|
 
 |
|
CASE REPORT |
|
|
|
| Year : 2014 | Volume
: 20
| Issue : 1 | Page : 85-88 |
| |
Unexpected Inheritance of a Balanced Homologous translocation t(22q;22q) from father to a phenotypically normal daughter
D. K. Chopade1, Harish Harde1, Pallavi Ugale1, Sandesh Chopade2
1 Genetic Health and Research Center, Nashik, India
2 Department of Bio-engineering, Indian Institute of Technology, Kanpur, Uttar Pradesh, India
| Date of Web Publication | 19-May-2014 |
Correspondence Address:
D. K. Chopade
Genetic Health and Research Center, 7, Mahatmanagar, Near ABB Circle, Triambakeshwar Road, Nashik 422 007
India
 Source of Support: None, Conflict of Interest: None
DOI: 10.4103/0971-6866.132765

 Abstract Abstract | | |
Rearrangements between homologous chromosomes are extremely rare and manifest mainly as monosomic or trisomic offsprings. There are remarkably few reports of balanced homologous chromosomal translocation t (22q; 22q) and only two cases of transmission of this balanced homohologous rearrangement from mother to normal daughter are reported. Robersonian translocation carriers in non-homologous chromosomes have the ability to have an unaffected child. However, it is not possible to have an unaffected child in cases with Robersonian translocations in homologous chromosomes. Carriers of homologous chromosome 22 translocations with maternal uniparental disomy do not have any impact on their phenotype. We are presenting a family with a history of multiple first trimester miscarriages and an unexpected inheritance of balanced homologous translocation of chromosome 22 with paternal uniparental disomy. There are no data available regarding the impact of paternal UPD 22 on the phenotype. We claim this to be the first report explaining that paternal UPD 22 does not impact the phenotype.
Keywords: Balanced homologous chromosomal translocation, inheritance, uniparental disomy
How to cite this article:
Chopade DK, Harde H, Ugale P, Chopade S. Unexpected Inheritance of a Balanced Homologous translocation t(22q;22q) from father to a phenotypically normal daughter. Indian J Hum Genet 2014;20:85-8 |
How to cite this URL:
Chopade DK, Harde H, Ugale P, Chopade S. Unexpected Inheritance of a Balanced Homologous translocation t(22q;22q) from father to a phenotypically normal daughter. Indian J Hum Genet [serial online] 2014 [cited 2016 Aug 24];20:85-8. Available from: http://www.ijhg.com/text.asp?2014/20/1/85/132765 |
| Introduction | |  |
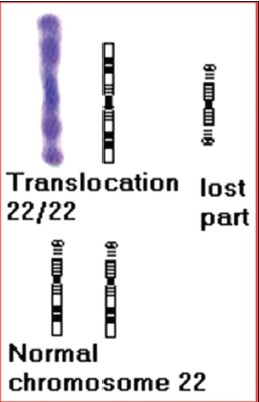
Translocation is a genetic mutation which refers to an exchange of chromosome segments. Translocation is of two types, one which arises by centric fusion of two acrocentric chromosomes called Robertsonian translocation and the other is reciprocal translocation, which involves exchange of two chromosome segments). Two complete acrocentric chromosomes are involved in the centric translocations, and the most common chromosomes found in the Robertsonian translocations are chromosome 13, 14 and 21. [1] The centric translocation of homologous chromosomes can occur between 13;13, 14;14, 15;15, 21;21 and 22;22. The commonly seen homologous chromosomal translocations in live-births are for chromosome 13 and 21. [2] Here we are discussing a case with inherited translocation of homologous chromosome 22 with paternal UPD. With exceptions, a parent with balanced homologous Robertsonian translocations cannot have a normal offspring without chromosomal rearrangement. [3] Transmission of the balanced homologous chromosomal translocation of chromosome 22 has been reported with no impact of the maternal uniparental disomy (matUPD) of chromosome 22. [4],[5],[6] In this study, we report a family with a history of multiple first trimester abortions and the unexpected transmission of the balanced homologous chromosome 22 from father to daughter with the paternal UPD.
| Case Report | | |
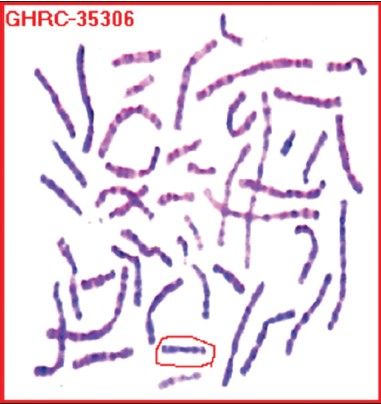
A couple with the history of 7 first trimester miscarriages and a married life of 13 years was referred for genetic counseling. This couple had visited a number of hospitals for treatment. All the routine investigations were found to be normal in their case; however, neither the couple nor any of the abortus was investigated for the chromosomal abnormality. Chromosomal analysis of this couple from peripheral blood culture and trypsin-Giemsa banding was done. Chromosomal complement of the husband (M) was normal 46, XY; however, the chromosomal complement of the wife (S) was found to be abnormal, i.e., 45, XX, t (22;22) [Figure 1], [Figure 2], [Figure 3].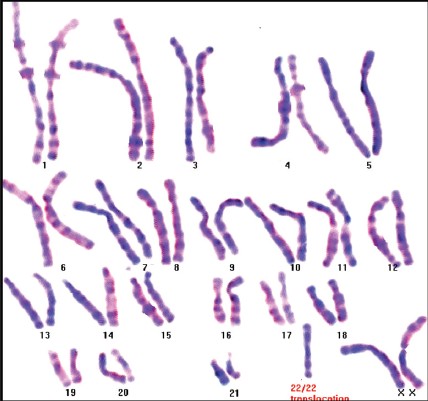 | Figure 1: Karyotype of the daughter(S) showing the balanced homologous chromosomal translocation t (22q;22q)
Click here to view |
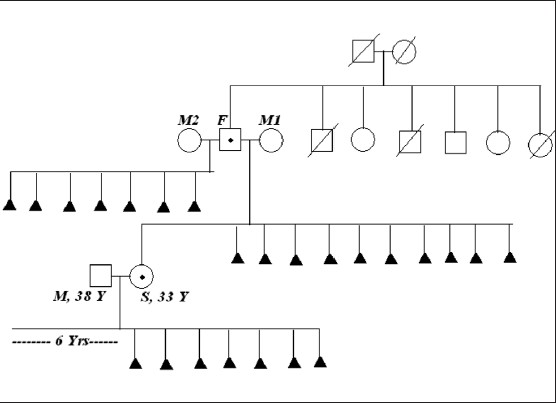
When the family history was taken and the pedigree [Figure 4] was analyzed it was found that she was the only child of her parents, and there was a history of 9 miscarriages to her mother (M1). Thinking that there is a problem with her mother (M1), her father (F) had married with other woman and this step-mother (M2) also had a history of seven first trimester miscarriages without any live birth. Pedigree clearly indicated that S had inherited the balanced translocation from her F. She had six paternal uncles and aunts, and none of them had a history of any infertility, miscarriages or fetal deaths.
Chromosomal analysis of F showed the same 22/22 translocation [Figure 5]. Chromosomes of the paternal grand-parents could not be studied as none of them were alive. Karyotyping of all the paternal uncles and aunts were found to be normal.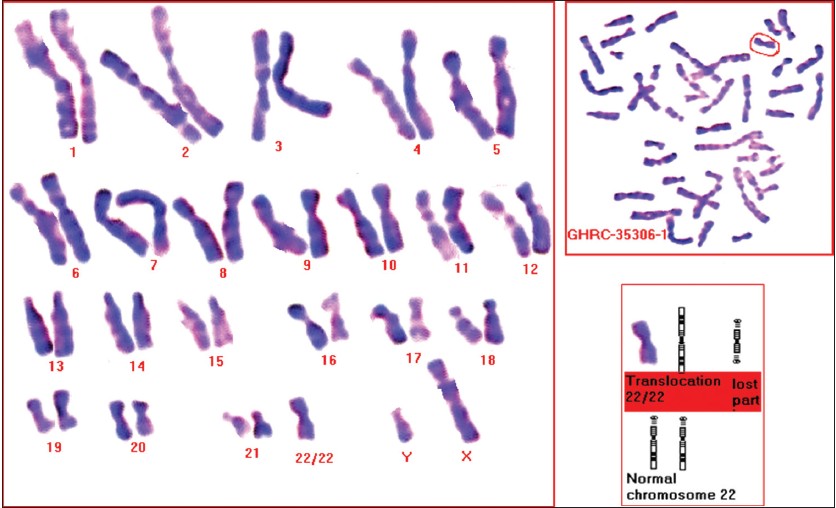 | Figure 5: Karyotype of the father(F) showing the balanced homologous chromosomal translocation t (22q;22q), with a metaphase and the partial karyotype
Click here to view |
| Discussion | | |
In this case, it was clear that the women had inherited the balanced homologous translocation of chromosome 22 from her father and her father had not inherited it from his parents. It was also clear that the multiple miscarriages the women had and her mother and her step mother had were because of this chromosomal rearrangement in her and her parent respectively. Literature search shows that the person with homologous translocation of chromosome 22 has only two possibilities of chromosomal segregation in his/her gametes; [3],[7] one is that of nullisomy and the other of disomy of the translocated chromosome. Translocation formation prevents the normal segregation of chromosome 22 at meiosis during gametogenesis. In such a case, the possibilities would be either a conceptus with monosomy or trisomy for chromosome 22. Conceptuses with monosomy or trisomy 22 are not viable and hence lead to miscarriages in the first trimester. In a carrier with balanced homologous chromosomal translocation, it is accepted that all the viable offspring will be abnormal; and hence the couple is counseled accordingly. [8],[9]
However, in the present family, the phenotypically normal daughter had inherited the balanced homologous chromosomal translocation of chromosome 22 from her father. Theoretically there are two possible ways that will permit this kind of inheritance of the balanced homologous translocation. One of them is the fertilization of a disomic sperm which is carrying translocated chromosome 22 with a nullisomic oocyte.[3] This is theoretically not acceptable due to the low possibility of formation of nullisomic oocyte especially for chromosome 22 during oogenesis. The other possible way is the disomic sperm fertilizing a normal oocyte resulting into the zygote with trisomy 22 and subsequently leading to trisomic rescue by expelling the free maternal chromosome 22. This will result into the conceptus with paternal uniparental disomy for chromosome 22. matUPD 22 does not have any impact on the phenotype. [6] The impact of paternal UPD for chromosome 22 is not reported in the literature as per our knowledge. In this family, the daughter (S) had inherited paternal UPD 22 in a translocated form and was phenotypically perfectly normal. We can conclude from this that paternal UPD for chromosome 22 also does not impact the phenotype.
| References | | |
| 1. | Scriven PN, Flinter FA, Braude PR, Ogilvie CM. Robertsonian translocations: Reproductive risks and indications for preimplantation genetic diagnosis. Hum Reprod 2001;16:2267-73. 
|
| 2. | Oglive C. Rare Chromosome Disorder Support Group, UK Unique Support and Information, 2005.
|
| 3. | Ercis M, Balci S. Can a parent with balanced Robertsonian translocation t (21q;21q) have a non-Down's offspring. Lancet 1999;353:751.
|
| 4. | Palmer CG, Schwartz S, Hodes ME. Transmission of a balanced homologous t (22q;22q) translocation from mother to normal daughter. Clin Genet 1980;17:418-22.
|
| 5. | Kirkels VG, Hustinx TW, Scheres JM. Habitual abortion and translocation (22q;22q): Unexpected transmission from a mother to her phenotypically normal daughter. Clin Genet 1980;18:456-61.
|
| 6. | Schinzel AA, Basaran S, Bernasconi F, Karaman B, Yüksel-Apak M, Robinson WP. Maternal uniparental disomy 22 has no impact on the phenotype. Am J Hum Genet 1994;54:21-4.
|
| 7. | Biricik A, Guney I, Berkil H, Benkhalifa M. A male (15;15) Robertsonian translocation case with 11 previous consecutive recurrent spontaneous abortions. Marmara Med J 2004;17:35-8.
|
| 8. | Mokate T, Leask K, Mehta S, Sharif S, Smith A, Saxena A, et al. Non-mosaic trisomy 22: A report of 2 cases. Prenat Diagn 2006;26:962-5.
|
| 9. | Creasy MR, Crolla JA, Polani PE, Elliott MH. A three chromosome translocation involving two homologous chromosomes in a trisomic abortus. Clin Genet 1976;9:15-9.
|
[Figure 1], [Figure 2], [Figure 3], [Figure 4], [Figure 5]
|