|
 
 |
| ORIGINAL ARTICLE |
|
| Year : 2014 | Volume
: 9
| Issue : 3 | Page : 112-115 |
|
Partner disclosure and human immunodeficiency virus serology status among antenatal clinic attendees with human immunodeficiency virus infection in Ilorin
AS Adeniran1, ST Raji2, R Saidu1, LO Omokanye1
1 Department of Obstetrics and Gynaecology, University of Ilorin, PMB 1515; Department of Obstetrics and Gynaecology, University of Ilorin Teaching Hospital, PMB 1459, Ilorin, Nigeria
2 Department of Obstetrics and Gynaecology, University of Ilorin Teaching Hospital, PMB 1459, Ilorin, Nigeria
| Date of Web Publication | 15-Nov-2014 |
Correspondence Address:
A S Adeniran
Department of Obstetrics and Gynaecology, University of Ilorin, PMB 1515, Ilorin
Nigeria
 Source of Support: None, Conflict of Interest: None  | Check |
DOI: 10.4103/9783-1230.144772

Background: The high prevalence of human immunodeficiency virus (HIV) remains rampant in sub-Saharan Africa with poor partner disclosure and a high risk for infections among serodiscordant couples. Objective: To determine the prevalence, partner disclosure and HIV serology pattern among HIV positive antenatal clinic attendees. Design: A descriptive (retrospective) study. Setting: The antenatal clinic of a tertiary center in Ilorin, Nigeria. Subjects: HIV positive women receiving antenatal care at the study site from September 1, 2010 to February 28, 2013. Materials and Methods: The case files and the antenatal clinic records of all participants were retrieved, relevant data were extracted and presented in tables and charts. Results: Of the 7,342 antenatal clinic attendees during the study period, 237 were HIV-positive (prevalence 4.9%). The modal age group was 30-34 years (42.6%), adolescents were three (1.3%), 206 (86.9%) were educated, 192 (81%) were employed, 96 (40.5%) were diagnosed during index pregnancy while 141 (59.5%) were diagnosed and commenced antiretroviral therapy prior to conception. The modal age for male partners was 35-44 years (54%), 228 (96.2%) were aware of the woman's HIV status, 211 (89%) of these men were aware of their own HIV status while the 26 (11%) refused testing; the serodiscordance rate was 56.7%. Conclusion: The high serodiscordance rate for HIV infection portends a significant risk for transmission between partners; thus, higher awareness during and outside pregnancy should be improved upon to educate on strategies for preventing partner and mother to child transmissions. Keywords: Antenatal clinic attendees, human immunodeficiency virus infection, human immunodeficiency virus serology, partner disclosure
How to cite this article:
Adeniran A S, Raji S T, Saidu R, Omokanye L O. Partner disclosure and human immunodeficiency virus serology status among antenatal clinic attendees with human immunodeficiency virus infection in Ilorin. J Med Investig Pract 2014;9:112-5 |
How to cite this URL:
Adeniran A S, Raji S T, Saidu R, Omokanye L O. Partner disclosure and human immunodeficiency virus serology status among antenatal clinic attendees with human immunodeficiency virus infection in Ilorin. J Med Investig Pract [serial online] 2014 [cited 2018 Aug 24];9:112-5. Available from: http://www.jomip.org/text.asp?2014/9/3/112/144772 |
| Introduction | |  |
Since the first reported case of acquired immunodeficiency syndrome (AIDS) in 1981, the number of people living with human immunodeficiency virus (PLWHIV) continues to increase and AIDS-related illnesses are still one of the leading causes of death worldwide. [1] The burden is highest in sub-Saharan Africa where 63% of PLWHIV reside. [2] Central to the control of human immunodeficiency virus (HIV) is a diagnosis of infection, treatment of currently infected individuals and prevention of new infections. Reports indicated that up to one-third of individuals diagnosed with HIV infection continue to have unprotected sex without informing their sexual partners who may be of positive, negative or unknown sero-status. [3] Partner disclosure may motivate partner testing, encourage changes in sexual and social behavior and ultimately decrease HIV transmission. It also affords the individual the opportunity for social support, improved access to care including antiretroviral treatment and prevention of mother-to-child transmission (PMTCT) interventions, increases opportunities to discuss and implement HIV risk reduction with partners and opportunities to plan for the future. [4],[5] Thus, disclosure of HIV status has been emphasized by the WHO and Centre for Disease Control and Prevention as an important prevention goal. [6],[7] Potential disadvantages of partner disclosure include unpredictable partner response with possibilities of blame and accusations of infidelity, loss of economic support, abandonment, abuse (physical/emotional) and disruption of family relationships. [4],[7] WHO estimated that about 50% of HIV-positive individuals are in serodiscordant relationships with significant new infections. [8] Where the HIV status of both partners is known, measures can be taken to prevent infection in the seronegative partner and treat the affected one. Parental HIV serodiscordance hampers the care of the HIV seropositive child with more frequent discharge against medical advice, abandonment, poor follow-up, lack of paternal responsibility during care and poor immunization. [9]
With the PMTCT programme, women are often the first member of a stable relationship to know their HIV status and can serve as a point of contact for couples' HIV counseling and test (CHCT). This may increase the uptake of HIV testing within the community and reduce the HIV transmission rate.
This study was carried out to determine the partner disclosure and serodiscordance rates in women attending the antenatal clinic of a tertiary center in Ilorin and to determine the associated bio-social variables.
| Materials and methods | | |
This was a retrospective descriptive study of all HIV positive women who attended the antenatal clinic at a tertiary center in Ilorin, Nigeria from September 1, 2010 to February 28, 2013. Records of all eligible patients were accessed from the case files and PMTCT clinic records. The PMTCT unit is run together with the general antenatal clinic every week days. Activities conducted there include pre-test counseling, testing and post-test counseling for women attending the antenatal clinic, couple's HIV counseling and testing, adherence counseling for HIV positive pregnant women, distribution of prescribed drugs and postnatal support for both the woman and the child. The data collected included socio-demographic characteristics of the women and their partners, time of diagnosis of HIV in the women, use of highly active antiretroviral therapy (HAART), partner disclosure, partner serology status and the serodiscordance. During the study patient confidentiality was ensured by use of codes instead of patient names, records were kept away from non-members of the research team and no means of individual identification of participants were included in the study.
The data retrieved was analyzed and depicted using percentages, proportions, tables and charts. There was no conflict of interest in the conduct of the study.
| Results | | |
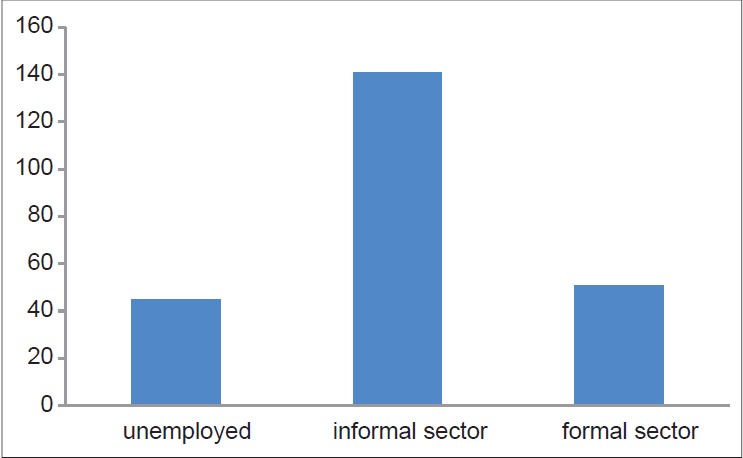
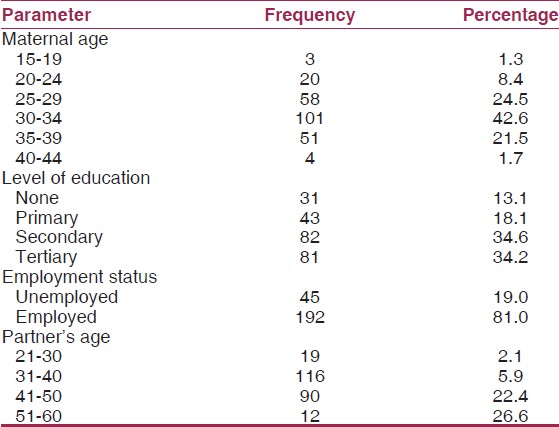
During the study period (September 1, 2010 to February 28, 2013), 7342 clients booked for antenatal care, of these, 365 were HIV positive, giving a prevalence of 4.9%. Records of 237 of these patients were available giving a retrieval rate of 64.9%; these 237 were included in subsequent analysis. From [Table 1], participants were aged 17-42 years, with a mean age of 30-34 years (42.6%), 13.1% had no formal education, and 19.0% were unemployed. The male partners were older than their wives with ages ranging from 21 to 60 years with modal age 31-40 years while 19% of the women were unemployed [Figure 1]. In [Table 2], 96 (40.5%) women were diagnosed during pregnancy, 141 (59.5%) were diagnosed and had commenced HAART before index pregnancy with duration ranging from 1 month to 8 years; 228 (96.2%) men were aware of their female partner's status among whom 203 (89%) had undergone HIV testing; 115 (48.5%) men were HIV seronegative, 88 (37.1%) were seropositive and 34 (14.4%) were of unknown status. Thus, the serodiscordance rate was 48.5% and seroconcordance 37.1%. Ten of the 88 (11.4%) HIV positive partners were newly diagnosed during CHCT at the clinic. In [Table 3], nine (3.8%) women refused to disclose their serology status to the male partner; of these, 5 (55.6%) were diagnosed in index pregnancy and 4 (44.4%) before pregnancy while six of them had tertiary education.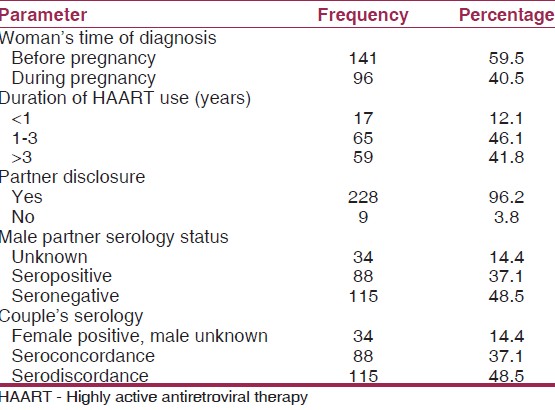 | Table 2: Timing of the women's testing, antiretroviral use, partner disclosure and serology
Click here to view |
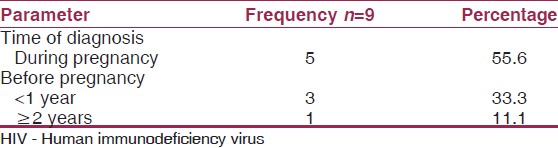 | Table 3: Time of diagnosis of HIV in women who refused partner disclosure
Click here to view |
| Discussion | | |
The prevalence of HIV among pregnant women in this study was 4.97% similar to reports from Benin City (5.2%) [10] and Abakaliki (5.4%); [11] lower than Jos (8.2%) [12] and Anambra (8.6%) [13] but higher than Niger Delta (3.96-4.1%). [14],[15] This shows a wide variation of HIV prevalence between different regions in Nigeria; this may be a reflection of the differences in sexual practices and behavior, awareness of HIV infection and testing, sociocultural practices and accessibility to healthcare. Literate women had a higher prevalence of HIV infection compared to their non-literate counterpart similar to report from Benin city. [10] This may be because literate women have a higher awareness about HIV and a generally better health seeking behavior necessitating presentation for screening; however, they are more likely to have a liberal attitude to sexual activities. The 96% partner disclosure rate was higher than the 16.7-86% quoted by the WHO for developing countries. [4] Other studies reported disclosure rates of 89% [5] (Jos), 46.2% [1] (Abidjan), 76.6% [7] (Ethiopia) and 61.5% [16] (Uganda). This may be the outcome of repeated counseling on the importance of partner disclosure and its effect on drug adherence and other PMTCT interventions. More than half of the women had initiated HAART for more than a year; reports from Ethiopia, Tanzania and Mozambique showed that most women their HIV status after 12 month of initiation of HAART. [7],[17] All of the nine women who did not disclose their HIV status to their partners were literate (66.7% had tertiary education); this compares with the report from Ethiopia that literate women were 60% less likely to disclose their seropositive status to their sexual partner than the non-literates. [7] Partner disclosure by HIV-positive women makes the male partners about three times more likely to undertake HIV testing than the partners of HIV-positive women who did not disclose their status. [1] This may explain the 89% testing rate and 11.4% newly diagnosed cases in this study. There is wide variation in serodiscordance rates with 56.7% in this study, 78.8% in Benin City, [10] 48.4% in Jos, [5] 7.7% in Kano [18] all in Nigeria and 40.2% in Abidjan [1] and 38.7% in Uganda. [16] This may be a reflection of the cultural, social and available support in each community.
This study concludes that since antenatal clinics may be a woman's first point of contact with the health care system, HIV counseling and testing should be integrated in such clinics at all levels of health care with repeated counseling and support for partner disclosure and testing. The high serodiscordance rate for HIV infection portends a significant risk for transmission between partners; thus, higher awareness during and outside pregnancy should be improved upon to educate on strategies for preventing partner and mother to child transmissions. The retrospective nature of this study limited the opportunity to determine the exact time of disclosure and the partner's response afterwards.
| References | | |
| 1. | Brou H, Djohan G, Becquet R, Allou G, Ekouevi DK, Viho I, et al. When do HIV-infected women disclose their HIV status to their male partner and why? A study in a PMTCT programme, Abidjan. PLoS Med 2007;4:e342.  |
| 2. | Joint United Nations Programme on HIV/AIDS (UNAIDS), World Health Organization (WHO). AIDS Epidemic Update: Special Report on HIV/AIDS: December 2006. Geneva: UNAIDS/WHO; 2006. Available from: http://www.data.unaids.org/pub/EpiReport/2006/2006_EpiUpdate_en.pdf. [Last accessed on 2013 Apr 01]. |
| 3. | Dan C, Ron S, Rebecca C, James C. Disclosure of HIV Status to Sexual Partners Among a Random Sample of American Seropositives. AIDS Research Institute University of California San Francisco. Available from: http://www.caps.ucsf.edu/uploads/pubs/presentations/pdf/ciccarone.pdf. [Last accessed on 2013 Apr 31]. |
| 4. | WHO. HIV Status Disclosure to Sexual Partners: Rates, Barriers and Outcomes for Women. WHO Documentary. Geneva: WHO Press; 2004. |
| 5. | Sagay AS, Musa J, Ekwempu CC, Imade GE, Babalola A, Daniyan G, et al. Partner disclosure of HIV status among HIV positive mothers in Northern Nigeria. Afr J Med Med Sci 2006;35 Suppl: 119-23. |
| 6. | UNAIDS. Best practices collection, counseling and HIV/AIDS. Geneva; 2007. Available from: http://www.hivaidsclearinghouse.unesco.org/search/resources/PNADB282.pdf. [Last accessed on 2013 Apr 01]. |
| 7. | Erku TA, Megabiaw B, Wubshet M. Predictors of HIV status disclosure to sexual partners among people living with HIV/AIDS in Ethiopia. Pan Afr Med J 2012;13:87. |
| 8. | WHO HIV/AIDS Programme. Guidance on couples HIV testing and counseling - including antiretroviral therapy for treatment and prevention in serodiscordant couples. Recommendations for a Public Health Approach. Geneva: WHO Press; 2012. |
| 9. | Adejuyigbe EA, Odebiyi AI. Parental HIV serodiscordance: Implications for the care of the HIV seropositive child in a resource-poor setting. AIDS Care 2006;18:537-43. |
| 10. | Imade P, Ibadin K, Eghafona N, Enabulele O, Ophori E. HIV seroprevalence among pregnant women attending antenatal clinic in a tertiary health institution in Benin City, Nigeria. Macedonian J Med Sci 2010;3:43-5. |
| 11. | Obi SN. Pregnancy outcome in HIV seroprevalence in Abakaliki, Nigeria. Orient J Med 2005;17:25-30. |
| 12. | Sagay AS, Kapiga SH, Imade GE, Sankale JL, Idoko J, Kanki P. HIV infection among pregnant women in Nigeria. Int J Gynaecol Obstet 2005;90:61-7. |
| 13. | Ezegbudo CN, Agbonlahor DE, Nwobu GO, Igwe CU, Agba MI, Okpala HO, et al. The seroprevalence of hepatitis B surface antigen and human immunodeficiency virus among pregnant women in Anambra State, Nigeria. Shiraz E Med J 2004;5:1-9. |
| 14. | Egesie UG, Mbooh RT. Seroprevalence of human immunodeficiency virus (HIV) infection in pregnant women in Amassoma, Nigeria. Afr J Biomed Res 2008;11:111-3. |
| 15. | Buseri F, Seiyaboh E, Jeremiah Z. Surveying infections among pregnant women in the Niger Delta, Nigeria. J Glob Infect Dis 2010;2:203-11. |
| 16. | Osinde MO, Kaye DK, Kakaire O. Sexual behaviour and HIV sero-discordance among HIV patients receiving HAART in rural Uganda. J Obstet Gynaecol 2011;31:436-40. |
| 17. | Pearson CR, Cassels S, Kurth AE, Montoya P, Micek MA, Gloyd SS. Change in sexual activity 12 months after ART initiation among HIV-positive Mozambicans. AIDS Behav 2011;15:778-87. |
| 18. | Sagay AS, Onakewhor J, Galadanci H, Emuveyan EE. HIV status of partners of HIV positive pregnant women in different regions of Nigeria: Matters arising. Afr J Med Med Sci 2006;35 Suppl: 125-9. |
[Figure 1]
[Table 1], [Table 2], [Table 3]
|









 Search Pubmed for
Search Pubmed for