 43%, and the patients were not candidate to cathode were 74 patients with 57% of all patients. For the group of patients where type of ischemia was assessed, 29.5% of patients were reversible posterior and inferior wall, 15.1% of patients were fixed large from apex to base, 9.6% of patients were mild basal inferior wall, 4.8% of patients were mild anterior wall, 6.2% of patients were antro septal. 34.9% of patients were moderate ischemia. Keywords: Contrast ventriculography, myocardial ischemia, myocardial scintigraphy
How to cite this article:
Eltayeb EW, Abdallah YY, Gar-Elnabi ME, Ali MA. Characterization of coronary artery obstruction and related findings in ischemic heart patients using cardiac scintigraphy
. Sudan Med Monit 2014;9:87-90 |
How to cite this URL:
Eltayeb EW, Abdallah YY, Gar-Elnabi ME, Ali MA. Characterization of coronary artery obstruction and related findings in ischemic heart patients using cardiac scintigraphy
. Sudan Med Monit [serial online] 2014 [cited 2018 Mar 6];9:87-90. Available from: http://www.sudanmedicalmonitor.org/text.asp?2014/9/2/87/146582 |
| Introduction | |  |
The heart is the pump responsible for maintaining adequate circulation of oxygenated blood around the vascular network of the body. It is a four-chamber pump, with the right side receiving deoxygenated blood from the body at low pressure and pumping it to the lungs (the pulmonary circulation) and the left side receiving oxygenated blood from the lungs and pumping it at high pressure around the body (the systemic circulation). [1],[2],[3] The myocardium (cardiac muscle) is a specialized form of muscle, consisting of individual cells joined by electrical connections. The contraction of each cell is produced by a rise in intracellular calcium concentration leading to spontaneous depolarization, and as each cell is electrically connected to its neighbor, contraction of one cell leads to a wave of depolarization and contraction across the myocardium. This depolarization and contraction of the heart is controlled by a specialized group of cells localized in the sino-atrial node in the right atrium-the pacemaker cells. [4],[5],[6] These cells generate a rhythmical depolarization, which then spreads out over the atria to the atrio-ventricular node, the atria then contract to push the blood into the ventricles. [7],[8],[9] The electrical conduction passes via the atrioventricular node to the bundle of His, which divides into right and left branches and then spreads out from the base of the ventricles across the myocardium. This leads to a "bottom-up" contraction of the ventricles, forcing blood up and out into the pulmonary artery (right) and aorta (left). The atria then re-fill as the myocardium relaxes. The "squeeze" is called systole and normally lasts for about 250 ms. The relaxation period, when the atria and ventricles re-fill, is called diastole; the time given for diastole depends on the heart rate. The heart needs its own reliable blood supply in order to keep beating; hence it receives the blood via the coronary circulation. There are two main coronary arteries, the left and right coronary arteries, and this branch further to form several major branches (see appendix). The coronary arteries lie in grooves (sulci) running over the surface of the myocardium, covered over by the epicardium, and have many branches that terminate in arterioles supplying the vast capillary network of the myocardium. However these coronary artery (CA) frequently susceptible to many disorders and diseases; of either acquired or congenital one such as: (septum patency as congenital and Ischemic and Infarction diseases as acquired) and the focus of this research is to characterize the CA obstruction and Related Findings in Ischemic Heart Patients Using Cardiac Scintigraphy. Indeed such obstruction could accompany with fatal consequences or morbidities. In this realm; revealed the CA obstruction using Tc99m-MIBI, Rest and Stress studies in 11 patients with coronary disease who had normal Rest study, new regions of dysfunction developed during exercise (P < 0.001), and in 10, ejection fraction dropped 7-47%. Fourteen age-matched normal subjects were studied; during exercise none had regional dysfunction, and each increased ejection fraction (average increase, 23% ± 3% [±standard error], P < 0.001 as compared with patients with coronary disease). Radionuclide Scintigraphy during exercise permits accurate assessment of the presence and functional severity of ischemic heart disease. Worldwide the coronary artery obstruction (CAO) has been as an endemic disease in some countries, such as USA (American Heart Association). [6],[7],[8],[9],[10],[11],[12]
| Methods | | |
This study was carried out at the Nuclear Medicine department of Elnileen Medical Center. The analysis comprised 146 patients of both sexes, with and without previous myocardial infarction (MI), referred for cardiac catheterization and coronary angiography due to symptomatic ischemic heart disease, documented by non-invasive methods. Diabetic patients, those with valvular heart disease alone or associated with myocardial hypertrophy, and those who could not discontinue the use of nitrates 24 h prior to any of the procedures were excluded. When the patient referred for heart Scintigraphy, the patient asked for the medication intake if found (stopped for 24 h before the study, as well as Caffeine containing foods or drinks), because it reduced the radiotracer uptake. Also asked for fasting after night till the intravenous injection of the radiopharmaceutical, after the injection time about 15-20 min the patient should eat a fatty meal and chocolate for the good excretion of the gallbladder (it has normal high uptake of the radiotracer). After 45 min to 1 h after the injection the patient entered to the gamma camera for imaging, and asked to pick out his/her upper clothes and lie supine in the imaging table to fix the electrocardiogram electrodes on his upper right side near Rt. Clavicle, Lt. Clavicle and Lt. Lower thoracic ribs. Then the computer already set on the gated single photon emission computed tomography for the rest hear study, and the machine started the acquisition form the right anterior oblique (−45°) to left posterior oblique (135°), step and shoot technique till the acquisition finished. Then the processing of the acquired study by emission computed tomography protocol for obtaining the serial images of sliced heart (Coronal, Sagittal and Transverse cuts), as well as bollar map and ejection fraction of the heart and any available information if interested on A4 paper with a colored scale. For the Stress heart Scintigraphy used the same process that of Rest study in addition to using treadmill as exercise for elevating the heart rate or Pharmacological agent (Persantin) as stress action after the heart reaches his maximum effort then the radiopharmaceutical should be injected, then all process as same as the rest study. The data analyzed using SPSS program.
| Results | | |
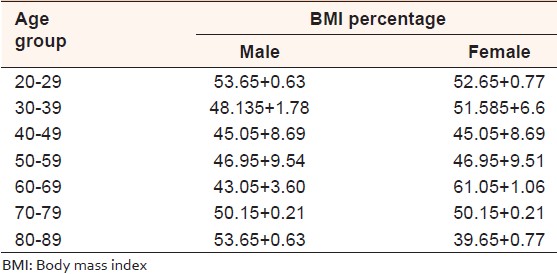
To characterize of coronary artery obstruction and related findings in ischemic heart patients using cardiac scintigraphy for the identification of myocardial ischemia. The sample of this study was 146 patients with different age distribution and body mass index (BMI). For the group of patients where age distribution was measured, 1.2% of patients were within the 20-29 years age range, 5% of patients were within the 30-39 years age range, 16% of patients were within the 40-49 years age range, 35% of patients were within the 50-59 years age range, 34.6% of patients were within the 60-69 years age range, 7% of patients were within the 60-69 years age range and 1.2% of patients were within the 80-89 years age range. For the group of patients where BMI was measured, 1.2% of patients were within the 53.65 + 0.63 (male), 52.65 + 0.77 (female) BMI ratio range, 5% of patients were within the 48.135 + 1.78 (male), 51.585 + 6.6 (female) BMI ratio range, 16% of patients were within the 45.05 + 8.69 (male), 45.05 + 8.69 (female) BMI ratio range, 35% of patients were within the 46.95 + 9.54 (male) and 46.95 + 9.51 (female) BMI ratio range, 34.6% of patients were within the 43.05 + 3.60 (male) and 61.05 + 1.06 (female) BMI ratio range. 7% of patients were within the 50.15 + 0.21 (male) and 50.15 + 0.21 (female) BMI ratio range. 1.2% of patients were within the 53.65 + 0.63 (male) and 39.65 + 0.77 (female) BMI ratio range. The key parameters for this group are shown in [Table 1].
Contrast ventriculography was done for 50 patients the results were the five already mentioned segments were compared in regard wall motion changes after the isosorbide mononitrate administration. In the apical segment, before drug administration, the results were: 1 normal, 8 hypokinetic, and 20 dyskinetic segments. After drug administration, 19 were identified as normal segments, only 7 as hypokinetic and 12 as dyskinetic (P = 0.0003). In the anterobasal segment, before the isosorbide mononitrate administration, the results were: 15 normal, 14 hypokinetic, and 2 akinetic segment. After the drug administration, 21 segments were identified as normal and only one as hypokinetic, and the one that was akinetic prior to drug use, remained so (P = 0.0033). In the posterobasal segment, before drug administration, the results were: 15 normal, 14 hypokinetic, and 2 akinetic segments. After drug use, 21 segments were normal, 8 hypokinetic, 2 dyskinetic, and 4 akinetic; among these segments, one that was first characterized as akinetic, turned into dyskinetic (P = 0.0015). In the anterolateral segment, at basal conditions, the results were: 7 normal, 20 hypokinetic, 4 dyskinetic, and 3 akinetic segment. With the use of the drug, there were alterations: 22 normal, 2 hypokinetic, 1 dyskinetic, and 4 akinetic segment (P = 0.0001). In the diaphragmatic segment, prior to drug administration, the results were: 11 normal, 22 hypokinetic, 7 dyskinetic, and 4 akinetic. After drug administration, the results changed: 22 normal, 3 hypokinetic, and 4 akinetic segments (P = 0.001) [Table 2].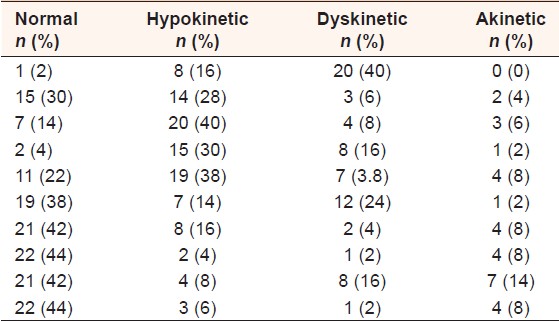 | Table 2: Characterization of the sample of study in relation to ventriculography, when compared before and after use of contrast
Click here to view |
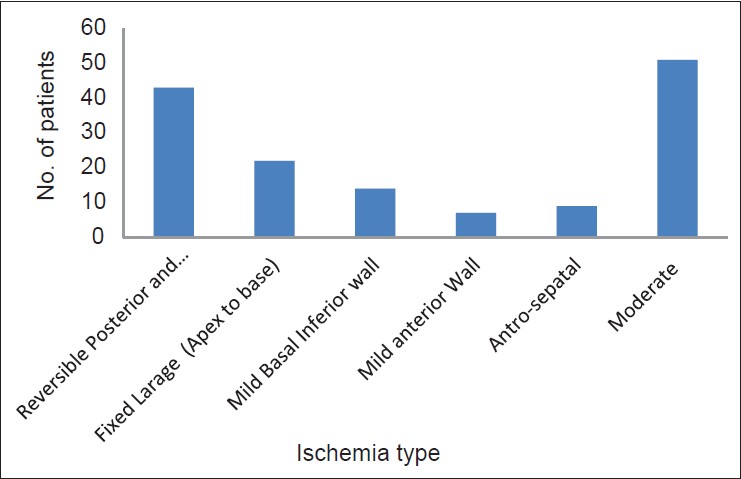
For the group of patients where type of ischemia was assessed, 29.5% of patients were reversible posterior and Inferior wall, 15.1% of patients were fixed large from apex to base, 9.6% of patients were mild basal inferior wall, 4.8% of patients were mild anterior wall., 6.2% of patients were antro-septal. 34.9% of patients were moderate ischemia. The key parameters for this group are shown in [Figure 1].
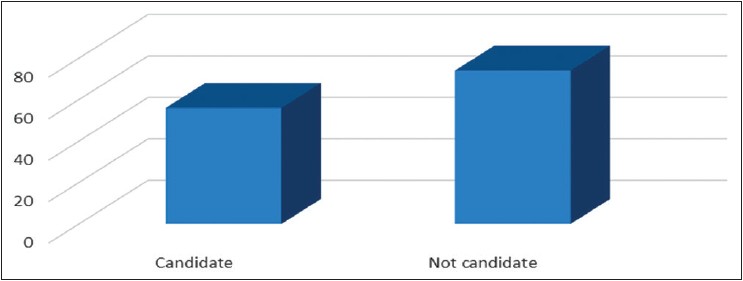
The number of patients were catheter candidate were 56 patient with 43% and the patients were not candidate to cathode were 74 patients with 57% of all patients in this study as shown in [Figure 2].
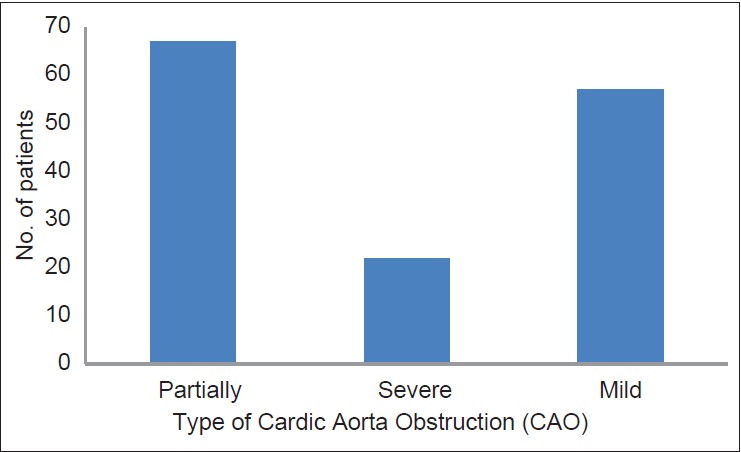
Regarding to number of patients with CAO, the study showed that were 45.9% of patients had partially CAO, 15.1% of patients had severe CAO and 39% had mild CAO of all patients in this study as shown in [Figure 3].
| Conclusion | | |
This study was carried out at the Nuclear Medicine department of Elnileen Medical Center. The analysis comprised 146 patients of both sexes, with and without previous MI, referred for cardiac catheterization and coronary angiography due to symptomatic ischemic heart disease, documented by non-invasive methods. Diabetic patients, those with valvular heart disease alone or associated with myocardial hypertrophy, and those who could not discontinue the use of nitrates 24 h prior to any of the procedures were excluded. Contrast ventriculographies was done for 50 patients the results were the five already mentioned segments were compared in regard wall motion changes after the isosorbide mononitrate administration. In the apical segment, before drug administration, the results were: 1 normal, 8 hypokinetic and 20 dyskinetic segments. After drug administration, 19 were identified as normal segments, only 7 as hypokinetic, and 12 as dyskinetic (P = 0.0003). In the anterobasal segment, before the isosorbide mononitrate administration, the results were: 15 normal, 14 hypokinetic, and 2 akinetic segment. After the drug administration, 21 segments were identified as normal and only one as hypokinetic, and the one that was akinetic prior to drug use, remained so (P = 0.0033). In the posterobasal segment, before drug administration, the results were: 15 normal, 14 hypokinetic, and 2 akinetic segments. After drug use, 21 segments were normal, 8 hypokinetic, 2 dyskinetic, and 4 akinetic; among these segments, one that was first characterized as akinetic, turned into dyskinetic (P = 0.0015). In the anterolateral segment, at basal conditions, the results were: 7 normal, 20 hypokinetic, 4 dyskinetic, and 3 akinetic segment. With the use of the drug, there were alterations: 22 normal, 2 hypokinetic, 1 dyskinetic, and 4 akinetic segment (P = 0.0001). In the diaphragmatic segment, prior to drug administration, the results were: 11 normal, 22 hypokinetic, 7 dyskinetic, and 4 akinetic. After drug administration, the results changed: 22 normal, 3 hypokinetic, and 4 akinetic segments (P = 0.001) [Table 2].
| References | | |
| 1. | Young T, Palta M, Dempsey J, Skatrud J, Weber S, Badr S. The occurrence of sleep-disordered breathing among middle-aged adults. N Engl J Med 1993;328:1230-5.  |
| 2. | Cherry SR, Sorenson JA, Phelps ME (2003). Physics in nuclear medicine, 3 rd ed. Saunders: Philadelphia. PA. p. 325-359. |
| 3. | Drager LF, Bortolotto LA, Lorenzi MC, Figueiredo AC, Krieger EM, Lorenzi-Filho G. Early signs of atherosclerosis in obstructive sleep apnea. Am J Respir Crit Care Med 2005;172:613-8. |
| 4. | Shahar E, Whitney CW, Redline S, Lee ET, Newman AB, Nieto FJ, et al. Sleep-disordered breathing and cardiovascular disease: Cross-sectional results of the Sleep Heart Health Study. Am J Respir Crit Care Med 2001;163:19-25. |
| 5. | Naughton MT, Bradley TD. Sleep apnea in congestive heart failure. Clin Chest Med 1998;19:99-113. |
| 6. | Peker Y, Kraiczi H, Hedner J, Löth S, Johansson A, Bende M. An independent association between obstructive sleep apnoea and coronary artery disease. Eur Respir J 1999;14:179-84. |
| 7. | Somers VK, Dyken ME, Clary MP, Abboud FM. Sympathetic neural mechanisms in obstructive sleep apnea. J Clin Invest 1995;96:1897-904. |
| 8. | Kato M, Roberts-Thomson P, Phillips BG, Haynes WG, Winnicki M, Accurso V, et al. Impairment of endothelium-dependent vasodilation of resistance vessels in patients with obstructive sleep apnea. Circulation 2000;102:2607-10. |
| 9. | Shamsuzzaman AS, Winnicki M, Lanfranchi P, Wolk R, Kara T, Accurso V, et al. Elevated C-reactive protein in patients with obstructive sleep apnea. Circulation 2002;105:2462-4. |
| 10. | Hanly P, Sasson Z, Zuberi N, Lunn K. ST-segment depression during sleep in obstructive sleep apnea. Am J Cardiol 1993;71:1341-5. |
| 11. | Schwartz PJ, La Rovere MT, Vanoli E. Autonomic nervous system and sudden cardiac death. Experimental basis and clinical observations for post-myocardial infarction risk stratification. Circulation 1992;85:I77-91. |
| 12. | Lazarus A, Py A, Guérin F, Valty J, Le Heuzey JY. Arrhythmia and syndrome of obstructive sleep apnea in adults. Arch Mal Coeur Vaiss 1993;86:1753-9. |
[Figure 1], [Figure 2], [Figure 3]
[Table 1], [Table 2]
|









 Search Pubmed for
Search Pubmed for