|
 
 |
| CASE REPORT |
|
| Year : 2015 | Volume
: 10
| Issue : 2 | Page : 69-71 |
|
Congenital bilateral anophthalmia: A case report and review of the literature
Ibrahim Aliyu, Safiya Gambo, Peter David Igoche
Department of Paediatrics, Aminu Kano Teaching Hospital, Bayero University, Kano, Nigeria
| Date of Web Publication | 16-Jul-2015 |
Correspondence Address:
Dr. Ibrahim Aliyu
Department of Paediatrics, Aminu Kano Teaching Hospital, Bayero University, Kano
Nigeria
  | Check |
DOI: 10.4103/1858-5000.160954 
Anophthalmia is congenital absence of the eyes; it may be unilateral or bilateral. Though rare, it occurs worldwide. It usually occurs in association with other systemic malformations particularly cardiac, musculoskeletal and central nervous system abnormalities. Therefore, the case of a female child delivered in our facility who was subsequently admitted into the special care baby unit on account of respiratory distress and bilaterally absent eyes is reported. She had ocular and brain computer tomography scan that showed under development of both globes and hypogyria; chest X-ray showed bilateral patchy opacities only, electrocardiography and abdominal ultrasound scan were normal while echocardiography revealed trivial tricuspid regurgitation with shunt lesions: Perimembranous ventricular septal defect of 5.4 mm and a secundum atrial septal defect of 5 mm. She is followed-up in both the ophthalmology and pediatric cardiology clinics. Keywords: Anophthalmia, congenital heart disease, microphthalmia
How to cite this article:
Aliyu I, Gambo S, Igoche PD. Congenital bilateral anophthalmia: A case report and review of the literature. Sudan Med Monit 2015;10:69-71 |
| Introduction | |  |
The term anophthalmia refers to the absence of ocular tissue. [1] It is closely linked and suggested to represent a phenotypic continuum with microphthalmia [1] in which the eyes are rudimentary or hypoplastic with the ocular diameter usually <10 mm and the posterio-anterior diameter of the globe been <20 mm. [2] These are abnormalities in the development of the primary optic vesicle. [3]
Anophthalmia is a rare anomaly with an estimated incidence of 3 per 1000 live births. [4],[5] In Sweden, a prevalence of 0.2-0.4 per 10,000 live births was reported. [6] In Benin city Nigeria, Ukponmwan [7] reported only two cases seen over a 20 year period. In Enugu, Southeastern Nigeria, anophthalmia represented only 9.3% of congenital eye anomalies seen over an 8 year period. [8] Earlier studies in Kano documented anophthalmia and microphthalmia to be less common congenital eye anomalies; [9],[10] however, their association with cardiac defects were not established in those reports.
Although anophthalmia may occur as unilateral or bilateral lesion, [11] it is most often bilateral. [12] It may occur in isolation or as part of a syndrome. [1] It usually occurs in association with other systemic malformations particularly involving cardiac, musculoskeletal and central nervous system. [13]
Its etiology is diverse with chromosomal, monogenic and environmental factors being implicated. [1] Advanced maternal age, [12] multiple births, [12] low birth weight, infections such as toxoplasmosis, rubella, cytomegalovirus, varicella virus, parvovirus, influenza virus and coxsackievirus have been implicated. [12]
The disease occurs equally in both sexes. [1],[12] Diagnosis is usually clinical, following a complete ophthalmologic examination that demonstrates the complete absence of the globe. Imaging tests confirm the diagnosis as well as excluding other associated systemic anomalies. Ultrasonography detects anophthalmia from early second trimester and trans-vaginal ultrasonography may provide better and earlier diagnosis. [13] Treatment is directed to the improvement of cosmesis. [1]
We, therefore, report a case of a female child who was delivered with bilateral anophthalmia and associated cardiac malformations in our facility.
| Case Report | | |
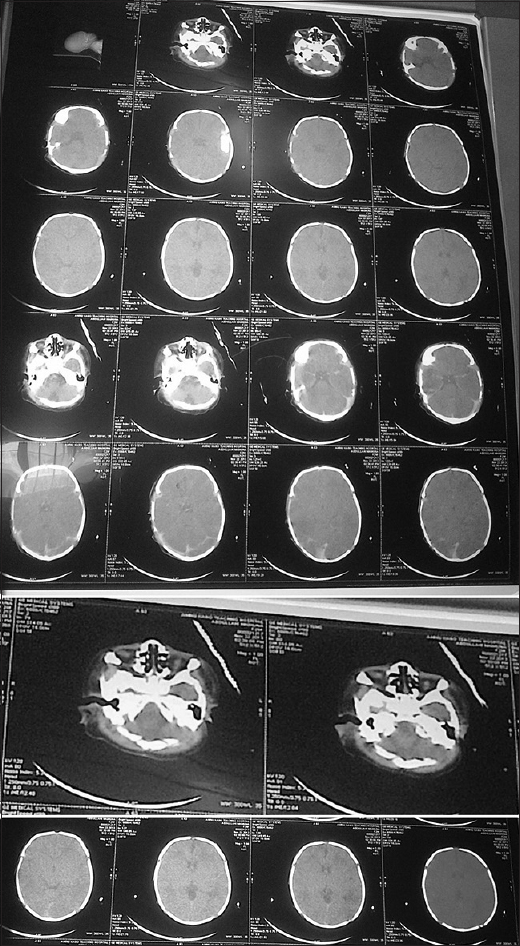
A 2-month old female child who was first seen within an hour of delivery in our facility and was subsequently admitted into the special care baby unit on account of the respiratory distress and bilaterally absent eyes. She was delivered at term to a 20-year-old mother via spontaneous vertex delivery. Delivery was uneventful, and Apgar score was 7 and 9 in the 1 st and 5 th min respectively. The mother had antenatal care in the same hospital. She was regular and complaint to all her antenatal medications and investigations including ultrasonography, all of which were normal. Prenatal period was free of adverse events. No history of fever, body rashes, use of traditional concoctions or nonprescribed medications and no exposure to X-rays. The mother was not a known hypertensive or diabetic. The father was a 30-year-old banker. There was no family history of the similar problem among siblings or relations. The union was consanguineous. On examination, the baby had a normal birth weight of 2.7 Kg, was not cyanosed, and had small palpebral fissures and the eyeballs were not discernible [Figure 1]. There was no other obvious anomaly. Other systems were normal. She had an extensive eye examination by the ophthalmologists who made a diagnosis of bilateral anophthalmia. The diagnosis was confirmed with an ocular computer tomography (CT) scan that showed under development of both globes within the orbit with a conclusion of bilateral anophthalmia; a brain CT also showed hypogyria [Figure 2]. Chest X-ray and abdominal ultrasound scan were normal. An echocardiography revealed trivial tricuspid regurgitation with shunt lesions: Perimembranous ventricular septal defect (VSD) of 5.4 mm and a secundum atrial septal defect (ASD) of 5 mm. The patient did well on admission and was discharged. Patient was followed-up in the cardiology clinic and was placed on diuretics. She was subsequently admitted in the emergency pediatrics unit on account of bronchopneumonia with heart failure. She improved on antibiotics and was discharged home, and her parents were properly counseled. She is being followed up in both the ophthalmology and pediatric cardiology clinics.
| Discussion | | |
Our patient presented with bilateral anophthalmia, trivial tricuspid regurgitation, an ASD with VSD. The defect is often bilateral, [12] similar to that in our patient. This is similar to the findings of Spear et al.[14] but contrasted with the two cases reported in Benin Nigeria, which were unilateral involvement. [7]
Shunt lesions had been observed as the cardiac components in this condition. Priolo et al. [15] documented an associated ASD while Spear et al. [14] reported a VSD. Other common cardiac anomalies associated with it are single left ventricle, tetralogy of Fallot, hypoplastic left ventricle, pulmonary valve atresia and bicuspid aortic valve.
Maternal age of 20 years observed in our patient is not in keeping with the significant association of the disease with advanced maternal age. [1],[12]
Although anophthalmia is closely linked to genetic and familial causes, [1] our patient had no family history of similar problem. Ng et al. [16] reported anophthalmia, lung hypoplasia and cardiac anomaly in two siblings whose first cousins had microphthalmia. Similarly, Benezra et al. [17] reported the presence of bilateral anophthalmia and unilateral microphthalmia in two siblings. This further supports the strong association between anophthalmia and micropthalmia. [1] Furthermore, our patient was a product of a consanguineous union that makes an autosomal recessive mode of inheritance plausible; similar observation had been reported by previous authors. [16],[17]
Our patient's condition was diagnosed after birth and antenatal ultrasonography failed to pick the anomaly. This may support the argument of other authors that ultrasonography may be unremarkable in the diagnosis of this defect; though we recognize the fact that ultrasound is operator dependent. However, better antenatal diagnosis of this condition reported by other authors may suggest lack of sophisticated equipment and laboratory support typical of our resource constraint setting. Unfortunately, chromosomal/genetic analysis was not done in our patient.
| Conclusion | | |
The paucity of data in our environment may undermine the contribution of such rare anomalies to childhood morbidity and mortality. The co-existence of anophthalmia with cardiac abnormalities is not uncommon. Therefore, a need for careful evaluation of such patients in other to pick associated anomalies which enables prompt institution of appropriate management measures is warranted.
| References | | |
| 1. | Verma AS, Fitzpatrick DR. Anophthalmia and microphthalmia. Orphanet J Rare Dis 2007;2:47.  |
| 2. | International Clearinghouse for Birth Defects Monitoring Systems. International Centre on Birth Defects: Annual Report; 2003. |
| 3. | Ragge NK, Subak-Sharpe ID, Collin JR. A practical guide to the management of anophthalmia and microphthalmia. Eye (Lond) 2007;21:1290-300. |
| 4. | Morrison D, FitzPatrick D, Hanson I, Williamson K, van Heyningen V, Fleck B, et al. National study of microphthalmia, anophthalmia, and coloboma (MAC) in Scotland: Investigation of genetic aetiology. J Med Genet 2002;39:16-22. |
| 5. | Campbell H, Holmes E, MacDonald S, Morrison D, Jones I. A capture-recapture model to estimate prevalence of children born in Scotland with developmental eye defects. J Cancer Epidemiol Prev 2002;7:21-8. |
| 6. | Källén B, Tornqvist K. The epidemiology of anophthalmia and microphthalmia in Sweden. Eur J Epidemiol 2005;20:345-50. |
| 7. | Ukponmwan CU. Congenital anophthalmos in Benin City, Nigeria. West Afr J Med 1999;18:141-3. |
| 8. | Chuka-Okosa CM, Magulike NO, Onyekonwu GC. Congenital eye anomalies in Enugu, South-Eastern Nigeria. West Afr J Med 2005;24:112-4. |
| 9. | Olatunji FO, Kirupananthan S, Ayanniyi AA, Abuh S. Causes of childhood blindness at ECWA Eye Hospital, Kano, Nigeria. Afr J Med Med Sci 2009;38:29-32. |
| 10. | Lawan A. Congenital eye and adnexial anomalies in Kano, a five year review. Niger J Med 2008;17:37-9. |
| 11. | Tucker S, Jones B, Collin R. Systemic anomalies in 77 patients with congenital anophthalmos or microphthalmos. Eye (Lond) 1996;10:310-4. |
| 12. | Källén B, Robert E, Harris J. The descriptive epidemiology of anophthalmia and microphthalmia. Int J Epidemiol 1996;25:1009-16. |
| 13. | Mashiach R, Vardimon D, Kaplan B, Shalev J, Meizner I. Early sonographic detection of recurrent fetal eye anomalies. Ultrasound Obstet Gynecol 2004;24:640-3. |
| 14. | Spear GS, Yetur P, Beyerlein RA. Bilateral pulmonary agenesis and microphthalmia. Am J Med Genet Suppl 1987;3:379-82. |
| 15. | Priolo M, Casile G, Laganà C. Pulmonary agenesis/hypoplasia, microphthalmia, and diaphragmatic defects: Report of an additional case. Clin Dysmorphol 2004;13:45-6. |
| 16. | Ng WY, Pasutto F, Bardakjian TM, Wilson MJ, Watson G, Schneider A, et al. A puzzle over several decades: Eye anomalies with FRAS1 and STRA6 mutations in the same family. Clin Genet 2013;83:162-8. |
| 17. | Benezra D, Sela M, Péer J. Bilateral anophthalmia and unilateral microphthalmia in two siblings. Ophthalmologica 1989;198:140-4. |
[Figure 1], [Figure 2]
|










 Search Pubmed for
Search Pubmed for