|
 
 |
|
BRIEF REPORT |
|
|
|
| Year : 2012 | Volume
: 18
| Issue : 2 | Page : 229-232 |
| |
An investigation of Ph 1 chromosome in chronic myeloid leukemia patients with different treatment modalities and hematological features
Koushik Chattopadhyay1, Bibhas Kar2
1 School of Life Sciences, College of Agriculture, Engineering and Science, University of KwaZulu-Natal, Durban, South Africa
2 Department of Medical Genetics, Apollo Hospitals, Chennai, India
| Date of Web Publication | 8-Sep-2012 |
Correspondence Address:
Koushik Chattopadhyay
Flat no. 12, Roseric, 67 Lena Ahrens Road, Bulwer, Durban - 4001
South Africa
 Source of Support: None, Conflict of Interest: None
DOI: 10.4103/0971-6866.100778

 Abstract Abstract | | |
Chronic myeloid leukemia (CML) is characterized by a Ph 1 chromosome that derives through a translocation between chromosomes 9 and 22, i.e., t (9;22). Identifying the Ph 1 chromosome through cytogenetic analysis is an important aspect of CML diagnosis. The aim of this study was to determine the significance of cytogenetic analysis in the diagnosis of CML as well as to find out a relationship between chromosomal abnormalities and CML patients in different stages of treatment. Six CML patients were investigated for this study. The presence of Ph 1 chromosome was detected at different times of treatment using GTG banding on peripheral blood or bone marrow aspirations, and the results were analyzed using cytovision workstation. Hematological features were compared between newly diagnosed patients and patients under treatment. The Ph 1 chromosome was strongly associated with all cases of CML. The regression of Ph 1 chromosomes differed for each patient depending on the treatments and individual response to specific treatments.
Keywords: Chronic myeloid leukemia, haematological, karyotype, Ph 1
How to cite this article:
Chattopadhyay K, Kar B. An investigation of Ph 1 chromosome in chronic myeloid leukemia patients with different treatment modalities and hematological features. Indian J Hum Genet 2012;18:229-32 |
How to cite this URL:
Chattopadhyay K, Kar B. An investigation of Ph 1 chromosome in chronic myeloid leukemia patients with different treatment modalities and hematological features. Indian J Hum Genet [serial online] 2012 [cited 2016 Jun 1];18:229-32. Available from: http://www.ijhg.com/text.asp?2012/18/2/229/100778 |
| Introduction | |  |
Leukemia or leucocythemia is a disease generally regarded as cancer of the blood-forming organs, specifically those concerned with the production of the various white blood cells (WBCs). In this disease, the number of white corpuscles in the blood may be increased. The disease is also characterized by great enlargement of the spleen, by changes in the marrow of the bones, and by enlargement of the lymph glands all over the body. Virtually, every tissue in the body is involved by the leukemia process. leukemia is generally known to people as blood cancer. According to the type of corpuscles chiefly present, it can be divided into two categories; lymphoblastic leukemia and myeloid leukemia. Again, each category is divided into two classes, acute and chronic. [1] Chronic leukemia is the term used to describe a group of malignant diseases of the blood system characterized by the accumulation of abnormal mature-looking white blood cells in the bone marrow and blood. [2] Chronic myeloid leukemia (CML) is a clonal malignant myeloproliferative disorder believed to originate in a single abnormal hematopoietic stem cell. [3] It is a clonal bone marrow disease characterized by neoplastic overproduction of granulocytes. [1] CML is the third most common leukemia, which accounts for approximately 20-25% of adult leukemia. The incidence of CML is greatest between ages of 40 and 60 years, with slightly more men affected by the disease compared to women. CML is characterized by an abnormal chromosome found in the blood cell, an unusually small G-group chromosome, which derives through a translocation of chromosomal material between 22 and the terminal part of the long arm of 9. [2] Scrutiny of prophase - prometaphase chromosomes has shown the breakpoints as 9q34.1 and 22q11.2, i.e. t (9;22) (q34.1;q11.2). [1] This chromosome, called the Philadelphia (Ph 1 ), chromosome is found in 95% of individuals affected by the illness.
Raised white blood cells (30-400 × 10 9 /L) differential count is observed in CML patients. Increased numbers of basophils and eosinophils are also seen. Hemoglobin concentration may be reduced. Nucleated (immature) red cells may be present and platelet count may be raised (300-600 × 10 9 /L). [3] Towards the advanced phase of the disease, white blood cells double much faster than in normal.
Conventional cytogenetics is still the method of choice for identifying the Ph 1 chromosome in CML at diagnosis. Generally, this can be confidently identified on un-banded metaphases. The present study was undertaken to determine the significance of cytogenetic analysis in the diagnosis of CML patients and to determine a relationship between chromosomal abnormalities and CML patients in different stages of treatment.
| Materials and Methods | | |
Subjects
The study was conducted on six patients who were referred to the Medical Genetics unit of Apollo Hospitals (Chennai, India) by different specialists. The ethics approval for the study was obtained from the internal ethics committee of the Apollo Hospitals (Chennai, India). The study was conducted in accordance with the Declaration of Helsinki [4] and Good Clinical Practice (GCP) guidelines. [5]
Slide Preparation for Karyotyping
For cytogenetic diagnosis of CML patients or suspected CML patients, Giemsa banding (also called G-banding or GTG banding) was performed on peripheral blood (PB) or bone marrow aspirations (BMA) obtained from each patient. GTG banded chromosomes from PB or BMA were prepared on slides following the techniques described by Verma and Babu. [6]
Cytovision Work Station
The selected banded metaphases were analyzed and karyotyped using OLYMPUS BX51 (Japan) and software from Applied Imaging (U.K.). Metaphases were karyotyped and interpreted according to the International System for Human Cytogenetic Nomenclature (ISCN). [7]
| Results | | |
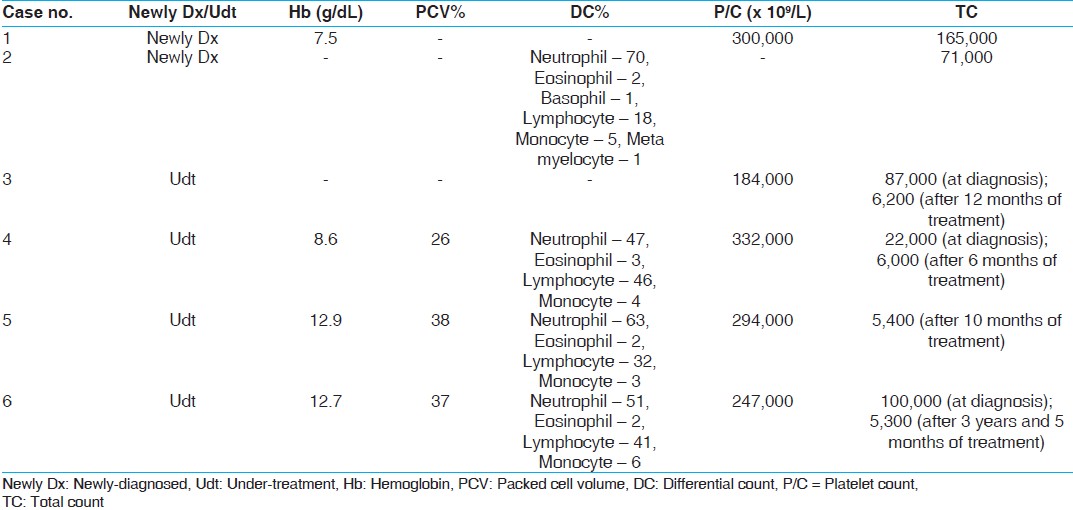
All the patients were of Indian origin, with four male (case no. 1, 2, 3, and 5) and two female (case no. 4 and 6) patients and age ranging between 47 and 57 years [Table 1]. PB or BMA was used for cytogenetic studies. All the patients were found to be in chronic phase of CML. No patient was found in accelerated or blast crisis [Table 1]. Only two patients (case no. 1 and 2) were newly diagnosed and yet to start their treatment program. The rest of the patients were in different stages of treatment [Table 1]. The details of basic characteristics of all the patients including cytogenetic findings at diagnosis and at different stages of treatment have been captured in [Table 1]. The hematological details have been captured in [Table 2].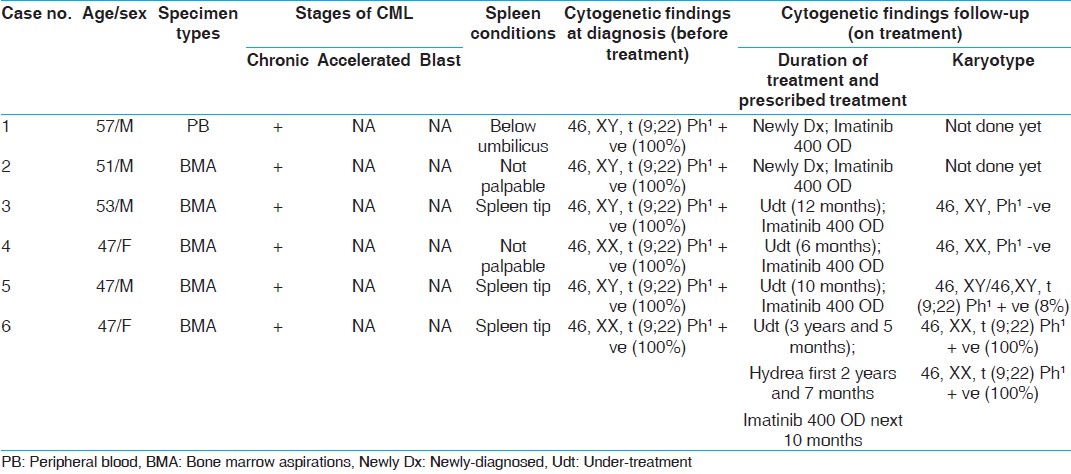 | Table 1: Cytogenetic and clinical details of all Chronic myeloid leukemia patients
Click here to view |
The Ph 1 chromosome is shown in a metaphase plate as visible under microscope [Figure 1]. The cytovision photographs [Figure 2] are showing the differences between chromosomes 9 and 22 from a normal individual [Figure 2]a and from a CML patient [Figure 2]b. | Figure 1: Metaphase plate showing the abnormal Ph1 chromosome (microscope photograph)
Click here to view |
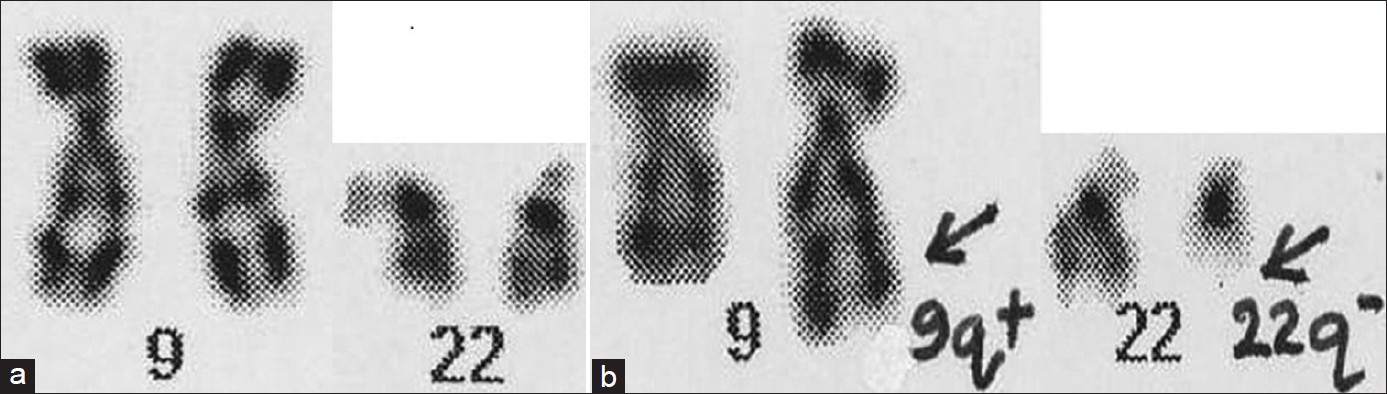 | Figure 2: (a, b) A partial karyotype of chromosomes 9 and 22 from a normal individual (a) and from a CML patient (b) showing a reciprocal translocation in between chromosomes 9 and 22 (cytovision photograph)
Click here to view |
| Discussion | | |
It was found that the presence of spleen differs between the newly diagnosed (before treatment) and patients under treatment and also in between newly diagnosed or patients under treatment.
Only two under-treatment patients (case no. 5 and 6) showed hemoglobin level in between normal range (male: 13-18 gm/dL; female: 12-16 gm/dL). Two other patients (case no. 1 and 4) had a decreased hemoglobin value [Table 2]. As patients 5 and 6 both were under treatment and did not recover fully with patient 6 showing no sign of recovery, the hemoglobin value is hard to explain. Patients 1 and 4 showed a decreased value of hemoglobin. Patient 1 was newly diagnosed and patient 4 was under treatment and had fully recovered. The contrasting hemoglobin value suggests that depending on other physiological conditions the level of hemoglobin fluctuates in an individual and it is not a reliable marker for the disease progression or regression.
The packed cell volume (PCV) data was available only for three patients. Two patients (case no. 5 and 6) showed a marginal decrease from the normal range (39- 49%) and the other patient (case no. 4) demonstrated a massive decrease from the normal range of PCV [Table 2].
The majority of the differential counts (DC) were in the normal range. However, for some patients it did vary. All the patients whether newly-diagnosed or under treatment were found to have normal platelet count (P/C) (150,000-350,000/mL) [Table 2].
The total count (TC) of WBCs gives a very distinct picture when comparing newly diagnosed with under treatment patients. For newly diagnosed patients (case no. 1 and 2), the count is much higher compared with the normal range (4,300-10,800 cells/μL/cu mm) of a healthy individual. The under treatment patients (case no. 3, 4, 5, and 6) also exhibited a high count of TC compared with normal when first diagnosed with CML. However, their count of TC dropped off to normal with the help of medication [Table 2].
It was observed that both the newly diagnosed patients (case no. 1 and 2) had an abnormal karyotype of 46, XY, t (9;22) with the presence of 100% Ph 1 chromosomes; expected for all suspected CML cases [Table 1]. All the patients under treatment (case no. 3, 4, 5, and 6) were found to have 100% Ph 1 chromosomes at the time of first diagnosis of CML [Table 1]. After completion of the treatment, patients 3 and 4 showed a completely normal karyotype with no Ph 1 chromosome (0%) suggestive of a full recovery from the disease. Patient 5 displayed both normal and abnormal cell lines with the presence of 8% Ph 1 chromosomes after going through the treatment prescribed. This suggests a partial recovery for patient 5 from CML and points to continuation of treatment for some more period of time until no sign of Ph 1 chromosome is found in cells. Only patient 6 showed no signs of recovery even after going through two different treatment modalities (Hydrea and Imatinib) and was found to have 100% Ph 1 chromosomes [Table 1].
In conclusion, we can say that the Ph 1 chromosome is strongly associated with CML. Depending on the hematological features and cytogenetic investigations, the treatment modalities for CML differ for different patients. The rate of regression of Ph 1 chromosomes in cells differs in every patient depending on the treatments and individual response to specific treatments.
| Acknowledgements | | |
Mr. G. Perumal (Apollo Hospitals, Chennai, India) helped in preparing slides for karyotyping as well as provided useful inputs in explaining the technical details. Dr. Radha Rajagopalan (Apollo Hospitals, Chennai, India) gave permission for the study and Mr. Mani (Apollo Hospitals, Chennai, India) offered technical help. The Medical Genetics unit of the Apollo Hospitals (Chennai, India) provided funding for the study.
| References | | |
| 1. | Heim S, Mitelman F. Chronic myeloid leukemia. In: Cancer cytogenetics. New York: Alan R. Liss; 1987. p. 41-60. 
|
| 2. | Besa CE, Woermann U. Chronic Myelogenous Leukemia. 2006; Available from: http://www.emedicine.com/med/topic317.htm
|
| 3. | Goldman J. ABC of clinical haematology. Chronic myeloid leukemia. BMJ 1997;314:657-60.
[PUBMED] |
| 4. | World Medical Association (WMA). Policy - World Medical Association Declaration of Helsinki - Ethical principles for medical research involving human subjects. 2004; Available from: http://www.wma.net/e/policy/b3.htm
|
| 5. | International Conference of Harmonisation (ICH). Guideline for Good Clinical Practice -E6 (R1). 1996; Available from: http://www.ich.org/LOB/media/MEDIA482.pdf
|
| 6. | Verma RS, Babu A. Tissue culture techniques and chromosome preparation. In: Human chromosomes: Manual of basic techniques. New York: Pergamon Press; 1989. p. 4-44, 48.
|
| 7. | Mitelman F. ISCN. An International System for Human Cytogenetic Nomenclature. Basel, Switzerland: Krager; 1995.
|
[Figure 1], [Figure 2]
[Table 1], [Table 2]
|