|
 
 |
| ORIGINAL ARTICLE |
|
| Year : 2016 | Volume
: 11
| Issue : 3 | Page : 71-77 |
|
Tuberculosis in Sudan: Efficiency of diagnostic techniques commonly used and investigation of some sociodemographic factors which may influence the disease prevalence
Mohammed Sirelkhatim1, Ghada Sulieman Sharaf Eldin2, Imad Fadl Almula2, Ahmed Babiker2, Rihab Ali Omer1
1 Department of Microbiology and Bio-molecular Technology, National University Research Institute, National University, Khartoum, Sudan
2 Faculty of Medicine, Al Neelain University, Khartoum, Sudan
| Date of Web Publication | 31-Aug-2016 |
Correspondence Address:
Mohammed Sirelkhatim
National University Research Institute, P. O. BOX: 3783, Khartoum
Sudan
  | Check |
DOI: 10.4103/1858-5000.189559 
Introduction: Tuberculosis (TB) is a bacterial disease that can be spread through the air. It usually attacks the lungs, but it can also attack and damage the other parts of the body such as the brain, kidneys, or spine. The disease remains to be a major health problem in countries suffering from poverty and unsettlement like Sudan. Materials and Methods: In this study, sputum samples were collected from 243 patients (186 males and 57 females) being suspected of pulmonary TB. The patients were distributed in TB specialized clinics in different areas of Central (Khartoum), Eastern (Port Sudan), and Western (Al Obeid) parts of Sudan after they have been informed and agreed to participate in the study. Age, sex, and social status including occupation and housing of the patients were recorded. The patients' common complaints were cough, fatigue, chest pain, shortness of breath, loss of weight, and hemoptysis. Samples were collected, treated with 4% NaOH, and examined both microscopically after having them stained with Ziehl-Neelsen (ZN) stain and microbiologically having them cultured on Lowenstein-Jensen (LJ) media. Isolates were further identified using biochemical tests and resistance to anti-TB drugs was determined. 85.2% (207/243) shown acid-fast bacilli in ZN stain whereas 78.6% (191/243) were positive for mycobacteria in culture. 149 (75%) were successfully subcultured in LJ media and confirmed to be Mycobacterium tuberculosis using biochemical tests. Results: Of 149 isolated M. tuberculosis species, 18.1% (27), 32.9% (49), 20.7% (31), and 22.4% (33) were resistant to isoniazid, streptomycin, rifampicin, and ethambutol, respectively. Conclusion: This study highlights the presence of yet-unknown species of mycobacterium causing active infection with TB in patients in Sudan and the presence of a high percentage of drug resistance which knocks in the alarm of having multidrug-resistant TB circulating in Sudan, a country with many suitable predisposing factors for the disease. Keywords: Drug resistance, identification, prevalence, Sudan, tuberculosis
How to cite this article:
Sirelkhatim M, Eldin GS, Almula IF, Babiker A, Omer RA. Tuberculosis in Sudan: Efficiency of diagnostic techniques commonly used and investigation of some sociodemographic factors which may influence the disease prevalence. Sudan Med Monit 2016;11:71-7 |
How to cite this URL:
Sirelkhatim M, Eldin GS, Almula IF, Babiker A, Omer RA. Tuberculosis in Sudan: Efficiency of diagnostic techniques commonly used and investigation of some sociodemographic factors which may influence the disease prevalence. Sudan Med Monit [serial online] 2016 [cited 2017 Feb 10];11:71-7. Available from: http://www.sudanmedicalmonitor.org/text.asp?2016/11/3/71/189559 |
| Introduction | |  |
Tuberculosis (TB) remains a major health problem in countries with low income. [1] It is considered as one of the most serious diseases and a considerable public health problem due to its high risk of person-to-person transmission, morbidity, and mortality. [2] It was reported that 8.9-9.9 million reported TB cases worldwide, most of them in Africa and Asia. [3]
Sudan is currently suffering from many factors which may predispose for the occurrence and increase of TB infection rates, among which are the civil war in some areas and displacement of people in a search of a better life. This may enhance the occurrence and spread of many health hazardous diseases, among them is TB. The other factors include poverty and lack of well-equipped medical centers that enable identification and treatment of TB in its earlier stage.
Hence, identification of epidemiological factors affecting the prevalence rates of TB is fundamental and crucial for decision-makers enabling them having the appropriate strategy to minimize the incidence of the disease and identifying the risk factors helping in its distribution.
The current study is a pilot study giving some information about the prevalence of TB in patients in different areas of the Sudan and collating that with some epidemiological factors as age, sex, social factors, and ethnic groups.
It also enables to compare between different diagnostic methods mostly used in a country like Sudan.
| Materials and Methods | | |
Study area
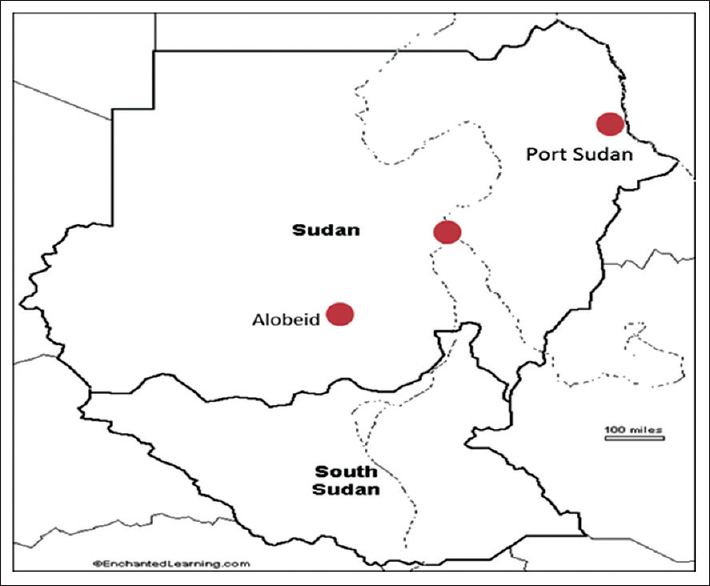
Patients included in the study were suspected TB patients in TB clinics in any of three cities located in different parts of the Sudan. These are Khartoum (Central), Port Sudan (Eastern), and Al Obeid (Western). These cities are the main centres in these mentioned regions where people from the nearby localities search advanced medical care [Figure 1].
Population
A total of 243 randomly selected patients (186 males, 57 females) were included in this study. 180 of them were from Khartoum (137 males, 43 females), 40 from Port Sudan (34 males, 6 females), and 23 from Al Obeid (15 males, 8 females). Study participants were enrolled 3 days per week.
Ethical approval
This study was ethically approved by Al Neelain Ethical Review Board, Khartoum, Sudan. All patients included in the study had agreed and signed to participate after being informed about the purpose of the study and the reason behind sampling.
Questionnaire
As a part of the study, a structured questionnaire including the following questions was answered by each patient for further epidemiological analysis: Age, sex, tribe (Ethnic), marital status, education, residence, type of housing (construction and number of persons), occupation, clinical symptoms with its duration, type of TB, and treatment.
Specimen processing and culture (Collection and examination of sputum)
Sputum samples were collected from each individual patient, decontaminated by adding a double volume of 4% sodium hydroxide. The pH of the mixture was brought to neutral by the addition of hydrochloric acid and phenol red as an indicator. Samples were then concentrated by centrifugation at 1500-2000 rpm for 20 min. Supernatants were discarded and a double volume of distilled water was added to sediment and centrifuged again for 5 min.
Ziehl-Neelsen smear and microscopy
Smears made from above-prepared specimens were air-dried, heat-fixed, and stained by the Ziehl-Neelsen (ZN) staining technique. The stained slides were examined under oil immersion (1000 × lens objective) and were reported negative when no acid-fast bacilli (AFB) were seen in at least 100 microscopic fields and were reported positive when at least 1-9 AFB were seen in 100 fields; the exact number recorded after examining 50 fields; 10-99 AFB/100 were recorded as 1+, 1-10 AFB/field recorded as 2+, more than 10 AFB/field after examining at least 20 fields was recorded as 3+. [4] All negative smears were rechecked.
Bacteriological investigation
The Lowenstein-Jensen (LJ) medium was prepared as follows: 37.4 g of LJ medium powder was dissolved in 600 ml distilled water and 12 ml glycerol was added to the solvent. The mixture was then autoclaved at 121°C for 15 min. A volume of 1000 ml homogenized egg mixture was added to the cool medium and the mixtures were then dispensed into McCartney bottles which were placed in a slanted position in the inspissator and coagulation occurred in 45 min at 80°C: After inspissations, all media bottles were incubated at 37°C to check sterility. Decontaminated sputum samples were inoculated in duplicate and incubated at 37°C and examined for growth twice weekly for the first 2 weeks and once weekly, thereafter up to 8 weeks after which a definite result was obtained. Cultures those showed no growth within 8 weeks were scored as "negative." A patient was defined as a TB-positive case if any of the two sputum specimens had a positive culture.
Smears from suspected growing colonies were fixed and stained with ZN stain to confirm the presence of AFB.
Biochemical tests
Catalase activity was tested at a temperature of 68°C and pH 7.0. In brief, two loops full of 14-day-old growth were suspended in 0.5 ml buffer solution in a screw-capped bottle and placed together with a negative control bottle in a water bath of a temperature of 68°C for 20 min and then cooled to room temperature. A volume of 0.5 ml freshly prepared tween peroxide was subsequently added. The appearance of bubbles indicates a positive catalase test.
For the nitrate test, 2 loops full of a 4-week-old growth were inoculated in one of two screw-capped bottles containing 2 ml of nitrate buffer while other bottle was used as a negative control. The contents of the bottle were mixed and incubated at 37°C for 2 h. After incubation, 1 drop of HCL, 2 drops of 0.2% sulfanilamide, and 2 drops of 0.1% N-naphthylethylenediamine were added. The solution was examined for the development of a pink/red color contrasting with the control. A pinch of zinc powder was added to the negative bottles to reduce nitrate to nitrite. The appearance of red color after this step confirms a negative reaction. [5]
Drug susceptibility testing (Proportion method)
Drug susceptibility testing of 149 isolates was done by conventional culturing on LJ media using the proportion method. [6] In brief, LJ media for drug susceptibility was prepared by adding 0.2 μg/ml, 40 μg/ml, 4 μg/ml, and 0.2 μg/ml of with each of isoniazid, rifampicin, streptomycin, and ethambutol consequently. Suspensions were prepared by transferring a full 10-μ loop of bacterial growth into suspension bottle containing sterile distilled water. The turbidity of the homogenized suspensions was adjusted to McFarland standard No. 1 by adding sterile distilled water. Two serial dilutions of the isolate suspensions (10−2 and 10−4 ) were prepared and inoculated in these media. Plain media were used as a control. The readings of the incubated samples were taken after 4 and 6 weeks. Resistance was calculated as the ratio of the number of colonies growing on the drug containing medium and those growing on the control media. An isolate was considered as resistant if the ratio between the growth in the media containing the critical concentration of the drugs and the growth in the control is greater or equal to 1%. [7]
| Results | | |
Age and sex distribution
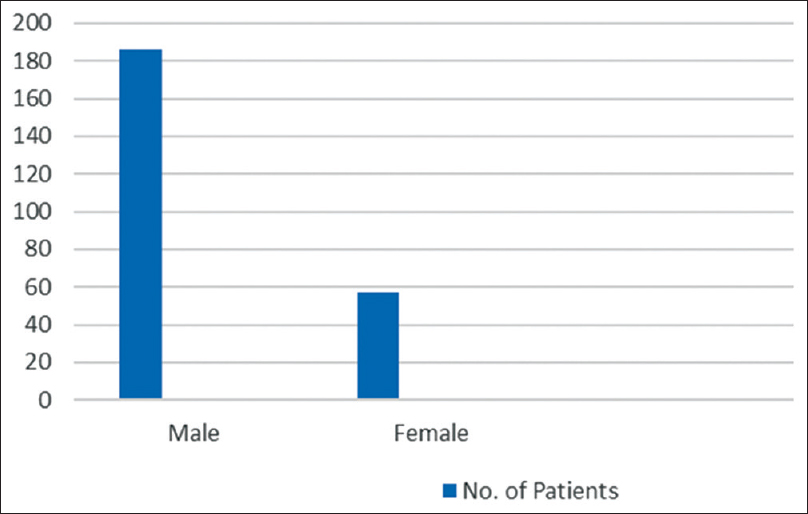
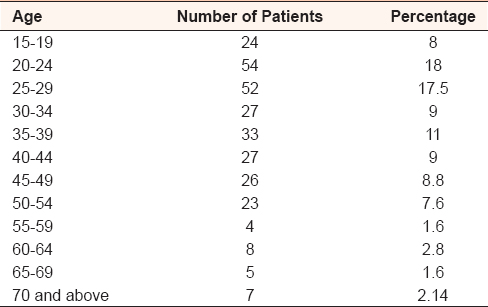
The age of the patients included in the study ranges from ≥15 to ≤70 years (mean 32.57± standard deviation [SD] 0.695, median 30± SD 13.499. More males than females were found to have TB (187:57) [Table 1] and [Figure 2].
Population study
In the study, the number of males was 186 (74.7%). Of them, 72 were workers (30.4%), 26 were farmers (10.7%), 30 were free workers (unskilled laborers) (12.3%), 27 were unemployed (11.9%), 16 were students (7%), 11 were drivers (4.9%), and 4 were soldiers (1.6%).
The number of females included in this study was 57 (25.3%). Of them, 35 were housewives (14.4%), 6 were female students (2.5%), 14 were workers (5.7%), and 2 were teachers (0.8%).
Marital status among the study subjects
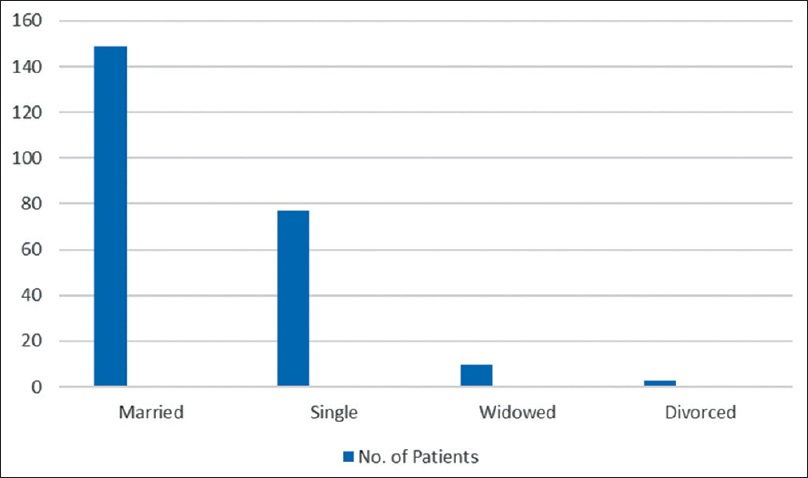
One hundred and forty-nine (61.5%) patients were married while 78 (31.8%) were single, 10 (4.0%) were widowed, and 7 (3%) were divorced [Figure 3].
Residence
The disease was found to be prevalent in all parts of Sudan. According to the residence of the patients, which was classified as urban and rural, 156 (64.1%) were urban and 87 (35.9%) were rural.
Type of housings
The participants of the study were found to live in different types of houses made of different building materials according to the area where they live. 34 (8.1%) of them live in houses made of concrete, 78 (32.1%) in houses built of bricks, 90 (37%) built of mud; the remaining houses were 35 (14.4%) Gutiya, 4 (1.0%) Birish, and 2 (0.5%) made of straw.
Education
Among the study population, 93 (38.3%) patients were illiterates and 18 (7.4%) went to khalwa while the educated vary in their education from primary to university. 66 (27.4%) had primary education, 8 (3.3%) stopped at the intermediate level, 48 (19.8%) had a secondary level of education while only 3 (1.1%) went to university.
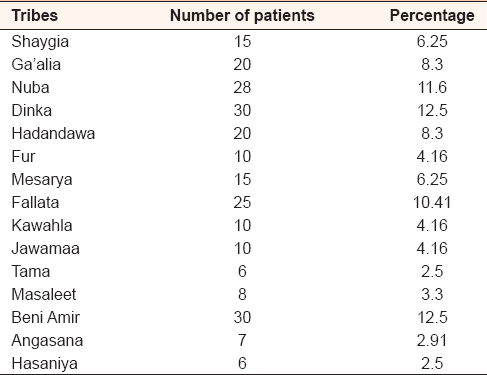
Ethnic groups
The patients belong to different tribes from different parts of Sudan. The highest number of the cases was Falata, Nuba, Dinka, and Beni Amir while the least incidence was in Hasaniya, Angsana, and Tama [Table 2].
Clinical symptoms
The patients' common complaints were cough, fatigue, headache, chest pain, shortness of breath, fever, loss of weight, and hemoptysis. The cough was the most common complaint.
Duration of clinical symptoms
The patients included in the study commonly complained of cough, fever, and shortness of breath. The duration of these symptoms varied from 6 weeks to 3 years.
Type of tuberculosis
Of the 243 subjects included in the study, 179 (74%) were new cases, 44 (18.1%) were relapses, 16 (6.5%) were patients with interrupted anti-TB treatment, and 4 (1.8%) were cases of failure of treatment.
Treatment
Of the study participants, 179 (74%) had no history of treatment while 64 (26%) received first-line anti-TB treatment.
Characterization of isolates
Microscopic results
Two hundred and forty-three sputum samples from TB patients included in the study were processed for staining using ZN stain and examined by the light microscope. 207 (85.2%) of them were positive showing AFB in ZN stain.
Results were recorded according to the WHO/IUATLD method of reporting ZN stain findings.
Culture results
Cultures of sputa from 191 of 243 pulmonary TB patients (78.6%) were positive for mycobacteria. 149 (75%) were successfully subcultured on LJ. 19 (13%) cultures were contaminated and only 149 isolates were used for biochemical identification and sensitivity testing.
Identification of isolates
Based on the morphology of the culture and results of the biochemical test, catalase, nitrate reduction, of 191 isolates, 149 (78.6%) isolates were Mycobacterium tuberculosis.
Biochemical analysis
Catalase test
Of 191 samples, 149 (78.6%) isolates showed negative result and were described as M. tuberculosis. All M. tuberculosis isolates were 68°C labile catalase negative.
Nitrate reduction test
Of 191 isolates, 149 (78.6%) isolates produced pink color (reduced nitrate to nitrite), which was an indication of a positive result. The positive result indicates that the isolate is M. tuberculosis. [8]
Resistance to first-line antituberculosis drugs
The drug susceptibility testing was performed on 149 strains (the successfully subcultured strains) using the proportional method. The result showed that resistance was as follows: Isoniazid 27 (18.1%), streptomycin 49 (32.95), rifampicin 31 (20.7%), and ethambutol 33 (22.4%) [Table 3].
Resistance within cases
Of the 149 successfully sub-cultured cases, 105 (71%) were new cases, 31 (20.7%) were relapses, 10 (6.5%) were cases of interrupted treatment, and 3 (1.8%) were failure to treatment [Table 4].
Multidrug-resistant strains of Mycobacterium tuberculosis (MDRMTB)
Of 149 isolated strains of M. tuberculosis, 13 (8.7%) were multidrug-resistant strains of M. tuberculosis. Six (6.1%) were isolated from new TB cases, five from relapse cases (15.1%), one from interrupted cases (6.7%), and 1 (20.0%) from cases of failure to treatment [Table 5].
| Discussion | | |
TB is among the most widely spread and serious of all human infectious diseases and there are more cases today than at any previous time in human history. [9] Despite the availability of many highly sensitive diagnostic tools and highly efficacious treatment for decades, the disease continues to be a major public health threat worldwide. It is more of a threat in developing countries. Sudan is currently suffering from poverty and social restlessness, which are factors that seriously affect the infection rates of the disease. The current study aimed at investigating the efficiency of diagnostic methods mostly used in Sudan. These are, namely, smear technique using ZN stain and culture technique using LJ media. Other factors that may play a role in the enhancement of infection include: Age, sex, and social status (occupation, housing, and residence of the patients) were considered. Resistance to anti-TB drugs was also determined.
For the purpose of the study, sputum samples were collected from 243 patients (186 males and 57 females) being confirmed of having any type of pulmonary TB (74% new, 18.1% relapsed, 6.5% patients with interrupted anti-TB treatment, and 1.8% were cases of treatment failure). The patients were distributed in three major cities in the central (Khartoum: 137 males, 43 females), Eastern (Port Sudan: 34 males, 6 females), and Western (Al Obeid: 15 males and 8 females) parts of Sudan. This distribution avails a large range of population that is living in areas having different types of climate and infrastructure facilities. Populations included in the study were in some TB specialized clinics and were either suspected of having or had a recurrent infection of TB and their common complaints were cough, fatigue, headache, chest pain, shortness of breath, loss of weight, and hemoptysis.
TB affects all age groups ranging from 15 to 70 years. The highest incidence rate was found among the age group of 25-30 years (18%) and the lowest was among the age group of 55-65 years (1.6%).
It was also found that the number of affected males constitutes 77% (186/243) of the patients. This may be attributed to the fact that males are mostly forced to work under hard conditions and are having insufficient nutrients in comparison with the females being mostly at home. This should even be considered having the fact that in our study, almost 40% of the patients (95/243) are single, divorced, or widowed and hence suffering from unstable social life. Gupta (Gupta et al., 2004) previously reported similar results; men (M:F = 3.7:1) PTB was significantly common in blue collar (44%) and white collar (27.1%) workers than household workers (12.1%). [10]
From the other hand, it was found that 64% (156/243) of the patients included in this study were from urban areas whereas 35% (87/243) from rural areas. This result does not reflect the real situation as many of the patients came from rural areas seeking better health care in big cities such as Khartoum and Port Sudan.
The participants of the study were found to live in different types of houses made of different building materials. Nevertheless, a majority of them (90) were living in houses made of mud. This is a reflection of a poor economic situation and lack of sanitation.
Among the study population, only 3 (1.1%) went to university in contrast to 93 (38.3%) illiterate patients. This again reflects the low economic level that most of the patients are suffering as it is usually in Sudan to have a positive relationship between the level of education and satisfying employment situation. This was clearly stated in this study as all of the participants were belonging to the low-income stratum of the society being categorized in one of these categories: Workers (47.6%), farmers (10%), unemployed (11.9%), housewives (14.4%), teachers (0.8%), and 1.6% soldiers. This finding agreed with other studies and this reveals the relationship between low income and TB. A WHO report at 2006 stated that TB is a disease associated to low socioeconomic conditions as in low-income people with large families crowded in poor housing conditions. [3]
No significant tribal differences were found although Abel and Casanova in 2000 [11] have proposed genetic predisposition to the disease.
| Conclusion | | |
This study showed that TB is spread all over Sudan. Different types of patients have been investigated, new TB cases (74%), relapses (18.1%), interrupted anti-TB treatment (6.5%), and failure to treatment (1.8%).
The results of the diagnosis using ZN stain and culture technique on LJ media were compared. 207 (85.2%) of the samples showed AFB in ZN stain whereas 191 of 243 pulmonary TB patients (78.6%) were positive for mycobacteria being cultured on LJ media. 149 isolates were used for biochemical identification and sensitivity testing.
DOTS strategy is adopted by the health authorities in Sudan for the diagnosis of pulmonary TB as recommended by the WHO. [12] Although this strategy is not demanding in its application (due to its simplicity), we have some preservations of using it as being the only method of TB diagnosis. Although in similar studies, [13] the results of positive LJ culture were more than positive results in ZN stain, in this study, the results were different: 78% gave positive results on LJ culture while 48% were positive on LJ stain. The cause is believed to lie in the quality of media that have been used and the method of preparation of the specimens for culture.
The media have been made locally in the laboratory, which certainly affect its quality and the concentration of the sodium hydroxide (4%) used for the decontamination of the samples may have affected the viability of mycobacterium in the samples.
This concentration has been used to assure proper decontamination of fast-growing normal flora found in the sputum although it is known that it might affect the growth of mycobacterium.
In similar studies, usually, commercially prepared media and automated machines such as Bac-Tek 490 and mycobacterial growth index tube of Becton Dickinson and other similar machines are used. This improves the growth of mycobacterium and gives better results in culture than in microscopy.
Culture is believed to be more sensitive and even more important as it provides the chance for checking drug sensitivity, which is increasing in importance due to the increase in the incidence of drug and multidrug resistance and even extensively drug resistance of mycobacterium.
The drug resistance to mycobacterium is a global problem. The problem is even worse in the developing countries as the rate of resistance is on the increase. Important factors are lack of resources leading to inefficient control programs, shortage of drug supplies and facilities for diagnosis, poor socioeconomic situations and poverty, and the emerging HIV/AIDS epidemic. [14]
Sudan is not an exception and resistance to anti-TB drugs has been reported by other studies (Hassan et al. 2012). [15]
Drug-assistant M. tuberculosis threatens the national TB control programs in several countries. The spectrum and prevalence of drug resistance in this study are comparable to those in other countries in Sub-Saharan Africa, with resistance to isoniazid and streptomycin being more common than resistance to rifampicin and ethambutol. [14] However, considering that the overall rates of resistance among isolates from previously untreated patients in seven out of eight countries surveyed in Sub-Saharan Africa ranged from 3.4% to 13.4%, the corresponding resistance rate of 8.43% in this study is comparatively high and high resistance was observed to streptomycin (32%) and rifampicin (22.8%) rather than isoniazid (18.1%) and ethambutol (22.2%).
In studies by Karstaedt et al. in 1998, [16] a previous history of TB treatment was clearly associated with the development of drug resistance. In this study, the higher drug resistance was observed among relapse TB patients (22.4%), treatment failure (2.1%), and patients with interrupted drug use (6.3%).
In Sudan, these highly sophisticated techniques are unavailable and difficult to use in routine work; hence, encouraging and availing facilities for culture and sensitivity at least at some centers will help in curbing the spread of drug resistance.
Acknowledgment
The authors wish to acknowledge the scientists and workers at the tuberculosis laboratory of the National Health Laboratory in Khartoum for their technical assistance and support.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
| References | | |
| 1. | World Health Organization. Global Tuberculosis Report 2014. Mumbai, Maharashtra, Inida: World Health Organization; 2014.  |
| 2. | Kivihya-Ndugga L, van Cleeff M, Juma E, Kimwomi J, Githui W, Oskam L, et al. Comparison of PCR with the routine procedure for diagnosis of tuberculosis in a population with high prevalences of tuberculosis and human immunodeficiency virus. J Clin Microbiol 2004;42:1012-5. |
| 3. | World Health Organization. Global Tuberculosis Control: WHO Report 2010. Geneva: World Health Organization; 2010. |
| 4. | IUAT Technical Guide. Sputum Examination for Tuberculosis by Direct Microscopy in Low Income Countries; 2000. |
| 5. | Vincent V, Rigouts L, Nduwamahoro E, Holmes B, Cunningham J, Guillerm M, et al. The TDR Tuberculosis Strain Bank: A resource for basic science, tool development and diagnostic services. Int J Tuberc Lung Dis 2012;16:24-31. |
| 6. | Canetti G, Fox W, Khomenko A, Mahler HT, Menon NK, Mitchison DA, et al. Advances in techniques of testing mycobacterial drug sensitivity, and the use of sensitivity tests in tuberculosis control programmes. Bull World Health Organ 1969;41:21-43. [ PUBMED] |
| 7. | Sethi S, Sharma S, Sharma SK, Meharwal SK, Jindal SK, Sharma M. Drug susceptibility of Mycobacterium tuberculosis to primary antitubercular drugs by nitrate reductase assay. Indian J Med Res 2004;120:468-71. |
| 8. | Kubica GP, Gross WM, Hawkins JE, Sommers HM, Vestal AL, Wayne LG. Laboratory services for mycobacterial diseases. Am Rev Respir Dis 1975;112:773-87. [ PUBMED] |
| 9. | Zhang X, Andersen AB, Lillebaek T, Kamper-Jørgensen Z, Thomsen VØ, Ladefoged K, et al. Effect of sex, age, and race on the clinical presentation of tuberculosis: A 15-year population-based study. Am J Trop Med Hyg 2011;85:285-90. |
| 10. | Gupta D, Das K, Balamughesh T, Aggarwal AN, Jindal SK. Role of socioeconomic factors in tuberculosis prevalence. Indian J Tuberc 2004;51:27-31. |
| 11. | Abel L, Casanova JL. Genetic predisposition to clinical tuberculosis: Bridging the gap between simple and complex inheritance. Am J Hum Genet 2000;67:274-7. [ PUBMED] |
| 12. | World Health Organization Tuberculosis Control: The DOTS Strategy (Directly Observed Treatment Short-Course): An annotated Bibliography. Geneva: World Health Organization; 1997. |
| 13. | Negi SS, Khan SF, Gupta S, Pasha ST, Khare S, Lal S. Comparison of the conventional diagnostic modalities, bactec culture and polymerase chain reaction test for diagnosis of tuberculosis. Indian J Med Microbiol 2005;23:29-33. [ PUBMED]  |
| 14. | Pablos-Méndez A, Raviglione MC, Laszlo A, Binkin N, Rieder HL, Bustreo F, et al. Global surveillance for antituberculosis-drug resistance, 1994-1997. World Health Organization-International Union against Tuberculosis and Lung Disease Working Group on Anti-Tuberculosis Drug Resistance Surveillance. N Engl J Med 1998;338:1641-9. |
| 15. | Hassan SO, Musa MT, Elsheikh HM, Eleragi AM, Saeed NS. Drug resistance in Mycobacterium tuberculosis isolates from Northeastern Sudan. Br J Med Med Res 2012;2:424-43. |
| 16. | Karstaedt AS, Jones N, Khoosal M, Crewe-Brown HH. The bacteriology of pulmonary tuberculosis in a population with high human immunodeficiency virus seroprevalence. Int J Tuberc Lung Dis 1998;2:312-6. |
[Figure 1], [Figure 2], [Figure 3]
[Table 1], [Table 2], [Table 3], [Table 4], [Table 5]
|









 Search Pubmed for
Search Pubmed for