|
 
 |
| ORIGINAL ARTICLE |
|
| Year : 2015 | Volume
: 10
| Issue : 2 | Page : 45-49 |
|
A study of acute ST elevation myocardial infarction in young patients from government teaching hospital
Chirayu Vijaykumar Vaidya1, Drusty Krishnasevak Majmudar2
1 Department of Medicine, GMERS Medical College and Hospital, Gandhinagar, Gujarat, India
2 Department of Radio Diagnosis, AMC MET Medical College, Ahmadabad, Gujarat, India
| Date of Web Publication | 16-Jul-2015 |
Correspondence Address:
Dr. Chirayu Vijaykumar Vaidya
Safalya, Plot No 1371/2, Sector-2/B, Gandhinagar - 382 002, Gujarat
India
  | Check |
DOI: 10.4103/1858-5000.160939 
Context: Myocardial infarction (MI) is being recognized in a younger age group in recent years. MI in the young adult may differ from that in the elderly by virtue of its greater incidence of risk factors and atherosclerotic etiology, the heavy preponderance of male patients. Aims: The aim of this study was to study clinical profile, risk factors, complications, infarct type, management, and outcome in patients 45 years or younger (young) admitted with acute ST elevation MI at a Government teaching hospital in Gandhinagar, Gujarat. Subjects and Methods: This is a retrospective study of all new young patients managed for acute ST elevation MI in ICCU of GMERS Medical College and Hospital, Gandhinagar, Gujarat from January 1, 2012 to December 31, 2013. Data were analyzed with SPSS version 21 software. Results: The mean age of 40.95 years with (89%) males and, (11%) females and male to female ratio was 8.1:1. Most patients (58.9%) were from 41 to 45 years age. The most common clinical presentation was chest pain and sweating (97.3% vs. 11%). Most patients (65.8%) arrived in hospital within 6 h from the onset of symptoms. The most common area of infarction was anterior wall and inferior (61.3% vs. 22.7%). The most common risk factor was smoking (40.7%) followed by hypertension (20.3%) and dyslipidemia (15.3%). The most common complication was arrhythmias (24.65%) followed by recurrent ischemia (12.3%). Most (78.7%) received thrombolysis. In hospital, death was 9.3%. Conclusion: In young acute ST elevation myocardial infarction, smoking is the most important risk factor. These patients have better outcome and prognosis. Keywords: Acute ST elevation myocardial infarction, arrhythmias, smoking, young
How to cite this article:
Vaidya CV, Majmudar DK. A study of acute ST elevation myocardial infarction in young patients from government teaching hospital. Sudan Med Monit 2015;10:45-9 |
| Introduction | |  |
Coronary artery disease (CAD) is the major reason of morbidity and mortality burden in the world. Young patients with CAD are a specific subset of patients. The cut-off age of 45 has been used in most studies to define young patients with CAD and myocardial infarction (MI). [1] Although uncommon entity, it constitutes an important problem for the patient and the treating physician because of the devastating effect of this disease on more active lifestyle of young adults. In addition, these patients have different risk factor profiles, and prognosis than older patients. [2],[3] The clinical presentation is also different from that of older patients. Studies [4],[5],[6],[7] have described the clinical profiles and outcomes of young adults with acute MI (AMI) and its incidence ranged between 2% and 10%. The most common among all acute coronary syndrome (ACS) patients is acute ST elevation MI in India. [8] In general, young patients are more likely to be male, have a history of smoking and hyperlipidemia but less likely to have other comorbidities and demonstrate less extensive CAD on coronary angiogram. The mean age of ACS presentation in India was estimated to be 57.5 years [8] which is 7-11 years younger than reports from the Western literature. [9] Effective screening, evaluation, and management strategies for coronary heart disease (CHD) are well-established in high-income countries, but these strategies have not been fully implemented in India. CHD prevalence appears to be worsening in India. In developing countries, rates are predicted to increase by 120% in women and 137% in men from 1990 to 2020. [10] We did this study to know the clinical profile of young patients (≤45 years) with acute ST elevation myocardial infarction in our hospital by which we can help young physicians to deal with this deadly disease in young patients.
| Subjects and Methods | | |
This is a retrospective study of 73 cases managed for acute ST elevation Myocardial Infarction in young patients (≤45 years) in the ICCU of GMERS Medical College and General Hospital, Gandhinagar, Gujarat from January 1, 2012 to December 31, 2013. Due to ethical committee, permission was taken to retrieve case notes of the patients from the medical record department of the hospital and relevant data extracted and analyzed. For further intervention, we have to send patients to higher cardiac centers. All patients of age (≤45 years) and having the following two criteria out of three were included in the study. [11]
- Typical symptoms (chest discomfort)
- Typical pattern of electrocardiography (ECG) (ST segment elevation of ≥0.1 mV in at least two consecutive leads)
- Elevated enzyme levels (serum CPK-MB 2 times the upper limit of normal level).
The data obtained were analyzed using SPSS version 21.0 (IBM) software. Results were expressed in frequencies and percentages.
| Results | | |
Seventy-three cases of acute ST elevation MI cases records managed in ICCU of GMERS Medical College and Government Hospital, Gandhinagar during a period of January 1, 2012 to December 31, 2013 who were ≤45 years of age (young) were studied for clinical presentation, risk factors, complications, infarct type as per ECG findings management and outcome.
Frequency and percentage of cases in young
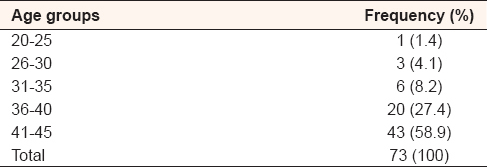
Totally, 73 patients ≤45 years of age were there. The age range in young age patients was from 25 years to 45 years with mean age of 40.95 years. In this study, the youngest patient was 25 years of age. Majority of the patients (58.9%) were from 41 to 45 years age group followed by (27.4%) who were in age group 36-40 and (8.2%) were in 31-35 years, (4.1%) in 26-30 and 1 case in age group 20-25 years. [Table 1] shows frequency and percentage of cases according to age groups.
Sex distribution of acute ST elevation myocardial infarction in young patients
In young MI, the majority were male patients, there were 65 (89%) males and 8 (11%) females. Male to female ratio was 8.1:1. [Table 2] shows sex distribution and percentage of it in young patients. As shown in [Table 3], maximum number of males (54.8%) were in age group 41-45, followed by (20.5%) in 36-40, (8.2%) in 31-35 years age group. Maximum number of females (6.8%) were from age group 36 to 40 years, followed by (4.1%) in 41-45 age group.
Clinical features of young patients with acute ST elevation myocardial infarction
In our study, the most common clinical presentation was chest pain (97.3%) followed by sweating (11%), vomiting and or nausea (8.2%), and breathlessness (6.8%). [Table 4] shows clinical features in patients.
Duration of chest pain before arrival to hospital
In our study, most of the patients with young MI (65.8%) arrived in hospital within 6 h from the onset of symptoms, followed by (21.9%) beyond 6 h and (12.3%) in less than an hour. [Table 5] shows the distribution of arrival time to hospital from the onset of symptoms in patients.
Area of involvement as per electrocardiography findings
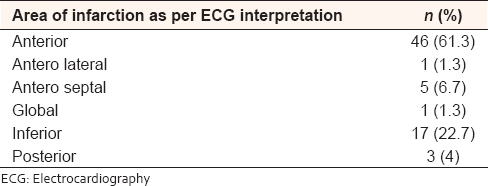
In our study, the most common area of infarction was anterior wall (61.3%) followed by inferior wall (22.7%), anteroseptal wall (6.7%), posterior (4%), and equal percentage of anterolateral, global with 1.3%. [Table 6] shows the area of infarction according in young patients.
Risk factors contributing to acute ST elevation myocardial infarction
In our study in young patients, most common risk factor was smoking or any form of tobacco consumption (40.7%) followed by hypertension (20.3%), dyslipidemia (15.3%), diabetes (11.9%), history of previous CAD (10.2%), and alcohol intake (1.7%). [Table 7] shows risk factors in patients.
Complications in patients presented with acute ST elevation myocardial infarction
In our study, the most common complication in young patients was arrhythmias (24.65%) followed by recurrent ischemia (12.3%), cardiogenic shock (10.9%) congestive cardiac failure (1.3%). [Table 8] shows complications in young patients. Maximum (64.3%) were without complications.
Thrombolysis of admitted patients
In our study, maximum numbers (78.7%) of young patients were thrombolysed and only 18.7% were not thrombolysed either because of late presentation or contraindication or complication [Table 9].
Outcome of patients
In our study, 48% of young patients were discharged. From our hospital, we have to send patients to higher cardiac center if they require further intervention, so 38.7% patients were referred to the higher cardiac center for further intervention, 9.3% patients died in hospital [Table 9].
| Discussion | | |
In our study, mean age of presentation was 40.95 years. In a study by Wong et al., [12] similar finding was there in study on Indian subgroup, where mean age was 39.9. In a study by Al-Khadra et al., [13] mean age was 40 years. In a study by Goornavar et al., [14] it was 36 years of age. In a study by Sricharan et al., [15] mean age was 37.03 years. Majority of the patients (86.3%) were from 36 to 45 years age group. In a study by Goornavar et al., [14] maximum (56.1%) were from 36 to 40 years age group. In a study by Sricharan et al., [15] majority (70%) were from 35 to 40 years age group. In this study, very less (5.4%) patients were below 30 years. It correlates with a study by Sricharan et al., [15] in which 3.33% were below 30. In a study by Tamrakar et al., [16] only (4.3%) patients were below 30 years of age. In our study, youngest age was 25 years of age which was higher age as compared to other studies. [17],[18] In India, youngest reported the age of AMI was 14 years. In young MI, majority were male patients, there were 65 (89%) males and 8 (11%) females. Male to female ratio was 8.1:1. In a study by Wong et al., [12] there were 94% males with very high 33.3:1 male to female ratio in Indian subgroup. In a study by Goornavar et al., [14] 95.4% were males and 4.5% were females. In a study by Sricharan et al., [15] 90% were males. In a study by Tamrakar et al., [16] 74% were males and 26% were females. In this study, 11% were females which were on higher side and was comparable with Italian [17] and USA [5] study in which females were 8% and 19%, respectively. In a study by Wadia and Nisal, [19] male to female ratio was 8:1 which was identical in our study.
In our study, the most common clinical presentation was chest pain (97.3%) followed by sweating (11%), vomiting and/or nausea (8.2%), and breathlessness (6.8%). This similar trend was seen in study by Al-Khadra et al., [13] Chest pain was the commonest symptom in 93.8% of the patients, followed by sweating in 69.2%, shortness of breath in 38.5%, shoulder pain in 33.6%, nausea and/or vomiting in 32.8%. In a study by Sricharan et al., [15] most common clinical feature was chest pain (90%) followed by sweating (50%) and breathlessness (20%).
In our study, most of the patients with young MI (65.8%) arrived in hospital within 6 h from the onset of symptoms, followed by (21.9%) beyond 6 h and (12.3%) in less than an hour. This was seen in a study by Bhatia et al., [20] in which maximum (72%) patients reached within 6 h of onset of symptoms. In a study by Suryadiparadja et al., [21] similarly majority young patients (50.76%) reached within 6 h of symptoms onset.
In our study, the most common area of infarction was anterior wall (61.3%) followed by inferior wall (22.7%) and anteroseptal wall (6.7%). In a study by Al-Khadra et al., [13] the most common area of infraction was anterior than inferior (55.4% vs. 44.6%), respectively. A similar trend was seen in study by Goornavar et al., [14] the most common area of infraction was anterior than inferior (75% vs. 25%), respectively. In a study by Sricharan et al., [15] 2/3 were having anterior and 1/3 having inferior. In a study by Tamrakar et al., [16] the most common area of infraction was anterior than inferior (50.47% vs. 33.9%), respectively.
In our study, in young patients, the most common risk factor was smoking or any form of tobacco consumption (40.7%) followed by hypertension (20.3%), dyslipidemia (15.3%), diabetes (11.9%). In a study by Al-Khadra et al., [13] most common risk factor was smoking (76.9%), dyslipidemia (33.8%), and hypertension (18.5%). In a study by Goornavar et al., [14] the most common risk factor was smoking (77.2%), dyslipidemia (54.5%), and hypertension (45%). In a study by Sricharan et al. [15] and Tamrakar et al., [16] the most common risk factor was smoking (70% vs. 64.3%), respectively. A study by Zimmerman et al. [4] found that among AMI patients <40 years old 73% to 90% reported a history of smoking. Many other studies have also found high rates of tobacco use among young patients who have AMI, with percentages ranging from 70% to >90%. [6],[22],[23] Smoking is known to cause increased fibrinogen concentrations and platelet aggregability, along with impaired fibrinolytic activity, decreased coronary flow reserve, and increased vasospasm. [24],[25],[26] Recurrent exposure to cigarettes with subsequent catecholamine surges damage endothelial cells, leading to endothelial dysfunction and injury of the vascular intima. Autopsy studies in young adults have showed that the extent of fatty streak lesions in the coronary arteries of young adults was higher in smokers than in nonsmokers. [27] All these evidence point out smoking as the most important modifiable risk factor in young adults.
In our study, the most common complication in young patients was arrhythmias (24.65%) followed by recurrent ischemia (12.3%), cardiogenic shock (10.9%). Maximum (64.3%) were without complications. It correlates with study by Wong et al., [12] in which the most common complication was arrhythmias (7.2%) followed by cardiogenic shock (4.5%). A similar trend was seen in study by Woon and Nisal, [28] in which 62.5% were without complications followed by 22.3% incidence of arrhythmias. In a study by Holay et al., [29] the most common complication was cardiac failure followed by arrhythmias (37.5%). In our study, unlike studies by Woon and Nisal, [28] and Holay et al., [29] only 1 case with cardiac failure was there, possible explanation could be early arrival in 6 h of onset of symptoms and prompt thrombolysis, no previous h/o coronary disease so good coronary reserve, all these will have positive outcome in young patients.
In our study, maximum numbers (78.7%) of young patients were thrombolysed and only (18.7%) were not thrombolysed. This was seen in study by Bhatia et al., [20] in which 44 (63.77%) out of 69 young patients with AMI received thrombolysis. In our study, 9.3% patients died in hospital. It correlates with study by Al-Khadra et al., [13] Bhatia et al., [20] Suryadipradja et al., [21] and Holay et al., [29] in which it was (9.2% vs. 8.6% vs. 12.94% vs. 12.5%), respectively.
| Conclusion | | |
The mean age of presentation was 40.95 years with male predominance, and male to female ratio was 8.1:1. Majority of the patients were from 36 to 45 years age group. The most common clinical presentation was chest pain followed by sweating and vomiting and/or nausea. Most of the patients with young MI (65.8%) arrived in hospital within 6 h from the onset of symptoms. The most common area of infarction was anterior wall followed by inferior wall and anteroseptal wall. The most common risk factor was smoking followed by hypertension (20.3%) and dyslipidemia. The most common complication in young patients was arrhythmias followed by recurrent ischemia and cardiogenic shock. Most of the young patients were thrombolysed. In hospital, mortality was 9.3%.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
| References | | |
| 1. | Egred M, Viswanathan G, Davis GK. Myocardial infarction in young adults. Postgrad Med J 2005;81:741-5.  |
| 2. | Chouhan L, Hajar HA, Pomposiello JC. Comparison of thrombolytic therapy for acute myocardial infarction in patients aged <35 and >55 years. Am J Cardiol 1993;71:157-9. |
| 3. | Hoit BD, Gilpin EA, Henning H, Maisel AA, Dittrich H, Carlisle J, et al. Myocardial infarction in young patients: An analysis by age subsets. Circulation 1986;74:712-21. [ PUBMED] |
| 4. | Zimmerman FH, Cameron A, Fisher LD, Ng G. Myocardial infarction in young adults: Angiographic characterization, risk factors and prognosis (Coronary Artery Surgery Study Registry). J Am Coll Cardiol 1995;26:654-61. |
| 5. | Kanitz MG, Giovannucci SJ, Jones JS, Mott M. Myocardial infarction in young adults: Risk factors and clinical features. J Emerg Med 1996;14:139-45. |
| 6. | Choudhury L, Marsh JD. Myocardial infarction in young patients. Am J Med 1999;107:254-61. |
| 7. | Ismail J, Jafar TH, Jafary FH, White F, Faruqui AM, Chaturvedi N. Risk factors for non-fatal myocardial infarction in young South Asian adults. Heart 2004;90:259-63. |
| 8. | Xavier D, Pais P, Devereaux PJ, Xie C, Prabhakaran D, Reddy KS, et al. Treatment and outcomes of acute coronary syndromes in India (CREATE): A prospective analysis of registry data. Lancet 2008;371:1435-42. [ PUBMED] |
| 9. | Budaj A, Brieger D, Steg PG, Goodman SG, Dabbous OH, Fox KA, et al. Global patterns of use of antithrombotic and antiplatelet therapies in patients with acute coronary syndromes: Insights from the Global Registry of Acute Coronary Events (GRACE). Am Heart J 2003;146:999-1006. |
| 10. | Murray CJ, Lopez AD. Alternative projections of mortality and disability by cause 1990-2020: Global burden of disease study. Lancet 1997;349:1498-504. |
| 11. | Antman EM, Braunwald E. ST elevation myocardial Infarction: Pathology, pathophysiolgy and clinical features. Braunwald's Heart Disaease: A Textbook of Cardiovascular Medicine. 9 th ed. Philadelphia: Saunders; 2011. |
| 12. | Wong CP, Loh SY, Loh KK, Ong PJ, Foo D, Ho HH. Acute myocardial infarction: Clinical features and outcomes in young adults in Singapore. World J Cardiol 2012;4:206-10. |
| 13. | Al-Khadra AH. Clinical profile of young patients with acute myocardial infarction in Saudi Arabia. Int J Cardiol 2003;91:9-13. |
| 14. | Goornavar SM, Pramiladevi R, Biradar Satish B, Sangamesh M. Acute myocardial infarction in young. J Pharm Biomed Sci 2011;8:1-5. |
| 15. | Sricharan KN, Rajesh S, Rashmi K, Meghana HC, Badiger S, Mathew S. Study of acute myocardial infarction in young adults: Risk factors, presentation and angiographic findings. J Clin Diagn Res 2012;6:257-60. |
| 16. | Tamrakar R, Bhatt YD, Kansakar S, Bhattarai M. Acute myocardial infarction in young adults: Study of risk factors. Angiographic features and clinical outcome. Nepal Heart J 2013;10:12-6. |
| 17. | Imazio M, Bobbio M, Bergerone S, Barlera S, Maggioni AP. Clinical and epidemiological characteristics of juvenile myocardial infarction in Italy: The GISSI experience. G Ital Cardiol 1998;28:505-12. |
| 18. | Siwach SB, Singh H, Sharma D, Katyal VK. Profile of young acute myocardial infarction in Harayana. J Assoc Physicians India 1998;46:424-6. |
| 19. | Wadia KS, Nisal JS. Precocious coronary artery disease. J Assoc Physicians India 1973;21:497-80. |
| 20. | Bhatia LC, Naik RH. Clinical profile of acute myocardial infarction in elderly patients. J Cardiovasc Dis Res 2013;4:107-11. |
| 21. | Suryadipradja M, Dewabrata W, Harun S, Alwi I, Hakim L, Effendy S, et al. Clinical manifestation of acute myocardial infarction in the elderly. Med J Indones 2003;12:229-35. |
| 22. | Hong MK, Cho SY, Hong BK, Chang KJ, Mo-Chung I, Hyoung-Lee M, et al. Acute myocardial infarction in the young adults. Yonsei Med J 1994;35:184-9. |
| 23. | Adhikari CM, Rajbhandari R, Limbu YR, Malla R, Sharma R, Rauniyar B, et al. A study on major cardiovascular risk factors in acute coronary syndrome (ACS) patient 40 years and below admitted in CCU of Shahid Gangalal National Heart Center. Nepal Heart J 2010;7:20-4. |
| 24. | Panduranga P, Sulaiman K, Al-Zakwani I, Abdelrahman S. Acute coronary syndrome in young adults from Oman: Results from the gulf registry of acute coronary events. Heart Views 2010;11:93-8. [ PUBMED]  |
| 25. | Lang NN, Gudmundsdóttir IJ, Boon NA, Ludlam CA, Fox KA, Newby DE. Marked impairment of protease-activated receptor type 1-mediated vasodilation and fibrinolysis in cigarette smokers: Smoking, thrombin, and vascular responses in vivo. J Am Coll Cardiol 2008;52:33-9. |
| 26. | Morita K, Tsukamoto T, Naya M, Noriyasu K, Inubushi M, Shiga T, et al. Smoking cessation normalizes coronary endothelial vasomotor response assessed with 15O-water and PET in healthy young smokers. J Nucl Med 2006;47:1914-20. |
| 27. | Berenson GS, Srinivasan SR, Bao W, Newman WP 3 rd , Tracy RE, Wattigney WA. Association between multiple cardiovascular risk factors and atherosclerosis in children and young adults. The Bogalusa Heart Study. N Engl J Med 1998;338:1650-6. |
| 28. | Woon VC, Lim KH. Acute myocardial infarction in the elderly - The differences compared with the young. Singapore Med J 2003;44:414-8. |
| 29. | Holay MP, Janbandhu A, Javahirani A, Pandharipande MS, Suryawanshi SD. Clinical profile of acute myocardial infarction in elderly (prospective study). J Assoc Physicians India 2007;55:188-92. |
[Table 1], [Table 2], [Table 3], [Table 4], [Table 5], [Table 6], [Table 7], [Table 8], [Table 9]
|









 Search Pubmed for
Search Pubmed for