|
 
 |
| ORIGINAL ARTICLE |
|
| Year : 2016 | Volume
: 11
| Issue : 4 | Page : 109-112 |
|
Cataract prevalence, etiology, and systemic association in children attending EI walidain Charity Eye Hospital from April to July 2015
Atif A. M Saad1, Hind M. M Abusnina2, Karimeldin M. A Salih3
1 Department of Pediatrics, Faculty of Medicine, Omdurman Islamic University, Omdurman, Sudan
2 Pediatrician, Federal Ministry of Health, Khartoum, Sudan
3 Pediatrician and Medical Educator, Department of Pediatrics, College of Medicine, University of Bahri, Bahri, Sudan
| Date of Web Publication | 16-Mar-2017 |
Correspondence Address:
Atif A. M Saad
Department of Pediatrics, Faculty of Medicine, Omdurman Islamic University, Omdurman
Sudan
  | Check |
DOI: 10.4103/1858-5000.202358 
Background: Childhood cataracts are responsible for 5%–20% of blindness in children worldwide and for an even higher percentage of childhood visual impairment in developing countries. This study is an attempt to evaluate the prevalence, etiology, and systemic association of cataract in Sudanese children attending El walidain Charity Eye Hospital. Materials and Methods: this is a cross-sectional, observational prospective study in the period between April and July 2015. Out of 783 children were enrolled in this study, 52 children aged ≤18 years presented with cataract to El walidain Charity Eye Hospital in Khartoum state in the period between April and July 2015. Diagnosis of cataract was made based on history and clinical examination using ophthalmoscope and slit lamp. Results: Prevalence was 6.6%. Nearly 63% of the patients were male, mostly were male, usually idiopathic and juvenile in nature, corneal opacity and photophobia in addition to lens opacity manifested were the usual presentation. Trauma, steroid therapy, congenital, Down syndrome, and other systemic diseases found to be a risk factor. Conclusion: The prevalence of cataract in children in El walidain Charity Eye Hospital was more than that of a hospital-based study done in Tanzania. The mean age of patients was 6.1 years. Corneal opacity and lens opacity were the most common symptoms and signs, respectively. Idiopathic cataract was the most common type and decreased vision was the most common complication. Keywords: Cataract, congenital, diabetes, toxoplasmosis
How to cite this article:
Saad AA, Abusnina HM, Salih KM. Cataract prevalence, etiology, and systemic association in children attending EI walidain Charity Eye Hospital from April to July 2015. Sudan Med Monit 2016;11:109-12 |
How to cite this URL:
Saad AA, Abusnina HM, Salih KM. Cataract prevalence, etiology, and systemic association in children attending EI walidain Charity Eye Hospital from April to July 2015. Sudan Med Monit [serial online] 2016 [cited 2017 Mar 24];11:109-12. Available from: http://www.sudanmedicalmonitor.org/text.asp?2016/11/4/109/202358 |
| Introduction | |  |
Childhood cataracts are responsible for 5% to 20% of blindness in children worldwide and for an even higher percentage of childhood visual impairment in developing countries,[1] with the prevalence of childhood cataracts ranges from 1 to 15/10,000 children depending on the age groups, methods of ascertainment, and case definitions.[2] In a hospital-based study done in Muhimbili National Health (MNH) Pediatrics Eye Clinic in Tanzania, the overall prevalence of cataract was found to be 4.8% among 58 patients out of 1213 patients.[3] Cataracts are usually classified according to their location in the lens, morphologic appearance, and underlying pathology or according to age group. Children cataract may be unilateral or bilateral, isolated defects, accompanied by other ocular disorders or systemic disease. Leukocoria, poor fixation, and strabismus or nystagmus or both may be the presenting complaints. In the newborn, the absence of a red reflex should suggest the possibility of cataract, especially if the infant's pupil has been dilated for the examination.[4] Metabolic diseases, particularly certain disorders of carbohydrate, amino acid, calcium, and copper metabolism, congenital causes, trauma and inheritance, and trisomy; corticosteroids in addition play a role in etiology.[5] The earlier cataracts are diagnosed and treated, the more likely it is that sight will be preserved or develop normally because cataract blocks light from entering the eye and stimulating the retina, the area of the brain used for sight does not develop properly and lazy eye (amblyopia) occurs.[2] Adequate history, proper examination, laboratory investigation as well as ophthalmological examination will allow the correct diagnosis.[6],[7],[8],[9],[10],[11],[12]
The rational
Loss of vision in children has an impact on their education, employment, and social life, so early detection and management is of high priority.
Objectives
To determine the prevalence, causes, types, presentations, and social impact of cataract among children.
| Materials and Methods | | |
This is prospective, descriptive hospital-based study conducted in the period from April to July 2015 enrolling all children attending the hospital during this period. El walidain Charity Eye Hospital which is one of the main eye hospitals in Khartoum state. It consists of emergency unit, retina clinic, glaucoma clinic, general clinics, major and minor theaters, and four wards with a capacity of 24 beds. The hospital receives patients from various regions of Khartoum state and from different states of Sudan. The diagnosis is based on history and clinical examination using ophthalmoscope and slit lamp. The ophthalmoscope types used in this study were Welch Allyn ophthalmoscope and Keeler ophthalmoscope.
Inclusion criteria
All children with cataract in the period of the study were included in the study.
Exclusion criteria
Children with incomplete data and children or their caregiver who refuse to be involved or unfit for the study were excluded from the study. Data were organized into a master sheet using the Statistical Package for Social Sciences (SPSS) software version 20 (IBM Corp. in Armonk, NY). The research gained ethical approval from the Ethical Committee in Sudan Medical Specialization Board and Research Committee in the hospital and consent from caregivers.
| Results | | |
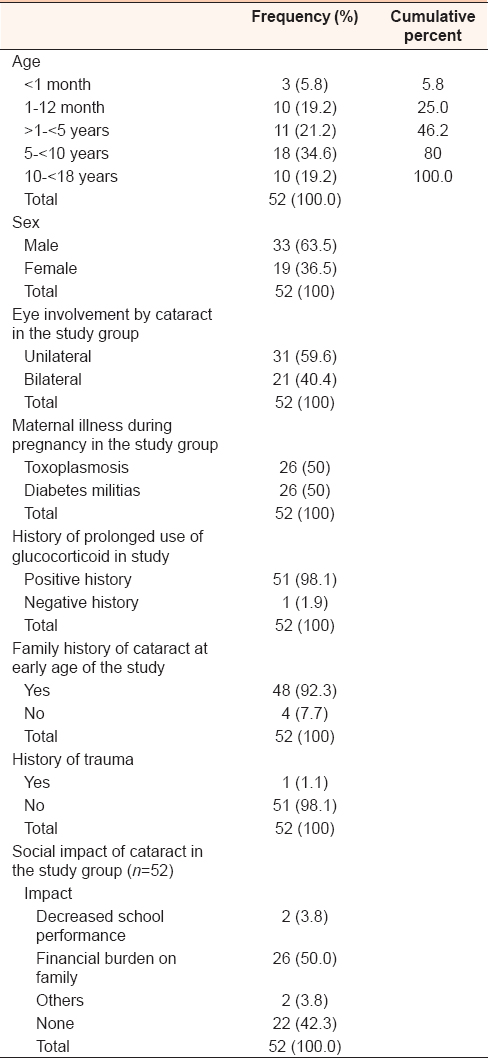
Out of 783 children attending the hospital, 52 children had cataract with the prevalence of 6.6%. The mean age at presentation was 6.1 years, third of them ranges between 5 and 10 years, 33 (63%) patients were male, 31 (59.6%) patients developed unilateral cataract, and maternal illness during pregnancy equally distributed between toxoplasmosis and diabetes mellitus 50% for each. Most of the patients had a history of prolonged use of glucocorticoid and family history of cataract at early age of the study (>98% and 92%), respectively. Financial burden on family and decreased school performance encountered in 50% and 3.8%, respectively [Table 1]. Hepatosplenomegaly and Dysmorphism encountered in 3.8% and 1.9%, respectively [Table 2] and [Table 3].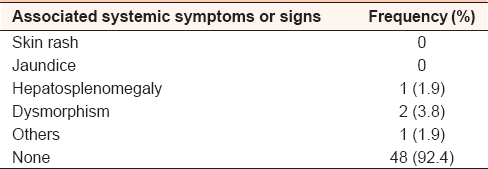 | Table 2: The frequency of associated systemic symptoms or signs in the study group (n=52)
Click here to view |
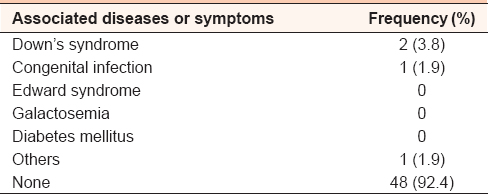 | Table 3: The frequency of associated systemic disease or symptoms in the study group (n=52)
Click here to view |
| Discussion | | |
The current study showed prevalence of cataract among Sudanese children at one of the major eye hospitals was 6.6%, mean age at presentation was 6.1 years, more commonly among male, most cases unilateral in nature, most mothers developed toxoplasmosis, diabetes during the pregnancy, glucocorticoid therapy, and family history were predisposing factors and financial burden on the family.
To the best of our knowledge, this is the first study among children in Sudan. The prevalence (6.6%) is not far from a study done in MNH Pediatrics Eye Clinic in Tanzania (4.8%)[3] and within the international range of prevalence (1–15/10,000 children). The wide range of prevalence could be explained in populations, age groups, methods of ascertainment, and case definitions.[2] The finding here of the unilateral cataract being the comments pattern, male dominance familial tendency for cataract. The mean age at presentation was 6.1 years in agreement with other studies.[2],[11],[13] Regarding symptoms, signs, and association of cataract finding in this work similar to presenting symptoms of childhood cataract reported by Holmes et al. as they mentioned that an infant with mild cataracts appears asymptomatic, delaying the diagnosis for years. At other times, lack of reaction to light, strabismus, a failure to notice toys, and faces or an apparent delay in development become the cause of concern. Mild cataracts may cause photophobia only in bright lights. Dense cataracts also may be discovered if they lead to the development of sensory nystagmus.[10] Only two patients (3.8%) were reported to have a history of maternal illness during pregnancy one mother had toxoplasmosis and the other had diabetes mellitus and as intrauterine infection is one of the causes of cataract in children mothers with intrauterine infections including rubella, herpes simplex, toxoplasmosis, varicella, and syphilis their children warrant careful ophthalmic evaluation.[14]
Only one patient was reported to have cataract associated with the prolonged use of glucocorticoid which was prescribed for management of nephrotic syndrome, and this is similar to what was written by Taylor and his colleague 2010; the cataractogenic effects of systemic glucocorticoids are well documented, so ophthalmologic evaluation for children receiving long-term systemic glucocorticoids or adrenocorticotropic hormone is recommended, and the risk of cataracts with inhaled glucocorticoids is not well established.[3]
In four patients (7.6%), cataract was associated with family history at an early age. In two of them, it affected their brother, in one patient it affected sister, and in the last one, his brother and father, in contrast to what was mentioned in literature heredity that cataract represents one-third of all congenital and developmental cataracts due to genetically determined chromosomal anomaly.[2],[15],[16],[17]
Only four patients (7.6%) had associated systemic symptoms and signs of them had hepatosplenomegaly and diagnosed as congenital infection (toxoplasmosis), two patients had dysmorphic features of Down's syndrome, and in comparison with literature chromosomal abnormalities (Trisomies) can be associated with cataract, and in Down syndrome which is the most common one. Small lens opacities are very common (50%), but the incidence of visually significant cataract requiring surgery is probably <5%.[18]
One patient had signs of rickets and justified by that hypocalcemia is one of the metabolic causes of cataract.[19]
Investigations to identify the cause were not needed in twenty patients (38.5%), in whom the cause of cataract was trauma. In one patient, TORCH screening was done, and the result was toxoplasmosis infection. Moreover, one patient with rickets underwent investigation for serum calcium and phosphate. In thirty patients (57.7%), the investigations were not done; two of them had dysmorphic features of Down's syndrome, and in 28 patients (53.8%), there was no apparently associated systemic symptoms or signs, so no further investigations required, and this group of patients (53.8%) represents the idiopathic type of cataract and our percentage was a little bit higher than the reported percentage of idiopathic cataract 40% to 50% of cases and these are generally sporadic.[20]
Associated complications were reported in 22 patients (42.3%), the most common one was decreased vision in 54.7%, followed by amblyopia in 31.8%, loss of vision in 9%, and secondary glaucoma in 4.5%. Regarding the social impact of cataract, the most common one is a financial burden on family in 26 patients (50%), whereas decreased school performance was reported in 2 patients (3.8%) and psychological trauma reported in 2 patients (3.8%).
| Conclusion | | |
The prevalence of cataract in children in El walidain Charity Eye Hospital is 6.6%, the mean age of patients was 6.1 years; corneal opacity and lens opacity were the most common symptoms and signs, respectively. Idiopathic cataract was the most common type and decreased vision was the most common complication. Addressing the important issues and drawing the attention of all stallholders (parents, health providers, teacher, and community at large) to detect and manage this problem early were the strength of the study. Only addressing those who came to the hospital and only one hospital was the weakness of the study.
Recommendation
The community-based multicenter study is needed, and facilities for early detection should be provided.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
| References | | |
| 1. | Foster A, Gilbert C. Epidemiology of childhood blindness. Eye (Lond) 1992;6(Pt 2):173-6.  |
| 2. | Foster A, Gilbert C, Rahi J. Epidemiology of cataract in childhood: A global perspective. J Cataract Refract Surg 1997;23 Suppl 1:601-4. |
| 3. | Mosenene NS. Pattern and Magnitude of Congenital and Developmental Cataract among Children Attending Muhimbili National Hospital Paediatric Eye Clinic. Child Health: Tanzania; Muhimbili University of Health and Allied Sciences; 2010. |
| 4. | Behrman RE, Kliegman RM, Jenson HB. Nelson Textbook of Pediatrics. 16 th ed. Philadelphia: W.B. Saunders Company; 2000. p. 1917-8. |
| 5. | Myron Y, Jay DS. Yanoff Ophthalmology. 1 st ed. London: Geoff Greenwood; 1999. p. 764-80. |
| 6. | Tesser RA, Hess DB, Buckley EG. Pediatric cataracts and lens anomalies. In: Nelson LB, Olitsky SE, editors. Harley's Pediatric Ophthalmology. 5 th ed. Philadelphia: Lippincott Williams & Wilkins; 2005. p. 255-9. |
| 7. | Calhoun JH. Cataracts in children. Pediatr Clin North Am 1983;30:1061-9. |
| 8. | Lambert SR, Taylor D, Kriss A, Holzel H, Heard S. Ocular manifestations of the congenital varicella syndrome. Arch Ophthalmol 1989;107:52-6. |
| 9. | Wolff SM. The ocular manifestations of congenital rubella. Trans Am Ophthalmol Soc 1972;70:577-614. |
| 10. | Holmes JM, Leske DA, Burke JP, Hodge DO. Birth prevalence of visually significant infantile cataract in a defined U.S. population. Ophthalmic Epidemiol 2003;10:67-74. |
| 11. | Olitsky SE, Nelson LB. Common ophthalmologic concerns in infants and children. Pediatr Clin North Am 1998;45:993-1012. |
| 12. | Wright KW, Kohn T, Matsumoto E. Lens abnormalities. In: Wright KW, editors. Pediatric Ophthalmology. St. Louis: Mosby; 1995. p. 367. |
| 13. | Wilson ME, Trivedi RH, Pandey SK. Miscellaneous issues and views. In: Wilson ME, Trivedi RH, Pandey SK, editors. Pediatric Cataract Surgery. Philadelphia: Lippincott Williams & Wilkins; 2005. p. 293. |
| 14. | Taylor JB, Young WO, Rutar T. Posterior subcapsular cataracts in children receiving adrenocorticotropic hormone (ACTH) for infantile spasms. J Child Neurol 2010;25:1017-9. |
| 15. | Berger BB. The lens cataract and its management. In: Peyman GA, editor. Principle and Practice of Ophthalmology. Philadelphia, PA, WB Saunders, 1980;506-7. |
| 16. | Gittinger JW. Congenital cataracts. In: Gittinger JW, Asdourian GK, editors. Manual of Clinical Problems in Ophthalmology. 1 st ed. Boston: Little Brown and Co.; 1998. p. 75-6. |
| 17. | Singh D. Congenital and infantile cataracts. In: Fraun Felden FT, Roy FR, editors. Current Ocular Therapy. 5 th ed. Philadelphia: W.B. Saunders Company; 2000. p. 538-41. |
| 18. | Berk AT, Saatci AO, Erçal MD, Tunç M, Ergin M. Ocular findings in 55 patients with Down's syndrome. Ophthalmic Genet 1996;17:15-9. |
| 19. | Roy FR. Ocular Syndromes and Systemic Diseases. Philadelphia, PA, WB Saunders; 1980:506-7. |
| 20. | Khurana AK. Diseases of the lens. In: Ophthalmology. 2 nd ed. New Delhi: New Age International; 2000. p. 183-212. |
[Table 1], [Table 2], [Table 3]
|









 Search Pubmed for
Search Pubmed for