|
 
 |
|
ORIGINAL ARTICLE |
|
|
|
| Year : 2014 | Volume
: 20
| Issue : 1 | Page : 51-58 |
| |
Paraoxonase1, its Q192R polymorphism and HDL-cholesterol in relation to intensive cardiac care unit stay in ischemic heart disease
Mahesh Harishchandra Hampe, Mukund Ramchandra Mogarekar
Department of Biochemistry, S.R.T.R. Medical College, Ambajogai, District Beed, Maharashtra, India
| Date of Web Publication | 19-May-2014 |
Correspondence Address:
Mahesh Harishchandra Hampe
Preventine Lifecare Pvt. Ltd., RPT House, Plot No. 6, Sector 24, Turbhe, Navi Mumbai, Maharashtra
India
 Source of Support: None, Conflict of Interest: None
DOI: 10.4103/0971-6866.132756

 Abstract Abstract | | |
Aims And Objectives: The present study was evaluated the atheroprotective potential of paraoxonase1 (PON1) and its Q192R polymorphism, to determine whether this polymorphism, which is responsible for differential PON1 activity plays any role in the pathogenesis, severity and extent of coronary artery disease (CAD).
Materials and Methods: This hospital-based cross-sectional study investigated 60 diagnosed cases of CAD and 60 age and gender matched controls. All were assessed for serum PON1 activity, PON1 Q192R polymorphism and for classical cardiovascular risk factors. Individual serum phenotyping for PON1 Q192R polymorphism was determined by double substrate hydrolysis assay. Severity of CAD was assessed by the length of intensive cardiac care unit (ICCU) stay.
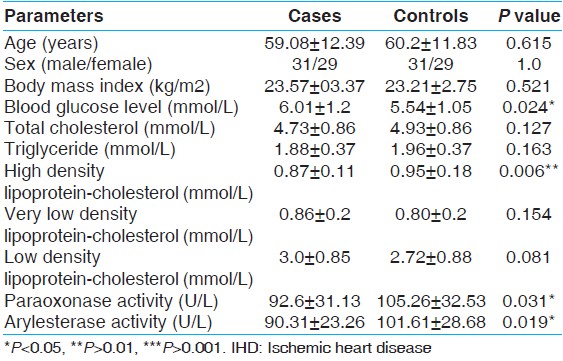
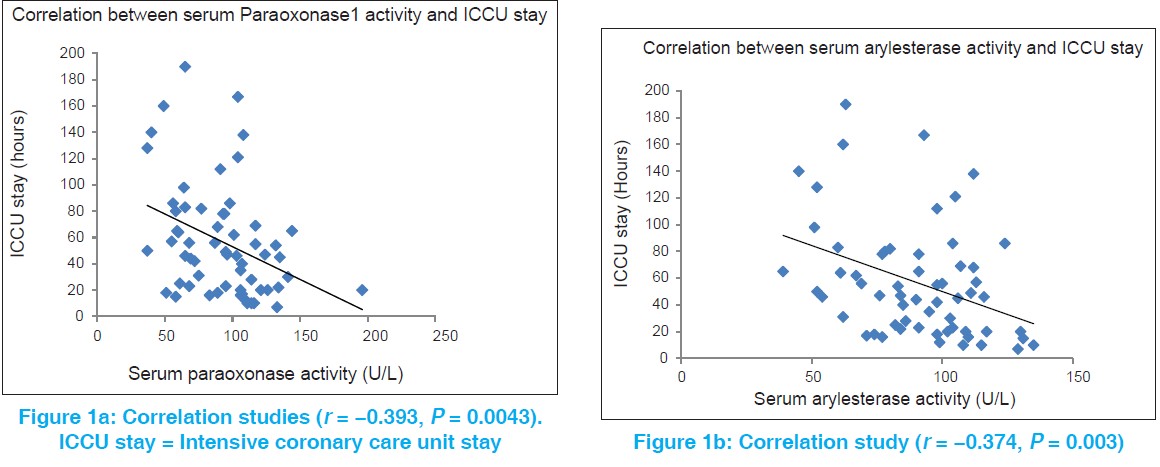
Results: Serum PON1 activity is significantly reduced in cases of CAD (92.6 ± 31.13 IU/L when compared with controls (105.26 ± 32.53 IU/L). Furthermore, serum arylesterase activity is reduced in CAD patients (90.31 ± 23.26 kU) when compared with the control subjects (101.61 ± 28.68 kU). Serum PON1 and arylesterase activities are significantly negatively correlated with the length of ICCU stay (r = −393 and r = −374 respectively). There is no significant difference in the occurrence of CAD and length of ICCU stay among the PON1 phenotypes (P = 0.92). Logistic regression analysis after adjustment of established risk factors revealed no significant association between CAD risk and PON1 Q192R polymorphism (odds ratios: 1.179 [95% confidence intervals: 0.507-2.744], P = 0.702).
Summary And Conclusions: The current study demonstrates that the activity of the PON1 enzyme may be more important factor than the PON1 Q192R polymorphism in the severity and extent of CAD.
Keywords: Coronary artery disease, paraoxonase1, paraoxonase1 Q192R polymorphism
How to cite this article:
Hampe MH, Mogarekar MR. Paraoxonase1, its Q192R polymorphism and HDL-cholesterol in relation to intensive cardiac care unit stay in ischemic heart disease. Indian J Hum Genet 2014;20:51-8 |
How to cite this URL:
Hampe MH, Mogarekar MR. Paraoxonase1, its Q192R polymorphism and HDL-cholesterol in relation to intensive cardiac care unit stay in ischemic heart disease. Indian J Hum Genet [serial online] 2014 [cited 2016 Aug 24];20:51-8. Available from: http://www.ijhg.com/text.asp?2014/20/1/51/132756 |
| Introduction | |  |
Ischemic heart disease (IHD) is a major public health concern and the single leading cause of mortality and morbidity in economically developed countries and is now rapidly assuming serious threat in developing countries like India. [1]
The oxidized low density lipoprotein (oxLDL) is believed to play a central role in atherogenesis. The best known anti-atherogenic function of high density lipoprotein (HDL) is in the reverse cholesterol transport, besides its anti-inflammatory, anti-oxidant and antithrombotic properties. [2] However, it appears that coronary artery disease (CAD) risk is not just merely related to the static plasma HDL-cholesterol (HDL-C) levels, but with the functional characteristics of HDL. [3],[4] Human serum paraoxonase1 (PON1) is present in serum entirely anchored to HDL particles containing apo A-1 and apo J. [5] PON1 has now been reported to have inverse relationship to the risk of cardiovascular diseases (CVD). PON1 hydrolyses a variety of oxidized and modified lipids including oxLDL. PON1 also protects HDL from oxidation and preserves its anti-oxidant function. [6] PON1 gene contains two coding region polymorphism: one at position 192 (Glutamine [Q] to arginine [R] substitution) and another at position 55 (leucine [L] to methionine [M] substitution). [7],[8] PON1 Q192R polymorphism constitutes the molecular basis for interindividual variability. Paraoxon hydrolytic activity is greatest in PON1 RR homozygotes and least with PON1 QQ homozygote individuals. [9] Heterozygotes have intermediate activity. Furthermore, it has been hypothesized that PON1 polymorphism offer differential genetic susceptibility toward risk of CVD. This gave us the insight to investigate PON1 activity and polymorphism in diagnosed cases of IHD and control subjects.
| Materials and Methods | | |
This was a hospital-based cross-sectional study. A total of 60 patients diagnosed as having IHD were included in the study as cases. Confirmation of diagnosis was carried out with history of typical chest pain and specific electrocardiogram (ECG) abnormalities for IHD. Control population consisted of 60 healthy subjects matched for age, gender and attending the routine health check-up in out-patient department. Written valid informed consent was obtained from all subjects. The study was approved by the institutional ethical committee.
The patients with chest pain admitted in the emergency department had undergone physical examination and classical 12 lead ECG taken in supine position according to classical recommendations. [1] History of major systemic illness in the past is obtained by health questionnaire. Signs of old myocardial infarction (MI) are detected by resting ECG. Subjects with previous history of IHD, diabetes, hypertension, renal or hepatic disease, patients on exogenous hormone therapy were excluded. After confirmation of diagnosis, decision is taken by the treating physician for the necessity of admitting the patient in the intensive cardiac care unit (ICCU). After improvement in health, patients are transferred to the general wards. The following criteria used for transferring the patient from ICCU to the general ward.
- Stabilization of vital parameters such as pulse rate, blood pressure etc.
- Repeat ECG showing no evidence of fresh infarct
- Improvement in the general condition of the patient.
The length of ICCU stay in hours was taken as one of the crude measurement of severity of ischemic attack.
All fine chemicals purchased from Sigma Chemical Co. Fasting venous blood collected aseptically from all subjects in the morning. Fasting blood sample collected in fluoride bulb (collected within 24 h in IHD cases) was analyzed within a few hours for estimation of plasma glucose while the remaining blood was allowed to clot in plain bulb. Serum was collected by slow speed centrifugation of clotted blood which was then used for estimation of biochemical parameters. Serum analyzes were estimated using ERBA Smartlab Autoanalyzer.
Serum paraoxonase (PON1) activity assay
1 unit of paraoxonase activity produces 1 nmol of p-nitrophenol and the activity is expressed as U/L based on the molar absorption coefficient (18050 M/cm) at 405 nm at pH 8.0. Intra- and inter-assay coefficients of variation (CVs) are 3.3% and 4.7% respectively. Paraoxon is neurotoxic substance. Therefore safety measures included use of face mask, preparation of required quantity of working reagent in one setting of analysis and treatment of waste water receptacle and pipettes with 2 N NaOH.
Serum arylesterase activity assay
1 unit of arylesterase activity is equal to 1 mM of phenylacetate hydrolyzed per min. The activity is expressed as kU/L, based on the extinction co-efficient of phenol of 1310 M/cm at 270 nm, pH 8.0 and 25°C after correction for non-enzymatic hydrolysis. Intra- and inter-assay CV are 2.4% and 3.7% respectively.
Lipid and lipoprotein measurement
Serum total cholesterol (TC), triglycerides (TG) and HDL-C levels were determined using commercially available kits (Star Diagnostics, India). The LDL-cholesterol (LDL-C) levels were calculated using Friedewald formula. [10]
Paraoxonase polymorphism
Individual serum was phenotyped for PON1 polymorphism by plotting the salt stimulated paraoxonase activity versus arylesterase activity which shows trimodal distribution of study population.
Statistical analysis
Results are presented as mean ± standard deviation. The continuous variables tested for normality with Shapiro-Wilk test. Student's unpaired t-test used for statistical analysis between cases and controls for numerical variables in Gaussian distribution. The strength of association between two parameters is expressed by the Pearson's correlation co-efficient. Allele frequency is evaluated for Hardy-Weinberg equilibrium. χ2 test and Fisher's exact test were performed to compare the frequencies of PON phenotypes between subjects with and without IHD. The logistic regression analysis is used for prediction of risk of IHD contributed by various risk factors. The three models prepared in the logistic regression for the analysis of data are as follows:
Model I: Age, sex, body mass index, smoking status, fasting plasma glucose level, TC, TG, HDL-C, LDL-C (known risk factors).
Model II: All parameters in Model I + Basal PON1 activity.
Model III: All parameters in Model I + PON1 polymorphism.
Subjects are divided into PON1 QQ homozygotes and PON1 R carriers for regression analysis. Odds ratios (ORs) and 95% confidence intervals (CIs) are calculated. P <0.05 is considered as statistically significant. All analyses are carried out with the statistical software Mystat 12 (Systat Software INC, USA) student version.
| Results | | |
[Table 1] shows that among the clinical and lipid parameters, the levels of HDL-C in IHD cases were significantly elevated than in control group. Fasting blood glucose levels were found significantly elevated in cases than in control subjects. Moreover, significantly lower paraoxonase and arylesterase activities were found in cases than in controls.
[Figure 1] shows that serum PON1 and arylesterase activity is significantly negatively correlated with duration of ICCU stay.
[Figure 2] shows that by plotting the graph of the ratio of salt stimulated paraoxonase activity to arylesterase activity versus cumulative frequency of individuals; it shows the trimodal division of the study population by the antimodes at 3.7 and 5.5 [shown by arrows in [Figure 2]a]. According to these antimodes, the study population is divided into 44 individuals with QQ phenotype, 56 individuals with QR phenotype and 20 individuals with RR phenotype [Figure 2]a and b]. The distribution of PON1 phenotypes in cases showed that there are 21 (35%) patients with QQ phenotype, 30 (50%) with QR phenotype and 9 (15%) with RR phenotype. Similarly, controls are divided into three phenotypes as 23 (38.33%) with QQ, 26 (43.33%) with QR and 11 (19.33%) with RR phenotype. There is no significant difference in the distribution of PON1 phenotypes in patients and controls [Table 2].
As shown in [Table 3], ICCU stay among individuals with PON1 phenotypes is statistically not significant (P = 0.92).
Model I of logistic regression is prepared with the known risk factors. When PON1 activity is added in this Model I, the significance of the model increases (from P = 0.021 for Model I to 0.015 for Model II) and it also increases the risk prediction reflected by Naglekerke R2 value from 0.201 to 0.224 showing weak independent association of serum PON1 activity toward CAD risk (OR: 0.989 [95% CI: 0.975 ± 1.003], P = 0.121). Similarly, when Model III is prepared for analysis of the predictive power of PON1 polymorphism, there is no significant association between PON1 polymorphism and IHD risk (OR: 1.179 [95% CI: 0.507-2.744], P = 0.702) [Table 4] after adjustment for all risk factors. Furthermore, the significance of the model and risk prediction does not change when compared with Model I showing no association of PON1 polymorphism in CAD risk.
| Discussion | | |
The cardioprotective function of HDL could be mostly attributed to the enzymes associated with HDL. [11] HDL-associated PON1 enzyme is found to be involved in destroying lipid peroxides. The present study shows statistically significant lower levels of paraoxonase activity in cases than in controls (P = 0.031). Low PON1 activity observed in IHD cases in the present study is consistent with the study done by Navab et al. and Ayub et al. who have found significantly lower activity and concentration of serum PON1 in cases than control group. Furthermore, they observed no significant variation in PON1 activity even 6 weeks after MI. [12],[13]
The present study showed significantly decreased values of baseline serum arylesterase activity of PON1 in cases when compared with control population and significant negative correlation between severity of ischemic attack measured in terms of length of ICCU stay and serum arylesterase activity.
Severity of IHD and PON1 activity
It is assumed that severity of MI is proportional to duration required for the settlement of vital parameters during intensive management. This study expressed significant inverse relationship between PON1 activity and length of ICCU stay of IHD patients. Thus findings of the present study show that PON1 activity as well as arylesterase activity of PON1 is significantly associated with the severity of CAD. Low PON1 activity may reduce the capacity of HDL to prevent oxidation of LDL and may, therefore, lead to IHD. Low PON1 observed in IHD patients may have been present earlier than the coronary event due to its inactivation by increased presence of oxidized lipoproteins in them.
However, the length of ICCU stay among the patients with different PON1 phenotypes does not differ significantly. Granιr et al. in their study obtained similar results while studying PON1 activity and concentration in relation to their extent of angiographic severity of CAD. [14] One Indian study conducted by Jayakumari and Thejaseebai explored the role of arylesterase activity of PON1 and HDL-C levels in angiographically confirmed CAD cases. [15]
Though PON1 activity is significantly decreased in cases than in controls, we observed null relationship between PON1 activity and occurrence of IHD (OR: 0.989, 95% CI: [0.975-1.003], P = 0.121) after adjustment of other established risk parameters of IHD. These findings suggest that the low activity of PON1 observed in IHD is due to other risk factors such as advanced age, increased plasma glucose levels, dyslipidemia. Cao et al. in their study suggested that the ability of PON1 to protect LDL against oxidation was independent of its esterase activity and the Q192R polymorphism. [16] Secondly Aviram et al. in their study suggested that different active sites are involved in paraoxonase/arylesterase activity and protection against LDL oxidation. [17] These data suggest that the protective function of PON1 in coronary atherosclerosis is mediated through the mechanism which is independent of polymorphic esterase activity.
The vast variability in the PON1 activity in the study population can be explained partly by the PON1 polymorphism. The distribution of PON1 alleles among cases and controls are in Hardy-Weinberg equilibrium. Several studies have hypothesized that PON1 RR phenotype is less favorable variant for the risk of developing CVD. However, in present study, there is no significant difference found in the distribution of PON1 phenotypes among cases and controls (P = 0.75). The multivariate study has examined no association between PON1 polymorphism and CAD. Similarly, distribution of homozygous PON1 QQ and PON1 R carriers among the cases and controls is not significant (P = 0.426). [18],[19]
In an article in 1993, Adkins et al. showed that the differential activity of PON1 phenotypes is due to single nucleotide polymorphism at position 192. [8] After this, several independent studies have found the association of PON1 RR phenotype at a higher frequency in CAD in some populations. [20],[21],[22],[23],[24],[25] However, some studies have failed to establish such a relationship. [26],[27],[28],[29],[30],[31],[32],[33],[34],[35],[36],[37] None of the studies have found PON1 R allele negatively correlated with the risk of CAD. Wheeler et al. had carried out meta-analysis of previously published 43 studies and concluded that there is a weak association between PON1 polymorphism and CHD (relative risk: 1.15 [95% CI: 1.09-1.22]). [38] However, this analysis did not take into account the ethnicity and therefore PON1 polymorphism can be the risk factor in particular ethnic groups. These discrepancies in the observations might be due to environmental and methodological factors. Modulation of association between PON1 polymorphism and risk of IHD by gene-environmental and/or gene-gene interactions can be the cause for such diverse results.
Polymorphism in PON1 gene influence both quality and quantity of PON1 enzyme (PON1 status). The quality of PON1 enzyme determines the catalytic efficiency of hydrolysis of paraoxon. In this study, PON1 activity and not PON1 Q192R polymorphism is significantly different in cases and controls. Furthermore, arylesterase activity of PON1 which is representative of PON1 enzyme concentration is also significantly decreased in cases when compared with control subjects. None of the risk factors of CAD analyzed in the study differ significantly amongst the PON1 phenotypes. This indicates that PON1 enzyme status, i.e. activity and concentration, seems to be the better predictors of coronary events and not the PON1 polymorphism. Mackness et al. and Jarvik et al. also showed that PON1 status and not PON1 genotype was associated with CVD. [39],[40]
Regression analysis after adjustment of known risk factors yielded OR of 1.18 (95% CI: [0.507-2.744], P = 0.702) for development of IHD in individuals with PON1 R carriers relative to individuals with PON1 QQ homozygotes. The lack of association of PON1 polymorphism and risk of CAD may be due to physiological role of PON1 which may play minor role in early pathogenesis of IHD but more powerful role in interaction with lipid peroxides which are proposed to be its natural substrates. The reason for the lack of association of PON1 polymorphism may also be due to various residual confounding factors not included in the study design.
The poor association between PON1 Q192R polymorphism and CAD may indicate that this polymorphism is unrelated to coronary atherosclerosis. This polymorphism affects the enzyme activity but this property may be for the artificial substrates like paraoxon and not valid for all substrates.
Thus the findings of the study demonstrate that the atheroprotective effects of HDL may be contributed by PON1 enzyme associated with it. This study strongly suggests that the estimation of HDL-associated PON1 enzyme status provides more valuable information for prediction of risk of future coronary events than static HDL-C levels. Furthermore, the present study shows that the activity of the PON1 enzyme is a more important factor than the PON1 Q192R polymorphism.
There are several potential limitations to the present study. The study is conducted on small sample size. PON1 polymorphism at codon 192 is done by two substrate hydrolysis assay. PON1 genotyping, which is more definitive, is not performed in the present study. So the wrong classification of few individuals among three phenotypes can be possible. Also, the actual concentration of PON1 is not directly estimated in the present study. Further studies are needed to characterize the molecular mechanism by which paraoxonase/arylesterase is involved in cardioprotection. Larger and preferably prospective studies are required to clarify the relationship of PON1 polymorphism and risk of CAD.
| References | | |
| 1. | Antman EM, Selwyn AP, Braunwald E, Loscalzo J. Ischaemic heart disease. In: Longo DL, editor. Harrison's Principles of Internal Medicine. 17 th ed., Vol. 2. USA: The McGraw-Hill Companies Inc.; 2008. p. 1514-27. 
|
| 2. | Calabresi L, Gomaraschi M, Franceschini G. Endothelial protection by high-density lipoproteins: From bench to bedside. Arterioscler Thromb Vasc Biol 2003;23:1724-31.
|
| 3. | Assmann G, Nofer JR. Atheroprotective effects of high-density lipoproteins. Annu Rev Med 2003;54:321-41.
|
| 4. | Trigatti BL, Krieger M, Rigotti A. Influence of the HDL receptor SR-BI on lipoprotein metabolism and atherosclerosis. Arterioscler Thromb Vasc Biol 2003;23:1732-8.
|
| 5. | Durrington PN, Mackness B, Mackness MI. Paraoxonase and atherosclerosis. Arterioscler Thromb Vasc Biol 2001;21:473-80.
|
| 6. | Aviram M, Rosenblat M, Bisgaier CL, Newton RS, Primo-Parmo SL, La Du BN. Paraoxonase inhibits high-density lipoprotein oxidation and preserves its functions. A possible peroxidative role for paraoxonase. J Clin Invest 1998;101:1581-90.
|
| 7. | Humbert R, Adler DA, Disteche CM, Hassett C, Omiecinski CJ, Furlong CE. The molecular basis of the human serum paraoxonase activity polymorphism. Nat Genet 1993;3:73-6.
|
| 8. | Adkins S, Gan KN, Mody M, La Du BN. Molecular basis for the polymorphic forms of human serum paraoxonase/arylesterase: Glutamine or arginine at position 191, for the respective A or B allozymes. Am J Hum Genet 1993;52:598-608.
|
| 9. | Eckerson HW, Wyte CM, La Du BN. The human serum paraoxonase/arylesterase polymorphism. Am J Hum Genet 1983;35:1126-38.
|
| 10. | Friedewald WT, Levy RI, Fredrickson DS. Estimation of the concentration of low-density lipoprotein cholesterol in plasma, without use of the preparative ultracentrifuge. Clin Chem 1972;18:499-502.
|
| 11. | Mackness MI, Durrington PN. HDL, its enzymes and its potential to influence lipid peroxidation. Atherosclerosis 1995;115:243-53.
|
| 12. | Navab M, Hama-Levy S, Van Lenten BJ, Fonarow GC, Cardinez CJ, Castellani LW, et al. Mildly oxidized LDL induces an increased apolipoprotein J/paraoxonase ratio. J Clin Invest 1997;99:2005-19.
|
| 13. | Ayub A, Mackness MI, Arrol S, Mackness B, Patel J, Durrington PN. Serum paraoxonase after myocardial infarction. Arterioscler Thromb Vasc Biol 1999;19:330-5.
|
| 14. | Granér M, James RW, Kahri J, Nieminen MS, Syvänne M, Taskinen MR. Association of paraoxonase-1 activity and concentration with angiographic severity and extent of coronary artery disease. J Am Coll Cardiol 2006;47:2429-35.
|
| 15. | Jayakumari N, Thejaseebai G. High prevalence of low serum paraoxonase-1 in subjects with coronary artery disease. J Clin Biochem Nutr 2009;45:278-84.
|
| 16. | Cao H, Girard-Globa A, Berthezene F, Moulin P. Paraoxonase protection of LDL against peroxidation is independent of its esterase activity towards paraoxon and is unaffected by the Q - >R genetic polymorphism. J Lipid Res 1999;40:133-9.
|
| 17. | Aviram M, Billecke S, Sorenson R, Bisgaier C, Newton R, Rosenblat M, et al. Paraoxonase active site required for protection against LDL oxidation involves its free sulfhydryl group and is different from that required for its arylesterase/paraoxonase activities: Selective action of human paraoxonase allozymes Q and R. Arterioscler Thromb Vasc Biol 1998;18:1617-24.
|
| 18. | Mackness MI, Arrol S, Abbott C, Durrington PN. Protection of low-density lipoprotein against oxidative modification by high-density lipoprotein associated paraoxonase. Atherosclerosis 1993;104:129-35.
|
| 19. | Regieli JJ, Jukema JW, Doevendans PA, Zwinderman AH, Kastelein JJ, Grobbee DE, et al. Paraoxonase variants relate to 10-year risk in coronary artery disease: Impact of a high-density lipoprotein-bound antioxidant in secondary prevention. J Am Coll Cardiol 2009;54:1238-45.
|
| 20. | Ruiz J, Blanché H, James RW, Garin MC, Vaisse C, Charpentier G, et al. Gln-Arg192 polymorphism of paraoxonase and coronary heart disease in type 2 diabetes. Lancet 1995;346:869-72.
|
| 21. | Sentí M, Tomás M, Vila J, Marrugat J, Elosua R, Sala J, et al. Relationship of age-related myocardial infarction risk and Gln/Arg 192 variants of the human paraoxonase1 gene: The REGICOR study. Atherosclerosis 2001;156:443-9.
|
| 22. | Mohamed RH, Mohamed RH, Karam RA, Abd El-Aziz TA. The relationship between paraoxonase1-192 polymorphism and activity with coronary artery disease. Clin Biochem 2010;43:553-8.
|
| 23. | Sanghera DK, Aston CE, Saha N, Kamboh MI. DNA polymorphisms in two paraoxonase genes (PON1 and PON2) are associated with the risk of coronary heart disease. Am J Hum Genet 1998;62:36-44.
|
| 24. | Imai Y, Morita H, Kurihara H, Sugiyama T, Kato N, Ebihara A, et al. Evidence for association between paraoxonase gene polymorphisms and atherosclerotic diseases. Atherosclerosis 2000;149:435-42.
|
| 25. | Wang M, Lang X, Zou L, Huang S, Xu Z. Four genetic polymorphisms of paraoxonase gene and risk of coronary heart disease: A meta-analysis based on 88 case-control studies. Atherosclerosis 2011;214:377-85.
|
| 26. | Mackness B, Durrington P, McElduff P, Yarnell J, Azam N, Watt M, et al. Low paraoxonase activity predicts coronary events in the Caerphilly Prospective Study. Circulation 2003;107:2775-9.
|
| 27. | Troughton JA, Woodside JV, Yarnell JW, Arveiler D, Amouyel P, Ferrières J, et al. Paraoxonase activity and coronary heart disease risk in healthy middle-aged males: The PRIME study. Atherosclerosis 2008;197:556-63.
|
| 28. | Thyagarajan B, Jacobs DR Jr, Carr JJ, Alozie O, Steffes MW, Kailash P, et al. Factors associated with paraoxonase genotypes and activity in a diverse, young, healthy population: The Coronary Artery Risk Development in Young Adults (CARDIA) study. Clin Chem 2008;54:738-46.
|
| 29. | Kerkeni M, Addad F, Chauffert M, Chuniaud L, Miled A, Trivin F, et al. Hyperhomocysteinemia, paraoxonase activity and risk of coronary artery disease. Clin Biochem 2006;39:821-5.
|
| 30. | Herrmann SM, Blanc H, Poirier O, Arveiler D, Luc G, Evans A, et al. The Gln/Arg polymorphism of human paraoxonase (PON 192) is not related to myocardial infarction in the ECTIM Study. Atherosclerosis 1996;126:299-303.
|
| 31. | Aubó C, Sentí M, Marrugat J, Tomás M, Vila J, Sala J, et al. Risk of myocardial infarction associated with Gln/Arg 192 polymorphism in the human paraoxonase gene and diabetes mellitus. The REGICOR Investigators. Eur Heart J 2000;21:33-8.
|
| 32. | Kaman D, Ilhan N, Metin K, Akbulut M, Ustündað B. A preliminary study of human paraoxonase and PON 1 L/M55-PON 1 Q/R 192 polymorphisms in Turkish patients with coronary artery disease. Cell Biochem Funct 2009;27:88-92.
|
| 33. | Turban S, Fuentes F, Ferlic L, Brugada R, Gotto AM, Ballantyne CM, et al. A prospective study of paraoxonase gene Q/R192 polymorphism and severity, progression and regression of coronary atherosclerosis, plasma lipid levels, clinical events and response to fluvastatin. Atherosclerosis 2001;154:633-40.
|
| 34. | Ko YL, Ko YS, Wang SM, Hsu LA, Chang CJ, Chu PH, et al. The Gln-Arg 191 polymorphism of the human paraoxonase gene is not associated with the risk of coronary artery disease among Chinese in Taiwan. Atherosclerosis 1998;141:259-64.
|
| 35. | Antikainen M, Murtomäki S, Syvänne M, Pahlman R, Tahvanainen E, Jauhiainen M, et al. The Gln-Arg191 polymorphism of the human paraoxonase gene (HUMPONA) is not associated with the risk of coronary artery disease in Finns. J Clin Invest 1996;98:883-5.
|
| 36. | Ombres D, Pannitteri G, Montali A, Candeloro A, Seccareccia F, Campagna F, et al. The gln-Arg192 polymorphism of human paraoxonase gene is not associated with coronary artery disease in italian patients. Arterioscler Thromb Vasc Biol 1998;18:1611-6.
|
| 37. | Gardemann A, Philipp M, Hess K, Katz N, Tillmanns H, Haberbosch W. The paraoxonase Leu-Met54 and Gln-Arg191 gene polymorphisms are not associated with the risk of coronary heart disease. Atherosclerosis 2000;152:421-31.
|
| 38. | Wheeler JG, Keavney BD, Watkins H, Collins R, Danesh J. Four paraoxonase gene polymorphisms in 11212 cases of coronary heart disease and 12786 controls: Meta-analysis of 43 studies. Lancet 2004;363:689-95.
|
| 39. | Mackness B, Davies GK, Turkie W, Lee E, Roberts DH, Hill E, et al. Paraoxonase status in coronary heart disease: Are activity and concentration more important than genotype? Arterioscler Thromb Vasc Biol 2001;21:1451-7.
|
| 40. | Jarvik GP, Hatsukami TS, Carlson C, Richter RJ, Jampsa R, Brophy VH, et al. Paraoxonase activity, but not haplotype utilizing the linkage disequilibrium structure, predicts vascular disease. Arterioscler Thromb Vasc Biol 2003;23:1465-71.
|
[Figure 1], [Figure 2]
[Table 1], [Table 2], [Table 3], [Table 4]
|