|
 
 |
| CASE REPORT |
|
| Year : 2015 | Volume
: 3
| Issue : 1 | Page : 23-25 |
|
Implant-retained nasal prosthesis
Ozlem Kara1, Necla Demir2, A Nilgun Ozturk2, Mustafa Keskin3
1 Department of Prosthodontics, Faculty of Dentistry, Bezm-i Alem University, Istanbul, Turkey
2 Department of Prosthodontics, Faculty of Dentistry, Selcuk University, Konya, Turkey
3 Department of Plastic and Reconstructive Surgery, Faculty of Medicine, Selcuk University, Konya, Turkey
| Date of Web Publication | 5-Jan-2015 |
Correspondence Address:
Ass. Prof. Ozlem Kara
Department of Prosthodontics, Faculty of Dentistry, Bezm-i Alem University, Istanbul
Turkey
 Source of Support: None, Conflict of Interest: None  | Check |
DOI: 10.4103/2347-4610.148518

Malignant tumors of the nose occasionally require rhinectomy. Facial defects can cause not only functional problems but also some serious physchological problems that could cause the individual to avoid social contact. In view of this, the first aim of maxillofacial rehabilitation should be solving esthetic problems. Implant retained prostheses can give good esthetic results. Predictable biomechanical retention of nasal prostheses can be achieved using osseointegrated implants and intra-oral and craniofacial implants have been used previously. These prostheses are tissue compatible, simple in design and easy to place, can be worn independently of spectacles and in the majority of cases can be provided soon after surgical excision. In this case report, a nasal prosthesis was fabricated for a patient who lost his nose due to the basal cell carcinoma. Extra-oral implants and magnet retention for the proper connection of the nasal prosthesis were used. This prosthesis was acceptable for the patient because of excellent support, retentive abilities and the patient's appearance. Keywords: Implant retained prosthesis, nasal prosthesis, osseointegrated nasal implants
How to cite this article:
Kara O, Demir N, Ozturk A N, Keskin M. Implant-retained nasal prosthesis. Eur J Prosthodont 2015;3:23-5 |
| Introduction | |  |
Management of neoplastic disease often involves surgical excision to achieve tumor-free margins in the residual tissue. [1] Tumors affecting the nose may necessitate a total or near-total rhinectomy, thereby creating a prominent midfacial defect. Surgical or prosthetic reconstruction is usually required; however, the prominent location and complexity of the anatomical configuration makes surgical reconstruction difficult. This situation is further complicated by the esthetic and functional demands in this site. [2] In view of this, the first aim of maxillofacial rehabilitation should be solving esthetic problems. [3],[4],[5]
The skin of the nose is a common site for basal cell and squamous cell carcinomas, which make up 12% of all skin tumors. [6] Nearly half of the patients with advanced cancer of the nose have squamous cell carcinomas,' which is more likely to recur than basal cell carcinoma. [6],[7],[8]
Partial thickness defects can be managed very satisfactorily by surgery. Full thickness defects can be reconstructed by surgery or a prosthesis. Reconstruction of large, full thickness defects of the nose following ablative oncological surgery remains a challenge, despite recent advances in surgical reconstruction techniques. [9]
With the advent of osseointegration in dental rehabilitation and recent advances in surgical or laboratory techniques, it has been possible to maintain the facial rehabilitation. [10]
Long-term success of a facial prosthesis mainly depends on retention. Retention of the facial prosthesis depends on providing a better edge integrity and conserving the position of the prosthesis during every movement of the head and mimic muscles. [11] Anatomic undercuts, skin adhesives and implants are important factors to provide sufficient retention. Extra-oral implant retained prosthesis have been proven to be a predictable treatment option for maxillofacial rehabilitation. [12],[13],[14],[15]
The preference for an implant-supported silicone prosthesis was also based on the premise that the implant surgery would be much simpler and less morbid for the patient, who also suffered from chronic cardiorespiratory disease. [16]
The use of implants with various bar designs, clips, magnets, and other retentive devices have aided in the stabilization and orientation of the prosthesis. [17],[18],[19],[20],[21]
In this case report, a patient who required a nasal prosthesis is presented.
| Case Report | | |
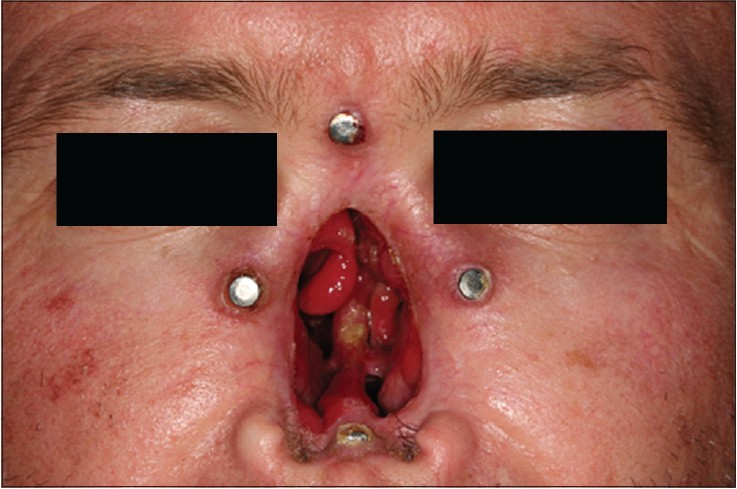
A 37-year-old man's nasal area had been resected due to basal cell carcinoma. Two EO implants (Straumann, AG, Switzerland)) were placed for each orbital bone, one implant was placed for glabella and one implant was placed for maxilla by plastic surgeon [Figure 1].
After the post-operative healing period, the concha area in the basement of the defect was covered, and an impression was taken from the defect together with the adjacent tissue, using a polyvinyl siloxane impression material (Virtual; Ivoclar Vivadent, Liechenstein) [Figure 2]. A nasal pattern was created using the ''donor technique,'' in which a person with ear contours that closely mimic those of the patient acts as the donor to make a nasal impression. A plaster cast was obtained from the defect area and a wax sculpture was formed, taking into account the patient's general appearance [Figure 3]. The prepared wax pattern was then adapted to the stone cast. The whole morphology of the cast was corrected based on visual knowledge, older photographs of the patient, and the patient's own descriptions of his preoperative appearance. After the completion of the wax pattern corrections, (ie, tissue texture and relevant contours), the same procedures were repeated on the face of the patient. The cast was then placed into a flask. After the complete removal of wax, the silicon material (Silasfic, medical adhesive silicone type A, Dow Coming), which was colored intrinsically (Intrinsic Coloring Kit, Factor II) was then bulk filled, and the material was processed according to the manufacturer's directions. After processing, the prosthesis was removed from the mold. The final corrections were made, and the silicon prosthesis was then adapted to the defect area [Figure 4]. By using eyeglasses, the esthetic appearance and retention of the prosthesis were enhanced.
| Discussion | | |
Advanced tumors of the midfacial region occasionally require extensive surgical removal of the tissue around the defect, to eradicate the disease. A large facial defect can prevent a patient from returning to normal daily activities. [22],[23]
Many patients with these defects have been rehabilitated successfully with prosthetic restorations. [24] Secondary mechanical factors, skin adhesives, and implants can provide retention for small midfacial defects. Anatomic undercuts are sufficient for maintaining retention of these maxillofacial prostheses. [5]
The use of craniofacial implants for retention of extraoral prosthesis, such as nasals, offers excellent support and retentive abilities and improves a patient's appearance and quality of life. [25],[26] However, a satisfactory outcome may only be achieved by careful planning in terms of the number and position and orientation of the implants and the proper connection of the nasal prosthesis to implant retention structure. [26]
Magnet and bar-and-clip retentions are the two primary forms of retention used in the auricular region.The bar-clip system provides good retention for the prostheses. However, bars may limit access for performing hygiene procedures and make it difficult to insert and remove the prosthesis. The most common problem encountered with the bar and clip system is loosening of the clip after 3-4 months. Magnetic retention can be selected because of hygiene, mechanical, and esthetic considerations. [21]
| References | | |
| 1. | Johnson JT. Management of advanced cancers of the external nose. Oncology (Williston Park) 1993;7:73-7.  |
| 2. | Brooks MD, Carr AB, Eckert SE. Nasal stent fabrication involved in nasal reconstruction: Clinical report of two patient treatments. J Prosthet Dent 2004;91:123-7. |
| 3. | Reisberg DJ, Habakuk SW. Nasal conformer to restore facial contour. J Prosthet Dent 1990;64:699-701. |
| 4. | Beumer J, Curtis TA, Marunick MT. Maxillofacial rehabilitation: Prosthodontic and Surgical Considerations. 2 nd ed. St Louis: Ishiyaku Euroamerica; 1996. p. 404. |
| 5. | Gurbuz A, Kalkan M, Ozturk AN, Eskitascioglu G. Nasal prosthesis rehabilitation: A case report. Quintessence Int 2004;35:655-6. |
| 6. | Goepfert H, Arredondo R, McNeese M. Cancers of the skin of the nose. Otolaryngol Head Neck Surg 1982;90:237-40. |
| 7. | Stanley RJ, Olsen KD. Rhinectomy for malignant disease: A 20 year experience. Arch Otolaryngol Head Neck Surg 1988;114:1307-11. |
| 8. | Harrison DF. Total rhinectomy: A worthwhile operation? J Laryngol Otol 1982;96:1113-23. [ PUBMED] |
| 9. | Ethunandan M, Downie I, Flood T. Implant-retained nasal prosthesis for reconstruction of large rhinectomy defects: The Salisbury experience. Int J Oral Maxillofac Surg 2010;39:343-9. |
| 10. | Seals RR Jr, Cortes AL, Parel SM. Fabrication of facial prosthesis by applying the osseointegration concept for retention. J Prosthet Dent 1989;61:712-6. |
| 11. | Godoy AJ, Lemon JC, Nakamura SH, King KG. A shade for acrylic facial prosthesis. J Prosthet Dent 1992;68;120-2. |
| 12. | Wolfaardt JF, Wilkes GH, Parel SM, Tjellstrom A. Craniofacial osseointegration: The Canadian experience. Int J Oral Maxillofac Implants 1993;8:197-204. |
| 13. | Tolman DE, Desjardins RP. Extraoral applications of osseointegrated implants. J Oral Maxillofac Surg 1991;49:33-45. |
| 14. | Parel SM, Tjellstrom A. The United States and Swedish experience with osseointegration and facial prostheses. Int J Oral Maxillofac Implants 1991;6:75-9. |
| 15. | Cheng AC, Morrison D, Cho RS, Archibald D. Vacuum-formed matrix as a guide for the fabrication of craniofacial implant tissue bar-retained auricular prostheses. J Prosthet Dent 1998;79:711-4. |
| 16. | Dimitroulis G. Nasal implants following nasectomy. Int J Oral Maxillofac Surg 2007;36:447-9. |
| 17. | Rubenstein JE. Attachments used for implant- supported facial prostheses: A survey of United States, Canadian, and Swedish centers. J Prosthet Dent 1995;73:262-6. |
| 18. | Lemon JC, Chambers MS. Locking retentive attachment for an implant-retained auricular prosthesis. J Prosthet Dent 2002;87:336-8. |
| 19. | Gary JJ, Donovan M. Retention designs for bone-anchored facial prostheses. J Prosthet Dent 1993;70:329-32. |
| 20. | Thomas KF. Freestanding magnetic retention for extraoral prosthesis with osseointegrated implants. J Prosthet Dent 1995;73:162-5. |
| 21. | Del Valle V, Faulkner G, Wolfaardt J, Rangert B, Tan HK. Mechanical evaluation of craniofacial osseointegration retention systems. Int J Oral Maxillofac Implants 1995;10:491-8. |
| 22. | Cheng AC, Morrison D, Wee AG, Maxymiw WG, Archibald D. 1998 Judson C. Hickey Scientific Writing Award. Maxillofacial prosthodontic management of a facial defect complicated by a necrotic frontal bone flap: A clinical report. J Prosthet Dent 1999;82:3-7. |
| 23. | Rcisberg DJ, Habakuk SW. Nasal confonner to restore facial contour. J Prosthet Dent 1990;64:699-701. |
| 24. | McCartney JW. Osseointegrated implant-supported and magnetically retained ear prosthesis: A clinical report. J Prosthet Dent 1991;66:6-9. |
| 25. | Chung RW, Siu AS, Chu FC, Chow TW. Magnet-retained auricular prosthesis with an implant-supported composite bar: A clinical report. J Prosthet Dent 2003;89:446-9. |
| 26. | Gilson TD, Asgar K, Peyton FA. The quality of union formed in casting gold to embedded attachment metals. J Prosthet Dent 1965;15:464-73. [ PUBMED] |
[Figure 1], [Figure 2], [Figure 3], [Figure 4]
|












 Search Pubmed for
Search Pubmed for