|


 |
| CASE REPORT |
|
| Year : 2012 | Volume
: 4
| Issue : 2 | Page : 118-120 |
|
|
An Unusual Presentation of Vallecular Cyst with near Fatal Respiratory Distress and Management Using Conventional Laparoscopic Instruments
Sandesh V Parelkar1, Jiwan L Patel1, Beejal V Sanghvi1, Prashant B Joshi1, Subrat K Sahoo1, Nandita Sampat1, Sanjay N Oak1, Nilam Sathe2
1 Department of Pediatric Surgery, KEM Hospital, Mumbai, Maharashtra, India
2 Oto-Rhino-Laryngology, Seth G S Medical College and KEM Hospital, Mumbai, Maharashtra, India
| Date of Web Publication | 8-Apr-2013 |
Correspondence Address:
Prashant B Joshi
Department of Pediatric Surgery, King Edward Memorial Hospital, Parel, Mumbai
India
 Source of Support: None, Conflict of Interest: None
DOI: 10.4103/2006-8808.110257

 Abstract Abstract | | |
Vallecular cyst is a rare cause of upper airway obstruction in infants and children and presentation like acute stridor with near fatal respiratory distress is extremely rare. It is one of the rare causes of difficult intubation, during which cyst aspiration can improve the access. Vallecular cyst is commonly managed using microlaryngoscope and specialized instruments. We hereby report a method of endoscopic management of these cysts using conventional laparoscopic instruments. Keywords: Endoscopic management, respiratory distress, vallecular cyst
How to cite this article:
Parelkar SV, Patel JL, Sanghvi BV, Joshi PB, Sahoo SK, Sampat N, Oak SN, Sathe N. An Unusual Presentation of Vallecular Cyst with near Fatal Respiratory Distress and Management Using Conventional Laparoscopic Instruments. J Surg Tech Case Report 2012;4:118-20 |
How to cite this URL:
Parelkar SV, Patel JL, Sanghvi BV, Joshi PB, Sahoo SK, Sampat N, Oak SN, Sathe N. An Unusual Presentation of Vallecular Cyst with near Fatal Respiratory Distress and Management Using Conventional Laparoscopic Instruments. J Surg Tech Case Report [serial online] 2012 [cited 2016 Jun 10];4:118-20. Available from: http://www.jstcr.org/text.asp?2012/4/2/118/110257 |
| Introduction | |  |
Congenital cysts of the larynx are a rare cause of upper airway obstruction in infants and children. Vallecular cysts are benign retention cysts of the minor salivary glands. The commonest site is the lingual surface of epiglottis. They distort the epiglottis when they increase in size and eventually fill the vallecula. Blockage of the laryngeal inlet causing severe respiratory distress is an unusual presentation. A surgical method of management of such cases using conventional laparoscopic instruments has been reported here.
| Case Report | | |
A 2-month female child presented to a peripheral hospital with difficulty in breathing and weak cry since 15 days. Later, she had an episode of breath holding when she became apneic and cyanotic after vigorously crying. Stridor with desaturation was subsequently noted, which only improved when the baby was lying in the lateral position and given oxygen supplementation. The child had history of oral and nasal regurgitation of feeds also. Computerized tomography (CT) scan confirmed the diagnosis as left vallecular cyst [Figure 1]a and b and the child was referred to a higher center for further management.
On admission to our hospital, the baby had severe respiratory distress and did not respond to facemask bagging so endotracheal intubation was needed. Patient was started on intravenous antibiotics and steroids. Direct laryngoscopy revealed a swelling in the region of the left vallecula, obscuring the view of the larynx and laryngopharynx. Endoscopic excision of the cyst was performed successfully using conventional 3 mm laparoscopic instruments.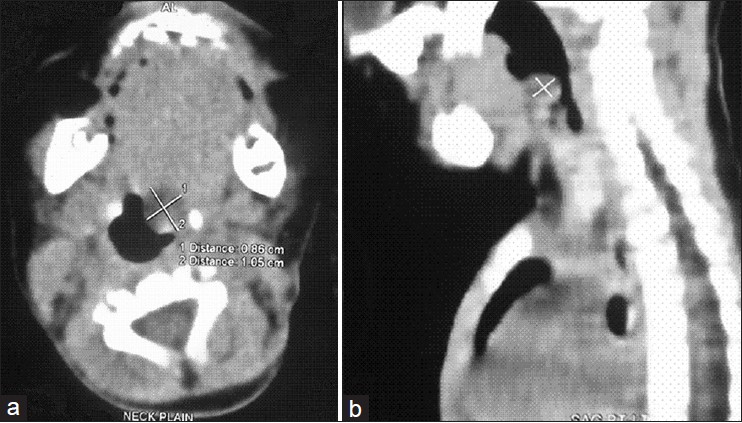 | Figure 1: (a) Computerized tomography scan image (Transverse cut) showing left vallecular cyst. (b) CT scan image (Lateral view) showing left vallecular cyst
Click here to view |
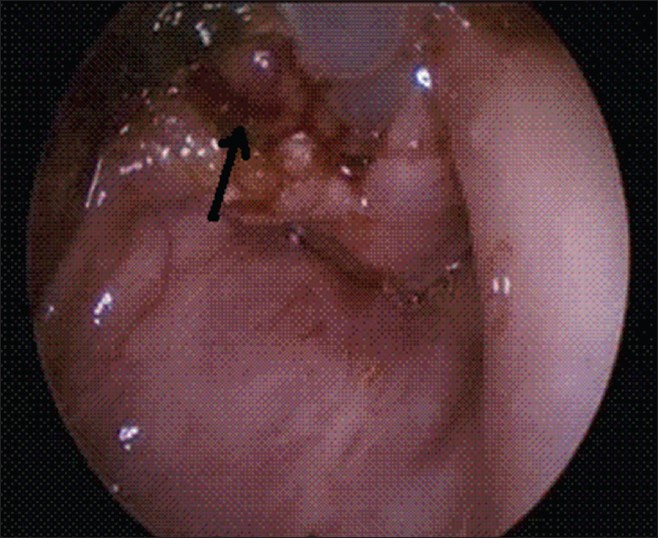
| Procedure | | |
Patient was placed at supine with extended neck position in operation table. Since previously intubated endotracheal tube was partially blocked, change of the endotracheal tube was attempted. At this time, the lesion was obscuring the laryngeal inlet and reintubation becomes difficult, which becomes possible only after aspiration of the cyst. Direct laryngoscopy showed the cystic lesion arising from the left vallecula [Figure 2]. A 4-mm zero-degree telescope was placed in pharynx transorally to visualize the cyst. Cauterization of the cyst wall was done circumferentially using hook electrocautery. Cyst wall was grasped using conventional Maryland forceps and deroofing done. Mucosal lining of the remaining posterior wall was excised totally [Figure 3]; 3 mm insulated laparoscopic instruments were used for the whole procedure. Complete hemostasis was achieved and extubation was possible on table. Postoperatively, the patient had stridor and tachypnea for the initial 2 days, which improved with intravenous steroid and nebulization. Feeding was started on the third day and the patient was discharged on the fifth day after surgery. On follow-up 6 months and 1 year after the surgery, the baby is doing well with no respiratory symptoms.
| Discussion | | |
Vallecular cysts are retention cysts which originate as a result of ductal obstruction of either mucous glands or minor salivary glands in the vallecula and base of the tongue. These cysts are fairly uncommon and exact incidence is not known. [1] Infants are affected most often but they have also been reported in older children and adults. [2] Small cysts are asymptomatic, but when enlarged may present with stridor, feeding difficulties, voice change and respiratory distress. [1],[3],[4] Acute airway obstruction leading to even fatal or near fatal outcome has also been reported. [5]
Vallecular cysts commonly arise from the lingual surface of the epiglottis and histologically contain respiratory epithelium with mucous glands with an external lining of squamous epithelium. [3]
Antenatal detection with ultrasound scanning and magnetic resonance imaging helps in parental counseling and perinatal preparation. [6] Post-natally, direct laryngoscopy remains the best diagnostic tool, which also helps in detection of laryngomalacia, commonly associated with vallecular cyst. [7]
In post-natal cases, ultrasound can be used as a screening method for congenital stridor especially for those who have no experience in flexible laryngoscopy. It provides good distinction between solid and cystic masses and confirms the presence of a normal thyroid gland (to rule out a lingual thyroid). [8]
The optimal study for the diagnosis of vallecular cyst post-natally is Gadolinium-enhanced magnetic resonance imaging (MRI). The cyst appears hypointense on T1-weighted and hyperintense on T2-weighted images and there is no enhancement after contrast. These features distinguish it from other entities. However, the usefulness of MRI is limited by the need for sedation and should consider the influence of breathing and swallowing, which cannot be prevented by sedation. High speed scanning should be used if the findings are not logically consistent. [8]
With the help of ultrathin flexible endoscopes, laryngoscopy can be carried out even in premature newborns. The flexible endoscope is technically and ergonomically easier to use. It does not interfere with the anesthetist's ventilation by the mask or endotracheal tube. If no muscle relaxation is used, the muscular activity of the larynx can be observed during spontaneous and assisted ventilation. However, it cannot make fine distinctions between the various differential diagnosis of vallecular cyst. Hence, it has to be replaced by direct laryngoscopy, performed by a skilled operator under cardiopulmonary monitoring, to enable methodical examination in such cases. Thus, flexible laryngoscopy is recommended for initial screening and direct laryngoscopy can be used for definitive diagnosis. [8],[9]
Surgical treatment for vallecular cysts in infants includes aspiration, marsupialization (deroofing) and excision. The surgical approach is transoral under direct vision with or without a microlaryngoscope or using a microlaryngoscope with a camera assembly. [8]
The various tools used for this purpose include direct electrocautery, CO 2 laser or microlarygngoscopic instruments.
The use of the carbon dioxide laser for surgery of the vocal fold is a subject of controversy. Many prefer to avoid it, for although the cutting beam is reasonably precise, it is hypothesized that the tissue reaction is somewhat unpredictable, probably because of the emitted heat. The alternative is microscopic instruments. Although they are more technically difficult to use, they offer equivalent accuracy and perhaps less potential for inadvertent damage and scarring.
Suzuki et al. [8] reported a negligible recurrence rate after marsupialization of vallecular cysts as compared to complete excision. Complete excision is more invasive and there is the possibility of bleeding and postoperative residual scarring. Hence, marsupialization is the preferred treatment of vallecular cysts.
The same study recommends that aspiration should be attempted only as an initial maneuver in cases of difficult intubation and not as definitive treatment due to high rates of recurrence.
Da Vinci robot-assisted excision of a vallecular cyst was reported recently by McLeod et al. and further research is needed to explore this modality of treatment. [10]
Excision of cyst using a tonsillar snare has also been reported as an easy and cost-effective method of treatment. [11]
Conventional laparoscopic instruments used were a 4 mm 0-degree telescope; 3 mm hook electrocautery and Maryland forceps. These give very good vision during surgery. The use of long instruments (approximately 33 cm) permits easy accessibility and maneuverability to the deep oral cavity and avoids undue overlapping and fighting between instruments. The instruments are insulated along their length which prevents thermal injury to other structures in the oral cavity. Pediatric surgeons are used to operating with conventional laparoscopic instruments as against specialized instruments like microdebrider, microscissors, etc.
| Conclusion | | |
Vallecular cyst is a rare and an unusual cause of stridor and severe respiratory distress in infants and children. Laryngomalacia is a common association and a close differential diagnosis. Direct laryngoscopy is diagnostic. Excision can be performed easily with a set of conventional laparoscopic instruments. The technique adopted by us is a quick, safe and cost-effective way of management of vallecular cyst.
| References | | |
| 1. | Ahrens B, Lammert I, Schmitt M, Wahn U, Paul K, Niggemann B. Life threatening vallecular cyst in a 3-month-old infant: Case report and literature review. Clin Pediatr (Phila) 2004;43:287-90. 
|
| 2. | Cheng SS, Forte V, Shah VS. Symptomatic Congenital Vallecular Cyst in a Neonate. J Pediatr 2009;155:446.
|
| 3. | Gutierrez JP, Berkowitz RG, Robertson CF. Vallecular cysts in newborns and young infants. Pediatr Pulmonol 1999;17:282-5.
|
| 4. | Oluwole M. Congenital vallecular cyst, a cause of failure to thrive. Br J Clin Pract 1996;50:170.
|
| 5. | Albert DM, Ali Z. Two cases of vallecular cyst presenting with acute stridor. J Laryngol Otol 1985;99:421-5.
|
| 6. | Cuillier F, Samperiz S, Testud R, Fossati P. Antenatal diagnosis and management of a vallecular cyst. Ultrasound Obstet Gynecol 2002;20:623-6.
|
| 7. | Ku AS. Vallecular cyst: Report of four cases-one with co-existing laryngomalacia. J Laryngol Otol 2000;114:224-6.
|
| 8. | Suzuki J, Hashimoto S, Watanabe K, Takahashi K. Congenital vallecular cyst in an infant: Case report and review of 52 recent cases. J Laryngol Otol 2011;125:1199-203.
|
| 9. | aWengen DF, Probst RR, Frei FJ. Flexible laryngoscopy in neonates and infants: Insertion through a median opening in the face mask. Int J Pediatr Otorhinolaryngol 1991;21:183-7.
|
| 10. | McLeod IK, Melder PC. Da Vinci robot-assisted excision of a vallecular cyst: A case report. Ear Nose Throat J 2005;84:170-2.
|
| 11. | Bhandary S. Innovative Surgical Technique in the Management of Vallecular Cyst. Online J Health Allied Sci. 2003;3:2.
|
[Figure 1], [Figure 2], [Figure 3]
|