|
 
 |
|
CASE REPORT |
|
|
|
| Year : 2014 | Volume
: 20
| Issue : 1 | Page : 82-84 |
| |
Poland syndrome
Chandra Madhur Sharma1, Shrawan Kumar2, Manoj K. Meghwani3, Ravi P. Agrawal1
1 Department of Pediatrics, Rama Medical College, Hospital and Research Centre, Kanpur, Uttar Pradesh, India
2 Department of Medicine, Rama Medical College, Hospital and Research Centre, Kanpur, Uttar Pradesh, India
3 Department of T.B. and Chest, Rama Medical College, Hospital and Research Centre, Kanpur, Uttar Pradesh, India
| Date of Web Publication | 19-May-2014 |
Correspondence Address:
Chandra Madhur Sharma
8/218, Flat No. H, Arya Nagar, Kanpur 208 002, Uttar Pradesh
India
 Source of Support: None, Conflict of Interest: None
DOI: 10.4103/0971-6866.132764

 Abstract Abstract | | |
Poland's syndrome is a rare congenital condition, characterized by the absence of the sternal or breastbone portion of the pectoralis major muscle, which may be associated with the absence of nearby musculoskeletal structures. We hereby report an 8-year-old boy with typical features of Poland syndrome, the first documented case from Uttar Pradesh, India.
Keywords: Pectoralis major, Poland syndrome, symbrachydactyly, syndactyly
How to cite this article:
Sharma CM, Kumar S, Meghwani MK, Agrawal RP. Poland syndrome. Indian J Hum Genet 2014;20:82-4 |
| Introduction | |  |
The Poland's syndrome consists of unilateral absence or under development of pectoralis major muscle, hypoplasia of the breast, associated in some cases with agenesis of ipsilateral costal cartilages, athelia and ipsilateral webbing of the fingers. [1] It has reported incidence of 1 in 7000-1 in 100,000 live births with a male preponderance (male: female ratio of 3:1) and is sporadic in nature. [2],[3] Thus it may have varied presentation. In 75% of the cases, hypoplasia is of right hemithorax only. [3] Associated features may include underdevelopment or absence of one nipple and patchy absence of hair in the axilla. In females, there may be underdevelopment or aplasia of one breast and underlying (subcutaneous) tissues. In some cases, associated skeletal abnormalities may also be present, such as underdevelopment or absence of upper ribs, elevation of the shoulder blade (Sprengel deformity) and shortening of the arm with underdevelopment of the forearm bones (i.e., ulna and radius). [4] Other associated abnormalities may include dextrocardia, diaphragmatic hernia and renal anomalies etc. [5]
| Case Report | | |
An 8-year-old school boy presented to us with a flattening of the left anterior chest wall along with hypoplasia and syndactyly of fingers of the left hand since birth. He was the fourth product of non-consanguineous marriage. There was no family history of any congenital disorder. His siblings were all alive and healthy. He has achieved all developmental milestones normally. His scholastic performance was satisfactory. On examination, child was of average built, weighing 27 kg and having a height of 129 cm. Arm span was 122 cm, right side contributing 65 cm and left 57 cm (measured from mid-point of sternum). Others vital were within normal limit. His chest was asymmetrical with hypoplasia of the left side and absence of left anterior axillary fold [Figure 1]. The limbs were asymmetrical, left upper limb was short but had a muscle power 4/5 at all the joints. Ipsilateral fingers were short and webbed (symbrachydactyly) [Figure 2]. Plain skiagram of the chest showed no abnormalities of the ribs or heart but increased lucency over the left side due to the absence of pectoralis major muscle [Figure 3]. Axial computed tomography scan showed the presence of pectoralis major on the right side but not on the left [Figure 4]. X-ray of the affected limb showed hypoplasia of the middle and terminal phalanx along with syndactyly. Echocardiography and abdominal ultrasound were normal. Based on above mentioned anomalies, diagnosis of Poland syndrome was established.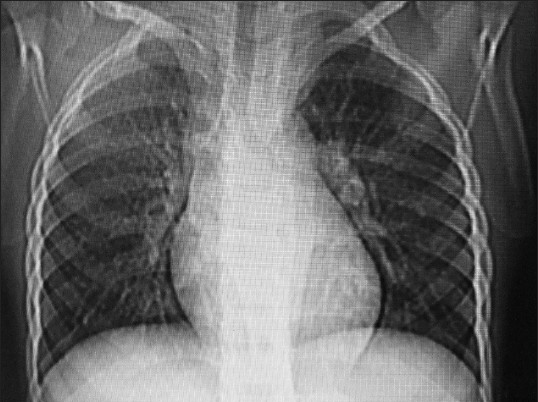 | Figure 3: Plain chest radiography shows increased lucency over the left side due to the absence of chest muscle
Click here to view |
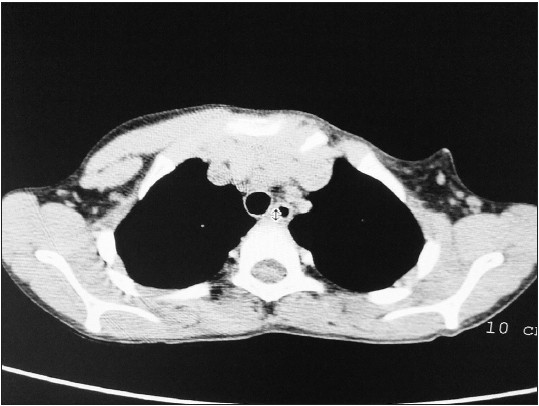 | Figure 4: Axial plain computed tomography scan shows absent pectoralis major on the left side
Click here to view |
| Discussion | | |
Poland syndrome, so named by Patrick Clarkson in 1962 after observing the similarity of his three cases with the one, described by Sir Alfred Poland in 1841. The cause of Poland syndrome is uncertain and it often occurs sporadically. [2],[6] Although some authors have suggested a genetic predisposition but Stevens et al.[7] have reported the presence of Poland syndrome in only one of the two monozygotic twins. Hence there was no purely genetic transmission. The disorder is currently considered "a non-specific developmental field defect" occurring at about the 6 th week of fetal development. It is suggested that, diminished blood flow through the subclavian artery that goes to the arm may be the precipitating cause. This diminished supply affects fetal growth at about the 46 th day of pregnancy, when the fetal fingers and pectoralis muscle are developing. [8] The risk of reappearance of Poland's syndrome in the family is very rare. Poland's syndrome thus can be regarded as a random condition with an extremely low risk of being transmitted from parents to child.
Our case is a classical Poland syndrome as it consists only unilateral aplasia of the pectoralis major muscle and symbrachydactyly of the left side without any other associated defects. However, in our case left hemithorax was involved rather than the usual right side.
The surgical options for chest wall asymmetry depend on anatomical severity, gender, associated anomalies and patient preferences which is generally recommended after the completion of growth. Treatment options include autologous fat injection, pedicled latissimus dorsi muscle transfer, transverse rectus abdominis musculocutaneous flap, custom-made chest wall prosthesis, nipple-areola complex repositioning, mammary prosthesis and sternal/rib reconstruction, or a combination of these techniques. [9]
Our case has good functional activity and does not require any intervention presently.
| References | | |
| 1. | Moir CR, Johnson CH. Poland's syndrome. Semin Pediatr Surg 2008;17:161-6. 
|
| 2. | Legbo JN. Poland's syndrome: Report of a variant. J Natl Med Assoc 2006;98:97-9.
|
| 3. | Gashegu J, Byiringiro JC, Nyundo M. Poland syndrome: A case report. East Cent Afr J Surg 2009;14:112-4.
|
| 4. | Urschel HC Jr. Poland's syndrome. Chest Surg Clin N Am 2000;10:393-403, viii.
|
| 5. | Lacorte D, Marsella M, Guerrini P. A case of Poland Syndrome associated with dextroposition. Ital J Pediatr 2010;36:21.
|
| 6. | Perez Aznar JM, Urbano J, Garcia Laborda E, Quevedo Moreno P, Ferrer Vergara L. Breast and pectoralis muscle hypoplasia. A mild degree of Poland's syndrome. Acta Radiol 1996;37:759-62.
|
| 7. | Stevens DB, Fink BA, Prevel C. Poland's syndrome in one identical twin. J Pediatr Orthop 2000;20:392-5.
|
| 8. | Bavinck JN, Weaver DD. Subclavian artery supply disruption sequence: Hypothesis of a vascular etiology for Poland, Klippel-Feil, and Möbius anomalies. Am J Med Genet 1986;23:903-18.
|
| 9. | Seyfer AE, Fox JP, Hamilton CG. Poland syndrome: Evaluation and treatment of the chest wall in 63 patients. Plast Reconstr Surg 2010;126:902-11.
|
[Figure 1], [Figure 2], [Figure 3], [Figure 4]
|











