|
 
 |
|
ORIGINAL ARTICLE |
|
|
|
| Year : 2012 | Volume
: 18
| Issue : 2 | Page : 226-228 |
| |
Adjusted classification for ultrasound scoring index for antenatal detection of fetal trisomy
Viroj Wiwanitkit
Wiwanitkit House, Bangkhae, Bangkok, Thailand
| Date of Web Publication | 8-Sep-2012 |
Correspondence Address:
Viroj Wiwanitkit
Wiwanitkit House, Bangkhae, Bangkok-10160
Thailand
 Source of Support: None, Conflict of Interest: None
DOI: 10.4103/0971-6866.100775

 Abstract Abstract | | |
Ultrasound (USG) is a useful investigation in obstetrics. Its mean indications include screening for fetal anomaly, especially for Down's syndrome and other genetic trisomy. Here, the author tries to access the compatibility between classical USG scoring index and the new likelihood ratio-based system. New recommendation on severity of studied markers is given.
Keywords: Index, likelihood ratio, ultrasound
How to cite this article:
Wiwanitkit V. Adjusted classification for ultrasound scoring index for antenatal detection of fetal trisomy. Indian J Hum Genet 2012;18:226-8 |
How to cite this URL:
Wiwanitkit V. Adjusted classification for ultrasound scoring index for antenatal detection of fetal trisomy. Indian J Hum Genet [serial online] 2012 [cited 2016 Jun 1];18:226-8. Available from: http://www.ijhg.com/text.asp?2012/18/2/226/100775 |
| Introduction | |  |
Ultrasound (USG) is a useful investigation in obstetrics. In feto-maternal medicine, fetal assessment during pregnancy is an important activity. [1] The identification of fetal anomaly in utero is an important theme and can be performed based on USG. Its mean indications include screening for fetal anomaly, especially for Down's syndrome and other genetic trisomy. [2],[3] The prenatal detection of those abnormalities often results in some obstetrical management and optimizes care of the fetus and newborn. [4] At present, USG is widely used in antenatal screening. For screening, USG scoring index is classically used. [5] The USG scoring index helps classify the findings into normal (no marker) and abnormal findings. Focusing on abnormal findings, either soft markers (short femur, short humerus, pyelactesis, hyperechoic bowel, choroids plexus cyst, and echogenic intracardiac focus) or major markers (major structural anomalies and nuchal fold thickness) can be seen. However, the diagnostic property of USG investigation in screening for fetal anomaly due to chromosome defects still varies from report to report. Some researches reported very good sensitivity [6,7] while the other reported on only acceptable findings. [8],[9] Garmel and DͲAlton said that "USG examination can diagnose in only approximately 50% of major anomalies." Manning et al. suggested that "It seems more reasonable to expect that continued modification and improvement of the existing fetal profile scoring method with inclusion of new testing techniques will be the steps that will occur to improve testing accuracy." [10] The new system based on likelihood ratio due to age-adjusted ultrasound risk assessment (AAURA) was proposed in 1998. [11] This system classifies the detected abnormalities at different level of likelihood ratios. However, this system is not widely used comparing to the classical classification into soft and major markers. Here, the author tries to access the compatibility between classical USG scoring index and new likelihood ratio-based system. New recommendation on severity of studied markers is given.
| Materials and Methods | | |
First, the author collected the data on the classification system of the classical USG scoring index and new likelihood ratio-based technique. Direct comparison based on the group of abnormalities of USG scoring index was done. The confidence intervals of likelihood ratios corresponding to soft marker and major marker groups were calculated. The overlapping of the confidence intervals in soft marker and major marker groups was determined and used for further adjustment on classical classification system, focused on severity, of present marker in soft marker and major marker groups.
| Results | | |
The comparative assessment of both classification systems was done [Table 1]. According to this work, the confidence intervals of likelihood ratios corresponding to soft marker and major marker groups were equal to 4.3-31.7 and 0-7.5, respectively. The overlapping of the confidence intervals in soft marker and major marker groups was detectable at the range between 4.3 and 7.5. According to the adjustment, the two markers, previously set in soft marker group, "short femur" and "hyperechoic bowel," are recommended to be included in the major marker group [Table 2].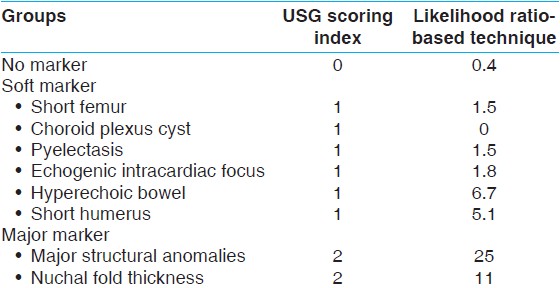 | Table 1: Comparison of ultrasound scoring index and likelihood ratio-based technique for classification of disorder detected by Ultrasound
Click here to view |
| Discussion | | |
Ultrasound evaluation is an important tool in present obstetrics. Mahieu-Caputo et al. said that "One of the major progress in fetal medicine in recent years is the increased sensitivity of sonographic screening for fetal malformations, due to technical improvement but also to a better training of professionals." [12] At present, USG screening for fetal abnormalities is rapidly becoming part of routine antenatal care. [13] The routine anomaly scanning is done in the second trimester but there may be a case for screening at other periods. [13] The clinical usefulness of the USG depends somewhat on the expectations for it. USG is best at detecting malformations, which distort surface anatomy, and it is surely not to be expected to find deep occult anomalies such as imperforate anus or hypospadias. Conversely, detection of overt gross anomalies such as spina bifida or abdominal wall defects is very easy. Since there are several possible findings due to USG investigation ranging from no abnormal observation to gross anomaly, there is a need to have a system to classify the observed findings from screening. USG scoring is the classical tool to serve this purpose. [5],[14] Based on this system, the clustering of markers forms the basis of the scoring index, such that each marker is assigned point values based on the sensitivity and specificity in the detection of fetal anomaly due to chromosome defect, especially for Down's syndrome. [14] Combining the genetic sonogram with maternal serum screening can be a very good method of assessing chromosome defect risk for pregnants who desire such an assessment in the second trimester. [15] Recently, Bromley et al. evaluated the accuracy of the USG scoring index in detecting Down's syndrome fetuses in a high-risk population, and it appeared that this technique could be used to identify approximately 75% of fetuses with Down's syndrome. [16]
Manning concluded that "It seems reasonable to effect continued modification and improvement of the score as a means of antepartum fetal risk assessment." [17] Indeed, the revision of the classical USG scoring system by adding of a new marker has ever been proposed in the medical literature. Absence of the nasal bone is the mentioned marker. [18] However, this marker is difficult to examine [19] and, therefore, not routinely used in general obstetrical practice.
Recently, a new likelihood ratio-based technique was proposed. [11] A good agreement between USG scoring index and new likelihood ratio-based technique was observed by Winter et al.[20] This implies the concordance between the two systems. However, it can be easily observed that the likelihood ratios are variable among disorders within already set soft marker and major marker groups. The new classification of the disorders into soft marker and major marker groups due to the difference in their likelihood ratios can be done and can be helpful in increasing the classical sensitivity of diagnosis. In this work, the author found that there are two markers (short femur and hyperechoic bowel) of classical minor marker group that fell in the overlapping range between confidence intervals in soft marker and major marker groups. Hence, it is suggested that these two disorders should be re-classified into the new major marker groups.
| References | | |
| 1. | Farley D, Dudley DJ. Fetal assessment during pregnancy. Pediatr Clin North Am 2009;56:489-504. 
[PUBMED] |
| 2. | Egan JF. The role of ultrasound in screening for fetal Down syndrome. Curr Womens Health Rep 2002;2:52-8.
[PUBMED] |
| 3. | Wald NJ, Hackshaw AK. Advances in antenatal screening for Down syndrome. Baillieres Best Pract Res Clin Obstet Gynaecol 2000;14:563-80.
[PUBMED] |
| 4. | Garmel SH, D¢Alton ME. Diagnostic ultrasound in pregnancy: An overview. Semin Perinatol 1994;18:117-32.
|
| 5. | Benacerraf BR, Nadel A, Bromley B. Identification of second-trimester fetuses with autosomal trisomy by use of a sonographic scoring index. Radiology 1994;193:135-40.
[PUBMED] |
| 6. | Shirley IM, Bottomley F, Robinson VP. Routine radiographer screening for fetal abnormalities by ultrasound in an unselected low risk population. Br J Radiol 1992;65:564-9.
[PUBMED] |
| 7. | Luck CA. Value of routine ultrasound scanning at 19 weeks: A four year study of 8849 deliveries. BMJ 1992;304:1474-8.
[PUBMED] |
| 8. | Ewigman BG, Crane JP, Frigoletto FD, LeFevre ML, Bain RP, McNellis D. Effect of prenatal ultrasound screening on perinatal outcome. RADIUS Study Group. N Engl J Med 1993;329:821-7.
[PUBMED] |
| 9. | Saari-Kemppainen A, Karjalainen O, Ylöstalo P, Heinonen OP. Ultrasound screening and perinatal mortality: Controlled trial of systematic one-stage screening in pregnancy. The Helsinki Ultrasound Trial. Lancet 1990;336:387-91.
|
| 10. | Manning FA, Harman CR, Menticoglou S, Morrison I. Assessment of fetal well-being with ultrasound. Obstet Gynecol Clin North Am 1991;18:891-905.
[PUBMED] |
| 11. | Nyberg DA, Luthy DA, Resta RG, Nyberg BC, Williams MA. Age-adjusted ultrasound risk assessment for fetal Down's syndrome during the second trimester: Description of the method and analysis of 142 cases. Ultrasound Obstet Gynecol 1998;12:8-14.
[PUBMED] |
| 12. | Mahieu-Caputo D, Senat MV, Romana S, Houfflin-Debarge V, Gosset P, Audibert F, et al. What's new in fetal medicine? Arch Pediatr 2002;9:172-86.
[PUBMED] |
| 13. | Chitty LS. Ultrasound screening for fetal abnormalities. Prenat Diagn 1995;15:1241-57.
[PUBMED] |
| 14. | Bromley B, Benacerraf BR. The genetic sonogram scoring index. Semin Perinatol 2003;27:124-9.
[PUBMED] |
| 15. | Shipp TD, Benacerraf BR. Second trimester ultrasound screening for chromosomal abnormalities. Prenat Diagn 2002;22:296-307.
[PUBMED] |
| 16. | Bromley B, Shipp T, Benacerraf BR. Genetic sonogram scoring index: Accuracy and clinical utility. J Ultrasound Med 1999;18:523-8.
[PUBMED] |
| 17. | Manning FA. The fetal biophysical profile score: Current status. Obstet Gynecol Clin North Am 1990;17:147-62.
[PUBMED] |
| 18. | Lee W, DeVore GR, Comstock CH, Kalache KD, McNie B, Chaiworapongsa T, et al. Nasal bone evaluation in fetuses with Down syndrome during the second and third trimesters of pregnancy. J Ultrasound Med 2003;22:55-60.
[PUBMED] |
| 19. | Malone FD, Ball RH, Nyberg DA, Comstock CH, Saade G, Berkowitz RL, et al.; FASTER Research Consortium. First-trimester nasal bone evaluation for aneuploidy in the general population. Obstet Gynecol 2004;104:1222-8.
[PUBMED] |
| 20. | Winter TC, Uhrich SB, Souter VL, Nyberg DA. The "genetic sonogram": Comparison of the index scoring system with the age-adjusted US risk assessment. Radiology 2000;215:775-82.
[PUBMED] |
[Table 1], [Table 2]
|









