|
 
 |
| ORIGINAL ARTICLE |
|
| Year : 2016 | Volume
: 4
| Issue : 2 | Page : 90-95 |
|
Sexual dimorphism in hand grip strength and hand dimensions among Hausas
Kabiru B Umar1, Barnabas Danborno1, Kolawale V Olorunshola2, Lawan H Adamu3
1 Department of Human Anatomy, Faculty of Medicine, Ahmadu Bello University, Zaria, Nigeria
2 Department of Human Physiology, College of Health Sciences, University of Abuja, Abuja, Nigeria
3 Department of Anatomy, Faculty of Basic Medical Sciences, College of Health Sciences, Bayero University, Kano, Nigeria
| Date of Web Publication | 18-Apr-2017 |
Correspondence Address:
Kabiru B Umar
Department of Human Anatomy, Faculty of Medicine, Ahmadu Bello University, Zaria
Nigeria
 Source of Support: None, Conflict of Interest: None  | Check |
DOI: 10.4103/2315-7992.204687

Background: Handgrip strength (HGS) is an anthropometric variable that is affected by a number of factors including age, gender, and body size. Aim: This study was designed to determine the gender differences in HGS and hand dimensions of secondary schools students in Kano metropolis. Materials and Methods: A cross-sectional study carried out on Hausas of Kano Metropolitan. Seven hundred and ten (340 males and 370 females) participated in the study. The hand dimensions were measured using digital vernier caliper. The HGS of right and left hands were measured using a standard adjustable digital hand grip dynamometer at sitting position. Descriptive statistics (mean ± standard deviation) was used to express the data. Independent sample t-test was used to find differences. Statistical significance was declared at P< 0.05. Data were analyzed using SPSS (IMB, Corporation, NY, USA) version 20. Results: A significant difference was observed among 17–18 and 19–20 age groups in the right-handed female participants with no such differences in the left-handed female participants. For 17–18 aged groups, the significant difference exists between the sexes in HGS and hand dimensions. In 19–20 age groups, similar pattern of significant difference was noticed in HGS and hand dimensions. Conclusion: It was concluded that function of HGS is the function of good hand dimension and body variable and vice versa. Age provided to be a factor that may influence the grip strength and hand dimension among Hausas.
Keywords: Hand dimensions, hand grip strength, hausa ethnic group, sexual dimorphism
How to cite this article:
Umar KB, Danborno B, Olorunshola KV, Adamu LH. Sexual dimorphism in hand grip strength and hand dimensions among Hausas. Ann Bioanthropol 2016;4:90-5 |
| Introduction | |  |
The power of hand grip is the result of forceful flexion of all finger joints with the maximum voluntary force that the subject can exert under normal biokinetic conditions.[1] Handgrip strength (HGS) is an anthropometric variable that is affected by a number of factors including age, gender, and body size.[2] The human hand is unique in being free of habitual locomotor duty and devoted entirely to functions of manipulation.[3]
Many of the research studies correlated grip strength to various other physical variables including nutritional status, rotator cuff weakness, fatigue, overall physical function anthropometric traits; weight, height, hand length. [2,4-7] Some studies found a correlation between grip strength and hand performance. Although in theory, one would believe the two are correlated but more studies may be necessary from other populations. The information related to the correlations of hand-anthropometry and grip strength in Hausas community is scanty. The information on correlations between HGS and hand dimensions among Kano metropolis indigence is nonexistent. For many games such as volleyball and basketball in which the use of the hand is essential, hand morphology, and grip strength may be of functional significance for effective performance. Therefore, reference data on various forms of hand dimension and HGS may be of paramount importance in solving problems associated with hand games and injuries.
The estimation of HGS is of immense importance in determining the efficacy of different treatment strategies of hand and also in hand rehabilitation. The reliability and valid evaluation of HGS is also of paramount importance in determining the effectiveness of various surgical and treatment procedure. The grip strength is also of use as a functional index of nutritional status of an individual. The data on hand dimension can be used for the designing of suitable hand tools, orthotics, gloves, etc., for the Hausas. The assessment of HGS may be used in the investigation and follow-up of patients with neuromuscular disease. Many exercises in gyms and fitness centers across the country indirectly work on individuals grip. Other exercises such as deadlifts, bent over rows among others also depend on the athlete's level of grip strength. The aim of the study is to investigate the sexual dimension in HGS and selected hand dimension among Hausas of Kano metropolis.
| Materials and Methods | | |
Study location
The study was conducted in Kano metropolis of Nigeria, which is located between latitude 12.2° North and longitude 9.4° East with the Kano city as the capital of the state [Figure 1]. Hausa is the lingua franca, but English is the official language. Kano is a city in Nigeria and the capital of Kano is Kano metropolis in Northwestern Nigeria. Its metropolitan population is the second largest in Nigeria after Lagos. The Kano Urban area covers 137 km 2 and comprises six local government area (LGAs) - Kano Municipal, Fagge, Dala, Gwale, Tarauni, and Nassarawa - with a population of 2163,225 at the 2006 Nigerian census. The Metropolitan area covers 499 km 2 and comprises eight LGAs-the six mentioned above plus Ungogo and Kumbotso - with a population of 2828,861 at the 2006 Nigerian census (NPC/FGN 2006). The principal inhabitants of the city are Hausa people. As in most parts of Northern Nigeria, the Hausa Language is widely spoken in Kano.
Subjects
Sampling was done randomly. The stratified sampling technique was used to collect data from twelve selected secondary school in Kano metropolis. The sample size for this study was 710 subjects comprising both male (340) and female (370) students from secondary schools of the metropolis. Criteria for inclusion were no restriction of movement in the upper limbs and no history of the inflammatory joint disease, neurological disorder, or injury to the upper or lower extremity by self-report. All the subjects were apparently healthy and within the age range of 15–20 were included in the study. The exclusion criteria were any subject with congenital deformities diseases or injuries in the hands and body parts. Any participant outside the age range was excluded from the study and also anybody who did not sign the consent form. Ethical approval was obtained from the committee on ethics from Kano State Hospital Management Board. Introduction letter was used to seek for permission at selected secondary schools in Kano metropolis.
Anthropometry
Hand dimension was measured using digital vernier caliper. Hand length was measured as the perpendicular distance from the tip of the middle finger to the wrist crease baseline. For the length of the 3rd digit (D3), a perpendicular distance from the tip of the D3 to ventral proximal crease this was used to determine the plamar length. The palmar length was calculated as hand length minus the D3 length (that is the distance from the midpoint of the distal wrist crease to the midpoint of the proximal digit crease). Palmar width was also considered as the distance between the radial side of metacarpal D2 (index finger) and ulnar side of metacarpal D5 [Figure 2].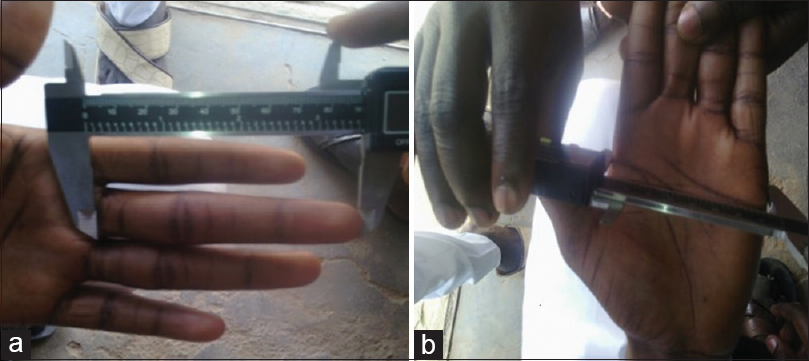 | Figure 2: Procedure for measuring hand dimensions ([a] third digit length [b] palmar breath)
Click here to view |
The right and left grip strength were measured using a digital hand grip dynamometer (Model EH101, Camry, China) at sitting position with shoulder adducted and neutrally rotated and elbow in semi-flex position [Figure 3]. The subjects were asked to put maximum force on the dynamometer. The value was recorded to the nearest 0.1 kg.
Statistical analyses
The data were expressed as mean ± standard deviation. Sexual dimorphism in HGS and digit length were determined using independent sample t-test. The analysis was done using SPSS version 20 (IBM Corporation, NY, USA). Statistical significance was declared at P< 0.05.
| Results | | |
A statistically significant (P < 0.005) sexual dimorphism in hand length, palmer length, and palmer width was observed. Higher mean value (P < 0.05) was recorded among male participants in both right- and left-hand variable among three age groups, 15–16 [Table 1], 17–18 [Table 2] and 19–20 [Table 3].
Figure 4] and [Figure 5] show a statistically significant sex differences were also observed with respect to HGS in both right [Figure 4] and left [Figure 5]. In all the three age groups, male participants tend to have higher mean value (P < 0.001) compared to the female counterparts.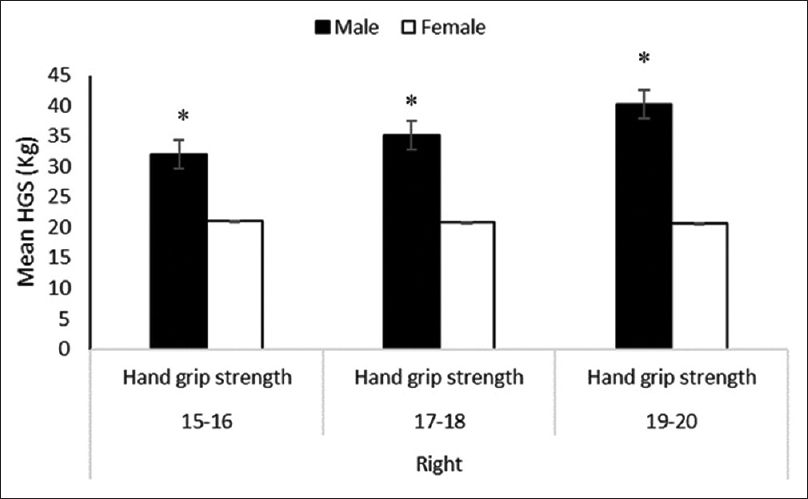 | Figure 4: Sexual dimorphism in the right-hand grip strength across different age categories *P < 0.001
Click here to view |
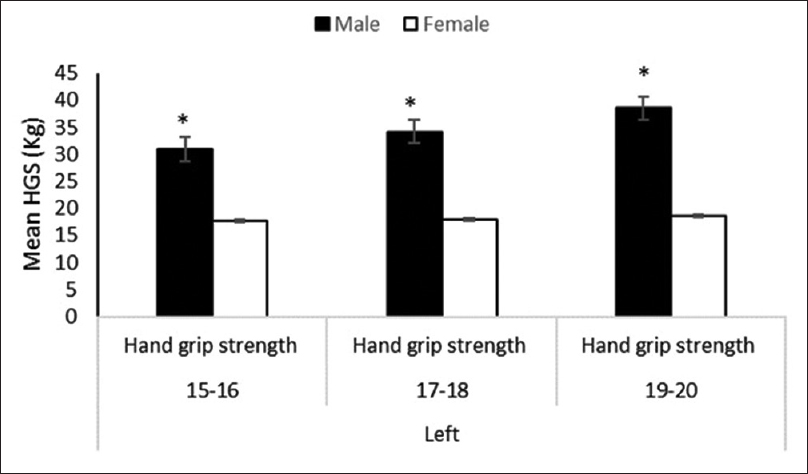 | Figure 5: Sexual dimorphism in the left-hand grip strength across different age categories *P < 0.001
Click here to view |
| Discussion | | |
HGS may be negatively affected by local disorders of the hand as well as by radiculopathy caused by degenerative changes in the cervical spine. Assessment of hand function, use of objective and reliable instruments and knowledge about the reference values of HGS and hand morphology is lacking in our locality. Numerous authors have studied handgrip strength in healthy individuals, and several of them have reported age- and - sex-specific data.[8],[9] The data on HGS and dimension can also be used for the designing of suitable hand tools, orthotics, and gloves among different ethnic groups including Hausas. The current study investigated the role of dominant hand in determining higher HGS, the sexual dimorphism and relationship between handgrip strength and some selected hand dimensions among Hausas of Kano metropolis.
With regards to hand dominance, the present study shows that a statistically significant difference was present among 17–18 and 19–20 age groups in right-handed female participants with no such differences in the left-handed female participants. However, in the previous researches, it was documented that the HGS is higher in dominant hand with right-handed subjects, but no such significant differences between sides could be documented for left-handed people.[10],[11],[12] also notice that stronger grip and pinch strengths were obtained at dominant sides of the participants and only 14.09% of the subjects had stronger nondominant hand grips.
The variation observed in the current finding with respect to higher grip strength in the left-handed participants among this study population may be linked to genetic influences due to differences in the ethnicity between the different study groups. Moreover, in the current results the differences in the grip strength with the dominance of hand was only observed among the female participant. This also gives another insight into the influence of genetic factor in the expression of higher grip strength with respect to the dominant hand. Although the sample size between the right- and left-handed participants is not proportional and this may affect conclusive statement to some extent. However, despite this limitation of the sample size which was also seen in the study by [13] that analyzed 48 left-handed and 262 right-handed subjects and found a significant difference between the two groups. Therefore, the issue of sample small sample size of left-handed participants is unavoidable in most population, including ours. This may be linked to cultural and/or religious influences that necessitate the use of the right hand as dominant against the left hand; hence, a left-hand dominant individual will be transformed into the right-handed individual. Furthermore, significant differences in the right- and left-hand width, right- and left-hand length, left grip strength values between female basketball, volleyball, and handball players was also noticed. Handball group was the reason for the significance.[14]
The reason of this sexual dimorphism in the study variables may be linked to several factors, for instance, senescence accounts for a larger percentage of the variation in HGS in men, with male HGS declining more quickly after the age of 30.[15] Sex differences also observed in forebrain and cardiac sympathetic nervous responses at the onset of handgrip exercise,[16] with smaller cardiovascular response (heart rate and mean arterial pressure) and weaker insular cortex activation, observed in women. Interestingly, this may reflect both physiological and psychological sex differences when asked to provide a maximum squeeze of a dynamometer. While greater height, weight, and muscle mass in males have been submitted as an explanation for this effect [17],[18] the sexual dimorphism in androgenic hormones (i.e., testosterone) may be the responsible factor. For instance, men with reduced testosterone levels caused by androgen deprivation have been shown to have low grip strength and supplementary increases in testosterone enhance HGS as well as lean body mass in elderly men with low serum testosterone.[19],[20],[21] Moreover, somatic sex differences in mammals to date have been found to be due to either androgenic masculinization or effects of the sex chromosomes [22] and increased bone mineral density and muscle mass in males when compared to females as another influencing factor.[23],[24] In addition to the previous reason reported in the literature, the current research also consider the exposure of male to the more manual work than the female counterpart to be an additional environmental factor lead to sexual differences between male and female in HGS and other study variables. Moreover, the more manual work exposure, the higher the musculature, hence the higher the grip strength.
Age is one of the confounding variables in most of the anthropological studies such categorization of individuals according to different age groups is always important for making some generalized conclusion. In the current study, we determine the sexual dimorphism in the study variables by three age categories, 15–16, 17–18 and 19–20 years of age. The present result shows that among 15–16 years of age, there are gender differences in the HGS and hand dimensions with the exception of left palmar length.
According to previous report, the hand grip power of females shows an age-level difference between the young and the elderly in all loads (30%, 40%, and 50%). However, the required time to reach peak velocity was longer in the elderly at 50%, and the time is shorter at 30% than at 40% and 50% in both young and elderly groups.[25] Therefore, a baseline data are always needed almost for every population groups. To achieve that for our local community, the present study categorized the data obtained a base on ages and sexes. Therefore, the mean value obtained for a particular age group of sex categories will be compared with any other population of the same sex and age categories. For instance, the mean grip strength of the different age categories of our study population indicates a linear increase of HGS with respect to age. Although in the previous studies involving volunteers aged 25–64 years indicated a decrease in handgrip strength in relation to the ages.[25],[26],[27] The possible explanation for the contradictory findings could be due to the influences of the age of HGS. According to [28] handgrip strength decreases by only about 0.5% a year from the age of 30 until 45–49 years of age, after which the decline accelerates to about1% a year until the age of 75, followed by an even larger decrease. Therefore, the reverse trend of increase in the HGS may occur in the individual below the 30 years of age.
Another possible explanation for the increase and decrease in handgrip strength in individual below and above the 30 years of age respectively may be due to the onset of muscle atrophy associated with individual above age of 30 years and normal body growth rate as well as an increase in the muscle tone before the age of 30 years. This explanation is in accordance with previous findings, who reported less loss of strength infrequently used muscles [28],[29] that is to say, i.e., older people in today's society have previously done heavier manual work than younger individuals. In general, it has been well documented that in adulthood, skeletal muscle strength in general decreases with age.[30] Based on the above discussion, the age and sex-specific data for HGS were provided for our locality. Hence, the mean value of the grip strength in the above-mentioned age categories may always be utilized within our Hausas population as a reference value.
| Conclusion | | |
Based on the current findings, there are strong sexual differences between the HGS and hand dimension. This indicated that function of HGS is the function of good hand dimension and body variable and vice versa. Age provided to be a factor that may influence the grip strength and hand dimension among Hausas.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
| References | | |
| 1. | Blair VA. Hand function. In: Durward BR, Baer GD, Rowe PJ, editors. Functional Human Movement. Oxford: Butterworth-Heinemann; 2002. p. 160-79.  |
| 2. | Kenjle K, Limaye S, Ghugre PS, Udipi SA. Grip strength as an index for assessment of nutritional status of children aged 6-10 years. J Nutr Sci Vitaminol (Tokyo) 2005;51:87-92. |
| 3. | Marzke MW. Origin of the human hand. Am J Phys Anthropol 1971;34:61-84. |
| 4. | Benefice E, Malina R. Body size, body composition and motor performances of mild-to-moderately undernourished Senegalese children. Ann Hum Biol 1996;23:307-21. |
| 5. | Guo CB, Zhang W, Ma DQ, Zhang KH, Huang JQ. Hand grip strength: An indicator of nutritional state and the mix of postoperative complications in patients with oral and maxillofacial cancers. Br J Oral Maxillofac Surg 1996;34:325-7. |
| 6. | Häger-Ross C, Rö sblad B. Norms for grip strength in children aged 4-16 years. Acta Paediatr 2002;91:617-25. |
| 7. | Budoff JE. The prevalence of rotator cuff weakness in patients with injured hands. J Hand Surg Am 2004;29:1154-9. |
| 8. | Mathiowetz V, Kashman N, Volland G, Weber K, Dowe M, Rogers S. Grip and pinch strength: Normative data for adults. Arch Phys Med Rehabil 1985;66:69-74. |
| 9. | Härkö nen R, Piirtomaa M, Alaranta H. Grip strength and hand position of the dynamometer in 204 Finnish adults. J Hand Surg Br 1993;18:129-32. |
| 10. | Chong CK, Tseng CH, Wong MK, Tai TY. Grip and pinch strength in Chinese adults and their relationship with anthropometric factors. J Formos Med Assoc 1994;93:616-21. |
| 11. | Armstrong CA, Oldham JA. A comparison of dominant and non-dominant hand strengths. J Hand Surg Br 1999;24:421-5. |
| 12. | Incel NA, Ceceli E, Durukan PB, Erdem HR, Yorgancioglu ZR. Grip strength: Effect of hand dominance. Singapore Med J 2002;43:234-7. |
| 13. | Incel NA, Ceceli E, Durukan PB, Erdem HR, Yorgancioglu ZR. Grip strength: Effect of hand dominance. Singapore Med J 2002;43:234-7. |
| 14. | Petersen P, Petrick M, Connor H, Conklin D. Grip strength and hand dominance: Challenging the 10% rule. Am J Occup Ther 1989;43:444-7. |
| 15. | Cagatay B, Pinar D, Sibel K. Evaluation of hand anthropometric measurements and grip strength in basketball, volleyball and handball players. Int J Exp Clin Anat 2008;2:55-9. |
| 16. | Vianna LC, Oliveira RB, Araújo CG. Age-related decline in handgrip strength differs according to gender. J Strength Cond Res 2007;21:1310-4. |
| 17. | Wang TD, Goto S, Bhatt DL, Steg PG, Chan JC, Richard AJ, et al. Ethnic differences in the relationships of anthropometric measures to metabolic risk factors in Asian patients at risk of atherothrombosis: Results from the REduction of Atherothrombosis for Continued Health (REACH) registry. Metabolism 2010;59:400-8. |
| 18. | Kamarul T, Ahmad TS, Loh WY. Hand grip strength in the adult Malaysian population. J Orthop Surg (Hong Kong) 2006;14:172-7. |
| 19. | Kuh D, Hardy R, Butterworth S, Okell L, Wadsworth M, Cooper C, et al. Developmental origins of midlife grip strength: Findings from a birth cohort study. J Gerontol A Biol Sci Med Sci 2006;61:702-6. |
| 20. | Page ST, Amory JK, Bowman FD, Anawalt BD, Matsumoto AM, Bremner WJ, et al. Exogenous testosterone (T) alone or with finasteride increases physical performance, grip strength, and lean body mass in older men with low serum T. J Clin Endocrinol Metab 2005;90:1502-10. |
| 21. | Sih R, Morley JE, Kaiser FE, Perry HM 3 rd, Patrick P, Ross C. Testosterone replacement in older hypogonadal men: A 12-month randomized controlled trial. J Clin Endocrinol Metab 1997;82:1661-7. |
| 22. | Wang C, Swerdloff RS, Iranmanesh A, Dobs A, Snyder PJ, Cunningham G, et al. Transdermal testosterone gel improves sexual function, mood, muscle strength, and body composition parameters in hypogonadal men. J Clin Endocrinol Metab 2000;85:2839-53. |
| 23. | Fink B, Thanzami V, Seydel H, Manning JT. Digit ratio and hand-grip strength in German and Mizos men: Cross-cultural evidence for an organizing effect of prenatal testosterone on strength. Am J Hum Biol 2006;18:776-82. |
| 24. | Hemberal M, Doreswamy V, Rajkumar S. Study of correlation between hand circumference and maximum grip strength (MGS). Natl J Physiol Pharm Pharmacol 2014;4:195-7. |
| 25. | Aoki H, Demura S. Age differences in hand grip power in the elderly. Arch Gerontol Geriatr 2011;52:e176-9. |
| 26. | Peolsson A, Hedlund R, Oberg B. Intra- and inter-tester reliability and reference values for hand strength. J Rehabil Med 2001;33:36-41. |
| 27. | Bohannon RW, Peolsson A, Massy-Westropp N, Desrosiers J, Bear-Lehman J. Reference values for adult grip strength measured with a Jamar dynamometer: A descriptive meta-analysis. Physiotherapy 2006;92:11-5. |
| 28. | Malkia E. Strength and aging: Patterns of change and implications for training. In: Harms-Ringdahl K, editor. Muscle Strength: International Perspectives in Physical Therapy. 8 th ed. Edinburgh: Churchill-Livingstone; 1993. p. 141-67. |
| 29. | Hackel ME, Wolfe GA, Bang SM, Canfield JS. Changes in hand function in the aging adult as determined by the Jebsen test of hand function. Phys Ther 1992;72:373-7. |
| 30. | Bassey EJ, Harries UJ. Normal values for handgrip strength in 920 men and women aged over 65 years, and longitudinal changes over 4 years in 620 survivors. Clin Sci (Lond) 1993;84:331-7. |
[Figure 1], [Figure 2], [Figure 3], [Figure 4], [Figure 5]
[Table 1], [Table 2], [Table 3]
|









 Search Pubmed for
Search Pubmed for