|
 
 |
|
CASE REPORT |
|
|
|
| Year : 2012 | Volume
: 18
| Issue : 1 | Page : 125-126 |
| |
Cockayne syndrome-xeroderma pigmentosum complex with demyelination: A rare association
Usha Rani Singh, Shujaath Asif, Peter Prasanth Kumar Kommu, Philomina D'Souza
Department of Pediatrics, Pondicherry Institute of Medical Sciences, Pondicherry, India
| Date of Web Publication | 26-May-2012 |
Correspondence Address:
Usha Rani Singh
Department of Pediatrics, Pondicherry Institute of Medical Sciences, Pondicherry
India
 Source of Support: None, Conflict of Interest: None
DOI: 10.4103/0971-6866.96681

 Abstract Abstract | | |
Xeroderma pigmentosum-Cockayne syndrome (XP-CS) includes facial freckling and early skin cancers typical of XP and some features typical of CS, such as mental retardation, spasticity, short stature, and hypogonadism. XP-CS does not include skeletal involvement, the facial phenotype of CS, or CNS demyelination and calcifications. We present a rare patient whose genome probably harbored a specific combination of mutations producing a rare double syndrome of XP-CS, with facial phenotype of CS, and CNS demyelination.
Keywords: Xeroderma pigmentosum-cockayne syndrome (XP-CS), demyelination, facial phenotype
How to cite this article:
Singh UR, Asif S, Kommu PP, D'Souza P. Cockayne syndrome-xeroderma pigmentosum complex with demyelination: A rare association. Indian J Hum Genet 2012;18:125-6 |
How to cite this URL:
Singh UR, Asif S, Kommu PP, D'Souza P. Cockayne syndrome-xeroderma pigmentosum complex with demyelination: A rare association. Indian J Hum Genet [serial online] 2012 [cited 2016 Jun 1];18:125-6. Available from: http://www.ijhg.com/text.asp?2012/18/1/125/96681 |
| Introduction | |  |
Cockayne syndrome (CS) is an autosomal recessive disorder characterized by growth failure, severe and progressive neurological deterioration, cachexia, retinal degeneration, and photosensitivity. Xeroderma pigmentosum (XP) patients are characterized by photosensitivity, pigmentation, ophthalmological complications, and development of cutaneous malignancies. [1]
| Case Report | | |
A 6-year-old girl, born of second degree consanguineous marriage, with a birth weight of 3.0 kg, with no postnatal complications, presented with a history of progressive loss of appetite and weight, and regression of developmental milestones for the past 3 years. A younger sibling died at 5 months of age due to intussusception. Another sibling is 3 months old and apparently healthy. Her maternal grandfather and all his brothers are blind (their sister is healthy).
On examination, she weighed 8 kg, her height was 83 cm, and head circumference was 41 cm (all below the third centile). There was generalized wasting, hair was sparse, brittle, coarse, and light colored, and angular stomatitis was present [Figure 1]. Her eyes were deep set, nose was beaked, and she had freckles on her face in a butterfly distribution over the malar area. Dental caries was present. She could sit but not walk, spoke only bisyllables in a staccato manner. She had photophobia, but could recognize her mother. She had generalized hypotonia, and the deep tendon reflexes were not elicitable. Plantar reflexes were flexor bilaterally. She had cerebellar signs, and glabellar tap and palmomental reflexes were elicitable. | Figure 1: Photograph of a child showing freckles, cachexia, sunken eyes and sparse hair
Click here to view |
| Investigations | | |
Blood counts, serum electrolytes, and urine: normal. X-rays: osteopenia, but no skeletal anomalies. Screening for errors of metabolism: normal. Ophthalmological examination: early optic atrophy. Magnetic resonance imaging: diffuse enlargement of all the ventricles, especially the 4th [Figure 2]; cerebellum was atrophic, especially the vermis; hyperintensity seen in centrum semiovale bilaterally in T2 weighted images, suggestive of white matter degeneration. Nerve conduction study: Evidence of demyelination and axonopathy.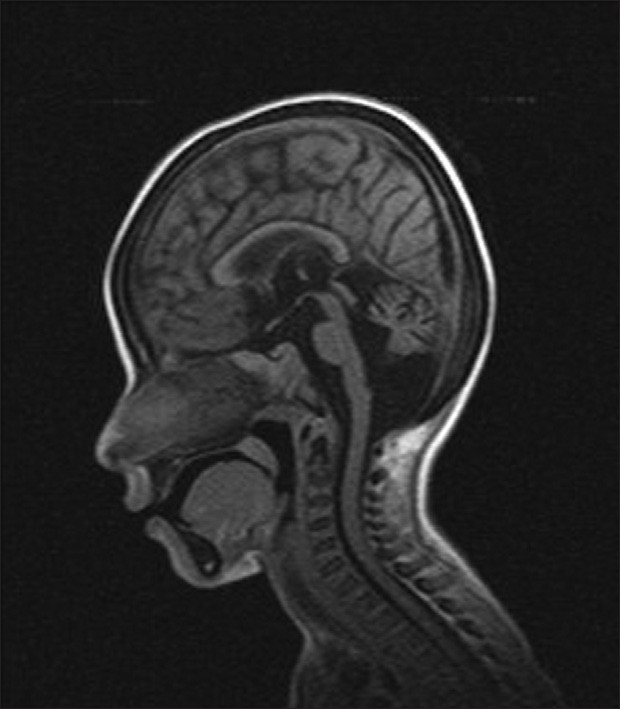 | Figure 2: MRI showing enlargement of 4th ventricle and atrophy of vermis
Click here to view |
| Discussion | | |
The differential diagnosis of CS includes other premature aging syndromes, endocrinopathies, chromosomal anomalies, and metabolic disorders. These were ruled out by routine physical and laboratory examinations.Postnatal growth failure (height and weight < 5 th centile by 2 years) and progressive neurologic dysfunction manifested as early developmental delay are the two major criteria for diagnosing CS. [2],[3],[4] Of the minor criteria required (any three are essential), she had cutaneous photosensitivity with thin, dry hair, optic atrophy, dental caries, and a characteristic physical appearance of "cachectic dwarfism" with thinning of the skin and sunken eyes. Fujimoto et al.[1] reported two cases of XP with additional features of CS with identical mutation (G47R), but they were phenotypically distinct. Since our patient satisfied the criteria of profound postnatal decline of somatic and brain growth (CS), and photosensitivity with ophthalmological complications (XP), [5] we conclude she was a rare case of CS XP complex.
| References | | |
| 1. | Fujimoto M, Leech SN, Theron T, Mori M, Fawcett H, Botta E, et al. Two new XPD patients compound heterozygous for the same mutation demonstrate diverse clinical features. J Invest Dermatol 2005;125:86-92. 
|
| 2. | Gene Reviews; Copyright© 1993-2010. Seattle: University of Washington. [Accessed May 2010].
|
| 3. | Nance MA, Berry SA. Cockayne syndrome: Review of 140 cases. Am J Med Genet 1992;42:68-84.
[PUBMED] |
| 4. | Bartenjev I, Butina MR, Potocnik M. Rare case of Cockayne syndrome with Xeroderma pigmentosum. Acta Derm Venereol 2000;80:213-4.
[PUBMED] |
| 5. | Jones KL, Smith D. Smith's recognizable patterns of human malformations. 6 th ed. Elsevier Saunders Publishers; 2005. p. 154.
|
[Figure 1], [Figure 2]
|









