|
 
 |
|
CASE REPORT |
|
|
|
| Year : 2013 | Volume
: 19
| Issue : 1 | Page : 93-95 |
| |
Tuberous sclerosis with rhabdomyoma
V Ajay, Vikram Singhal, Vardhelli Venkateshwarlu, SM Rajesh
Department of Pediatrics, Kasturba Medical College, Manipal University, Mangalore, India
| Date of Web Publication | 4-Jun-2013 |
Correspondence Address:
Vikram Singhal
Department of Pediatrics, KMC Hospital, Attavar, Mangalore - 575 001
India
 Source of Support: None, Conflict of Interest: None
DOI: 10.4103/0971-6866.112912

 Abstract Abstract | | |
Tuberous sclerosis is a neurocutaneous syndrome characterized by abnormalities of both the integument and central nervous system. We present a case of tuberous sclerosis with rhabdomyoma in the heart. This was a 1½-year-old female child with infantile spasms and rhabdomyoma in heart with mother having neurocutaneous markers of tuberous sclerosis. Magnetic resonance imaging brain and electroencephalography findings were consistent with diagnosis.
Keywords: Infantile spasms, neurocutaneous, rhabdomyoma
How to cite this article:
Ajay V, Singhal V, Venkateshwarlu V, Rajesh S M. Tuberous sclerosis with rhabdomyoma. Indian J Hum Genet 2013;19:93-5 |
How to cite this URL:
Ajay V, Singhal V, Venkateshwarlu V, Rajesh S M. Tuberous sclerosis with rhabdomyoma. Indian J Hum Genet [serial online] 2013 [cited 2016 May 24];19:93-5. Available from: http://www.ijhg.com/text.asp?2013/19/1/93/112912 |
| Introduction | |  |
Tuberous sclerosis complex (TSC) is an autosomal dominant neurocutaneous syndrome with a high incidence of sporadic cases and variable clinical expression. [1],[2],[3] It has an estimated frequency of 1/6000. [1],[4] Major manifestations of TSC include skin lesions in more than 95%, autism and seizures in 85%, kidney disease in 60%, mental retardation in 50%, and cardiac rhabdomyoma in 50%. [3] Mental retardation and autism are more in TSC patients who presents with generalized seizures including infantile spasms in the first 2 years of life. [1],[2],[3] We present a 1½-year-old female child with features suggestive of TSC.
| Case Report | | |
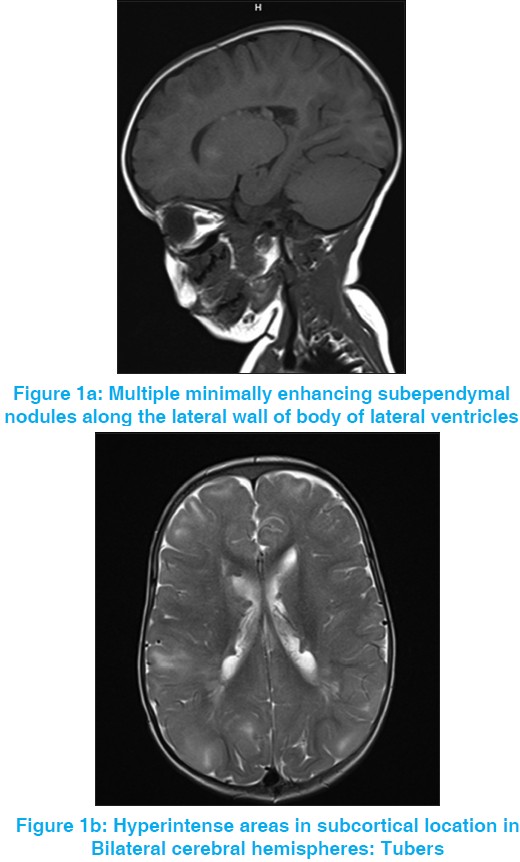
A 1½-year-old female child born out of a non-consanguineous marriage to a primi mother at 34 weeks of gestation, presented with abnormal jerky movements of both upper and lower limb for past 2 months. The development was normal for age, except for speech and language delay. Clinical and central nervous system examination was normal. During hospital stay child was found to have infantile spasms. Electroencephalography (EEG) carried out showed hypsarrhythmic pattern. Magnetic resonance imaging (MRI) brain was suggestive of multiple subependymal nodules and cortical tubers [Figure 1]a and b. Ultrasonogram abdomen was normal. Antenatal scan had revealed a mass in fetal heart in left ventricle. Echocardiography carried out at this admission was suggestive of rhabdomyoma in left ventricular cavity 21 mm × 15 mm size [Figure 2]. Ophthalmological examination was normal. On clinical examination of parents, mother had adenoma sebaceum on face and Shagreen patch in right lumbosacral region. Based on the criteria a diagnosis of TSC was made and child was started on topiramate. There was no further episode of infantile spasms. Now on follow-up the child is seizure free.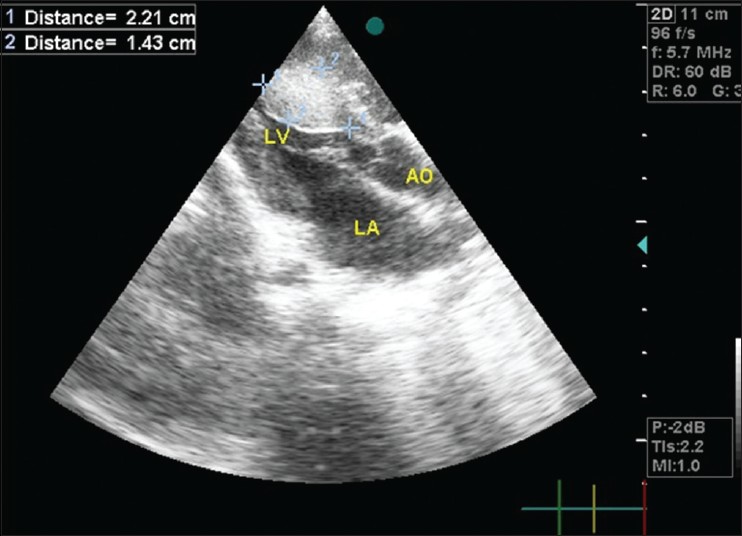 | Figure 2: Echocardiography showing rhabdomyoma in left ventricular cavity 21 mm × 15 mm size
Click here to view |
| Discussion | | |
The first complete description of TSC was given by Bourneville in 1880. [4] TSC is a disorder of cellular differentiation and proliferation that can affect the brain, skin, kidneys, heart, and other organs. Abnormal neuronal migration plays a major additional role in neurological dysfunction. [1] Two genes responsible for TSC are TSC1 at chromosome 9q34 (hamartin) and TSC2 on 16p13.3 (tuberin). [1],[4],[5] Diagnostic criteria include major and minor features.
Major features
- Facial angiofibroma or forehead plaques.
- Non-traumatic ungual or periungual fibroma.
- Shagreen patch (connective tissue nevis).
- Multiple retinal nodular hamartomas.
- Cortical tuber.
- Subependymal nodule.
- Subependymal giant cell astrocytoma.
- Cardiac rhabdomyoma, single or multiple.
- Angiomyolipoma.
Minor features
- Multiple randomly distributed pits in dental enamel.
- Hamartomatous polyps.
- Bone cysts.
- Cerebral white matter radial migration lines.
- Gingival fibromas.
- Non-renal hamartoma.
- Retinal achromic patch.
- "Confetti" skin lesions.
- Multiple renal cysts.
Diagnosis of TSC is established when two major features or one major plus two minor features can be demonstrated (TSC Consensus Conference, 1998). [1],[2],[4],[5]
This child had three of the major features: Subependymal nodules, cortical tubers, and rhabdomyoma.
Recent two-dimensional (2D) ECHO studies have reported that 50% of the patients with TSC have cardiac rhabdomyomas. Incidence of tuberous sclerosis is as high as 59-80% in patients with confirmed fetal rhabdomyomas. [6] Cardiac rhabdomyomas are hamartomas; they tend to be multiple and evidence exists that they involute with time. These lesions sometimes are evident on prenatal ultrasound testing and most of the patients with cardiac dysfunction present soon after birth with heart failure. [6] However, our child has no features suggestive of cardiac involvement except antenatal scan showing a cardiac mass. A few children later develop cardiac arrhythmias or cerebral thromboembolism from the rhabdomyomas. Some patients stabilize after medical treatment with digoxin and diuretics and eventually improve while others require surgery. [6] For existing rhabdomyomas surveillance studies should be done every 6-12 months until stabilization or involution occurs. [1] In TSC vigabatrin is the effective treatment option for infantile spasms. Other drugs which may be useful are topiramate and Adrenocorticotropic hormone. Occasionally, children can discontinue their antiepileptic medication. [1],[2],[4] Oral rapamycin has been shown to cause regression of astrocytomas associated with TSC and may eventually be an alternative to operative therapy. [2],[5] In general in TSC the disease advances so slowly that years must elapse before one can be sure of progression. Of the severe cases, approximately 30% die before the 5 th year and 50-75% before attaining the adult age. The child with infantile spasm is at great risk of later intellectual deficit. [2],[7]
| Conclusion | | |
Any child with fetal rhabdomyoma should be evaluated for TSC. Diagnosed cases should be followed-up regularly with neurodevelopment testing at school entrance, MRI brain, and renal ultrasound every 1-3 years during the childhood and adolescence should be carried out. Other tests such as EEG, ophthalmological examination, and 2D ECHO are repeated only if clinical findings are present.
| References | | |
| 1. | Islam MP, Roach ES. Neurocutaneous syndromes. In: Bradley WG, Daroff RB, Fenichel GM, Jankovic J, editors. Neurology in Clinical Practice. 5 th ed., Vol. 69. Elsevier health sciences Publishers; 2010. p. 1822-7. 
|
| 2. | Gold AP, Patterson MC. Tuberous sclerosis complex. In: Rowland LP, Pedley TA, editors. Merritt's Neurology. 12 th ed., Vol. 109. Lippincott Williams and Wilkins Publishers; 2010. p. 698-704.
|
| 3. | Kandt RS. Tuberous sclerosis complex and neurofibromatosis type 1: The two most common neurocutaneous diseases. Neurol Clin 2002;20:941-64.
|
| 4. | Maria BL, Menkes JH, Sarnat HB. Neurocutaneous syndromes. Child Neurology. 7 th ed., Vol. 12. Lippincott Williams and Wilkins Publishers 2000. p. 810-5.
|
| 5. | Sahin M. Neurocutaneous syndromes. In: Kliegman RM, Stanton BMD, Geme SJ, Schor N, Behrman RE, editors. Nelson Textbook of Paediatrics. 19 th ed., Vol. 589.2. Elsevier Publishers; 2011. p. 2049-51.
|
| 6. | Marx GR. Cardiac tumours. In: Allen HD, Driscoll DJ, Shaddy RE, Felter TF, editors. Moss and Adams Heart Disease in Infants, Children and Adolescents including the Fetus and Young Adult. 5 th ed., Vol. 104. Lippincott Williams and Wilkins Publishers; 1995. p. 1774-6.
|
| 7. | Ropper AH, Samuel MA. Developmental disease of the nervous system. In: Ropper AH, Samuel MA, editors. Adams and Victor's Principles of Neurology. 9 th ed., Vol. 38. McGraw-Hill Professional Publishers; 2009. p. 977-9.
|
[Figure 1], [Figure 2]
|