| |


 |
| Year : 2011 | Volume
: 5
| Issue : 2 | Page : 31-37 |
|
|
|
|
|
REVIEW ARTICLE Treatment of adhesive capsulitis with intra-articular hyaluronate: A systematic review
Joshua D Harris, Michael J Griesser, Alex Copelan, Grant L Jones
Department of Orthopaedics, The Ohio State University Sports Medicine Center, OH, Columbus, USA
Correspondence Address:
Joshua D Harris
Department of Orthopaedics, The Ohio State University Medical Center, 2050 Kenny Road, Suite 3300, OH 43221, Columbus
USA
 Source of Support: None, Conflict of Interest: None  | 5 |
DOI: 10.4103/0973-6042.83194

|
|
|
|
| Date of Web Publication | 26-Jul-2011 |
 Abstract Abstract | | |
Sodium hyaluronate injection into the glenohumeral joint is a treatment option in the management of adhesive capsulitis of the shoulder. We hypothesized that a systematic review would demonstrate that intra-articular sodium hyaluronate injections would result in significant improvements in passive range-of-motion, shoulder and general clinical outcome measures, and pain scales at short- and mid-term follow-up. Multiple medical databases were searched for levels I-IV evidence with a priori defined specific inclusion and exclusion study criteria. Clinical outcome measures used included Constant score, VAS pain scores, Cho functional scores, JOA scores, and range-of-motion measurements. Seven studies were included (four Level I and three Level IV; 292 subjects, 297 shoulders). Mean subject age was 59.1 years and mean pre-treatment duration of symptoms was 7.3 months. 140 subjects underwent one or multiple hyaluronate injections (120 glenohumeral joint; 20 subacromial bursa). Clinical follow-up was mean 9.0 weeks. Sodium hyaluronate injection into the glenohumeral joint has significantly improved shoulder range-of-motion, constant scores, and pain at short-term follow-up following treatment of adhesive capsulitis. Isolated intra-articular hyaluronate injection has significantly better constant scores than control. Isolated intra-articular hyaluronate injection has equivalent clinical outcomes and range-of-motion compared to intra-articular corticosteroid injection. Intra-articular hyaluronate injection was safe, with no reported complications within the studies in this review. Sodium hyaluronate injection into the glenohumeral joint is a safe, effective treatment in the management of adhesive capsulitis of the shoulder. Short-term evidence indicates that clinical outcomes are better than control and equivalent to intra-articular corticosteroid injection.
Keywords: Adhesive capsulitis, glenohumeral joint, sodium hyaluronate
How to cite this article:
Harris JD, Griesser MJ, Copelan A, Jones GL. Treatment of adhesive capsulitis with intra-articular hyaluronate: A systematic review. Int J Shoulder Surg 2011;5:31-7 |
| Introduction | |  |
Primary adhesive capsulitis is a common shoulder condition characterized by painful loss of both active and passive range-of-motion in all planes of the glenohumeral joint, especially external rotation. [1] Although the pathogenesis progresses through fibrosis and culminates in joint contracture, [2] it is generally recognized as a self-limiting process [3] with an unknown etiology. [4] Despite reports of 96% to 100% of patients returning to normal shoulder function by two-year and four-year follow-up, [3],[5] some authors have described severe limitations in range-of-motion and persistent pain and weakness at similar durations of follow-up. [6],[7],[8],[9] Nevertheless, several treatments are recognized and utilized to reduce pain and improve range-of-motion faster than the disease's natural history course. These treatments, in isolation or combined, include intra-articular corticosteroid injection into the glenohumeral joint, subacromial corticosteroid injection, intra-articular saline hydrodilation with distention and eventual rupture of the glenohumeral joint capsule, intra-articular sodium hyaluronate injection into the glenohumeral joint, suprascapular nerve block, shoulder manipulation under anesthesia, physical therapy with modalities, oral corticosteroid tapers, oral NSAIDs (non-steroidal anti-inflammatory drugs) and analgesics, and open or arthroscopic surgery with synovectomy and glenohumeral capsular releases. [4]
Sodium hyaluronate injection into the glenohumeral joint for the treatment of adhesive capsulitis has shown similar clinical improvements as those seen following corticosteroid injection with fewer side effects. [10] The effects seen following hyaluronate injection include, but are not limited to, reduction in pain [10] and improved range-of-motion, [10] anti-inflammation, [11] chondroprotection, [11] and improved synovial fluid characteristics. [11]
Primary adhesive capsulitis of the shoulder is usually described as a self-limiting condition that resolves spontaneously by two to four years. [3],[4] However, the natural history is not completely understood and recent studies have shown that longer term disability may occur following "resolution" of the disease. [6],[7],[8],[9] Further, it is not entirely clear how much a specific treatment improves long-term outcomes, if a specific treatment expedites clinical improvement, and if a specific treatment results in faster or better clinical outcomes than other treatments. Sodium hyaluronate is a well-recognized, safe, and minimally invasive treatment that results in improved outcomes in adhesive capsulitis of the shoulder. To the authors' knowledge, no study has fully evaluated the literature reporting clinical outcomes following sodium hyaluronate intra-articular glenohumeral joint injection for the treatment of adhesive capsulitis.
The purpose of this systematic review was to comprehensively analyze the evidence regarding the effectiveness of intra-articular sodium hyaluronate injections in the treatment of primary adhesive capsulitis. We hypothesized that intra-articular sodium hyaluronate injections would result in significant improvements in passive range-of-motion, shoulder and general clinical outcome measures, and pain scales at short- and mid-term follow-up.
| Methods | | |
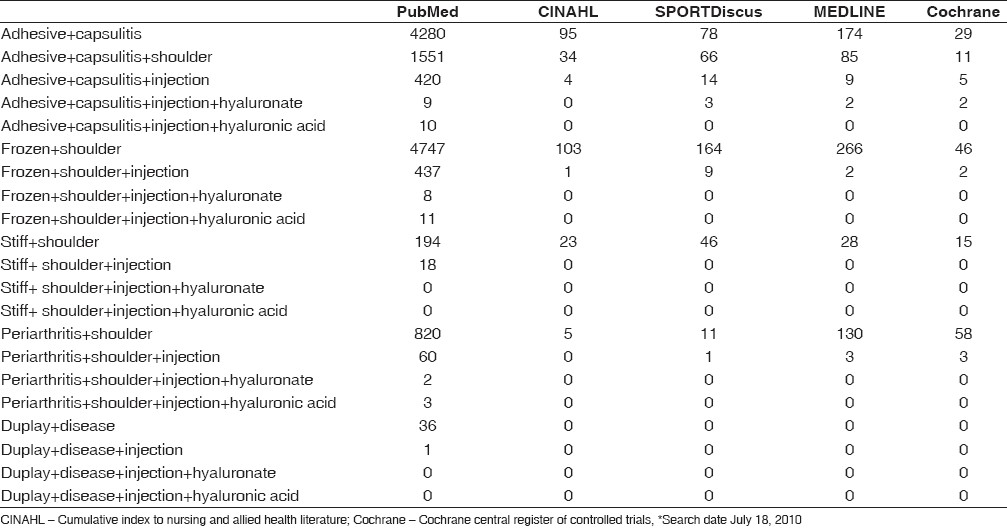
To address our hypotheses, we performed a systematic review of the available medical literature using several medical databases, including PubMed, MEDLINE, CINAHL (Cumulative Index to Nursing and Allied Health Literature), SPORTDiscus with full text, and Cochrane Central Register of Controlled Trials / Database of Systematic Reviews / Methodology Register. The search was independently performed by all three authors (JDH, MJG, GLJ) on July 18, 2010. Database journal search dates ranged from 1950 to the current. Search terms included frozen shoulder, adhesive capsulitis, stiff shoulder, Duplay disease, periarthritis, injection, sodium hyaluronate, hyaluronic acid, Synvisc, and Hyalgan. Levels I, II, III, IV evidence (according to the Oxford Center for Evidence Based Medicine used by the American version of the Journal of Bone and Joint Surgery). [12] Potential inclusive papers were manually reviewed, discussed among authors, and a decision made regarding inclusion or exclusion. In the event of disagreement among authors for study inclusion, the final decision was made by the senior author (GLJ). The full text article was reviewed and reference list checked for potential studies not identified by our original search.
Inclusion criteria were
- Level I, II, III, IV evidence studies
- English language studies
- Human subjects
- Study publication date from January 1, 1950 to July 18, 2010
- Studies investigating treatment of primary adhesive capsulitis (including subjects with diabetes mellitus)
- Studies investigating treatment of primary adhesive capsulitis during the freezing [9] or frozen stage [9]
- Studies investigating intra-articular glenohumeral joint sodium hyaluronate injection
- Studies reporting clinical outcomes following intra-articular glenohumeral joint sodium hyaluronate injection
Exclusion criteria were:
- Level V evidence
- Non-English language studies
- Studies investigating treatment of non-adhesive capsulitis causes of shoulder pain
- Studies investigating treatment of secondary causes of adhesive capsulitis
- Studies investigating treatment of primary adhesive capsulitis during the thawed stage [13]
See [Table 1] for all database search criteria citation results. Fourteen studies were initially retained and analyzed further. Four studies were excluded due to being in a non-English language (Korean, Japanese). [14],[15],[16],[17] One study was excluded as it evaluated the use of hyaluronate for supraspinatus tendinosis and not adhesive capsulitis. [18] One study was excluded as it evaluated the use of subacromial hyaluronate injection for rotator cuff tear arthropathy. [19] One study did treat subjects with adhesive capsulitis, however it did not report clinical outcomes for those subjects, therefore was excluded. [20] Seven studies met inclusion criteria and were further analyzed [1],[10],[21],[22],[23],[24],[25] The inclusion of diabetic subjects within a study was not specifically excluded from our review. Nevertheless, three studies specifically excluded diabetic subjects, [23],[24],[25] one study specifically allowed diabetic subjects, [10] and three studies did not report specifically an approval or denial of diabetic subjects. [1],[21],[22] For the purposes of this review, the control group was defined as no treatment, small volume (<5 mL) intra-articular glenohumeral joint injection of saline or lidocaine.
Subjects were in Stage II adhesive capsulitis, based on classification systems reported by Finnoff [26] or not clinically staged. [1],[21],[22],[23],[24],[25] An attempt was made to identify common outcome measure(s) across all studies analyzed. However, several different clinical outcome measures were used for assessment, including passive range-of-motion (forward elevation, abduction, external rotation, and internal rotation), Cho functional score, [14] visual analog scale (VAS) for pain intensity, [1],[10] constant score, [1] and Japanese Orthopaedic Association (JOA) score. [24] Imaging outcomes (including magnetic resonance imaging and ultrasound) were also recorded when available. Studies, demographic data and treatment data were analyzed with mean, median, mode, and standard deviation calculations, when appropriate. A P-value less than 0.05 was a priori deemed statistically significant. A paired t-test was utilized for outcome data comparison, when possible based on study reporting. The lack of subject-level-specific data and heterogeneity in outcome reporting precluded meta-analysis.
| Results | | |
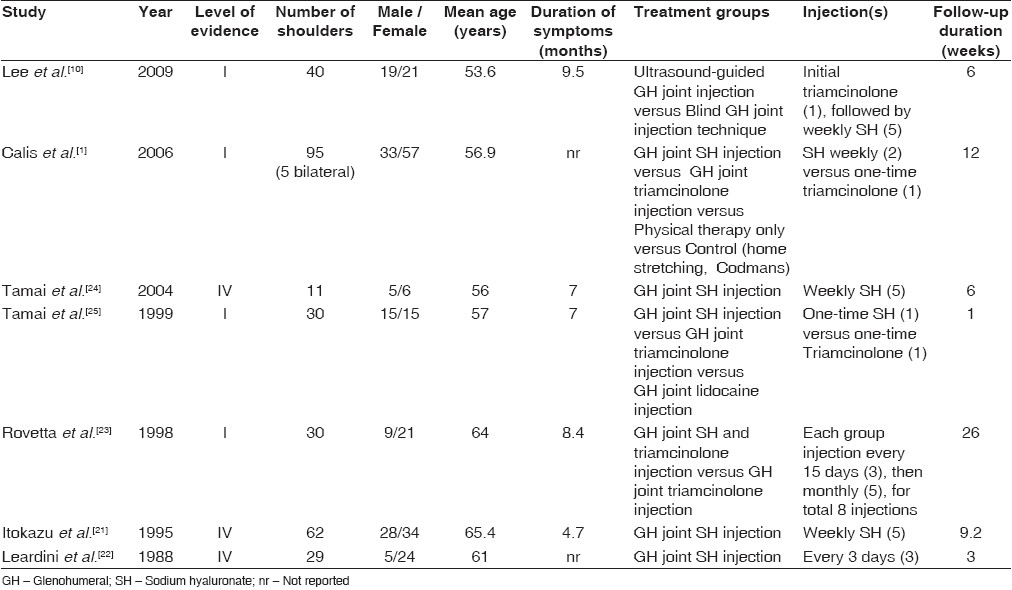
Seven studies met criteria for inclusion (four studies were Level I evidence [1],[10],[23],[24],[25] ; three studies were Level IV evidence [21],[22],[24] ) [Table 2]. Three hundred and three subjects (308 shoulders) were eligible for enrollment within these seven studies. There were 11 subjects who withdrew for various reasons within two studies, [10],[21] leaving 292 subjects (297 shoulders; 5 bilateral cases [1] ) for analysis. Of the four studies that randomized subjects to different treatments, one utilized alternating consecutive selection, [10] one randomized based on date of study entry, [25] and two did not report a randomization method. [1],[23] Six studies [1],[21],[22],[23],[24],[25] did not report the presence or absence of a financial conflict of interest, while one study denied a financial conflict of interest. [10] There were 114 male subjects (39%) and 178 females (61%). Affected shoulder dominance was only reported in one study [1] and this study reported that the affected shoulder was the dominant shoulder in 87 of 90 subjects (97%). Four of seven studies reported the side (right versus left) of the affected shoulder and 104 were right-sided (53%), while 91 were left-sided (47%). Mean pre-treatment duration of symptoms was 7.3 ± 1.8 months (reported in five studies). Mean subject age at the time of treatment initiation was 59.1 ± 4.4 years of age.
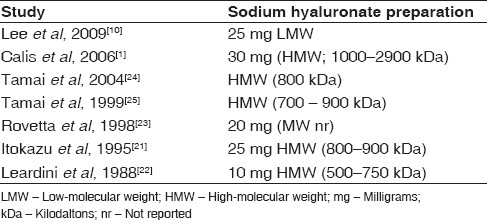
All seven studies included a sodium hyaluronate injection group. One-hundred forty subjects underwent either one or multiple isolated sodium hyaluronate injections (120 intra-articular glenohumeral joint and 20 subacromial bursa). Variable sodium hyaluronate preparations were utilized, including both low molecular weight (LMW; <500 kDa) [10] and high-molecular weight (HMW; >500 kDa) [1],[21],[22],[24],[25] [Table 3]. Fifty subjects underwent one or multiple isolated triamcinolone intra-articular injections. Nine subjects underwent isolated single intra-articular glenohumeral joint lidocaine (1%; 4 mL) injection (control). Forty-three subjects underwent an initial intra-articular glenohumeral joint injection of triamcinolone, followed by five weekly intra-articular glenohumeral joint injections of sodium hyaluronate. Sixteen subjects underwent combined intra-articular glenohumeral joint injections of triamcinolone and sodium hyaluronate. All injections were given via the posterior shoulder. None of the injections were performed with the assistance of fluoroscopy, but 21 were performed with the assistance of ultrasound. The remainder were performed blind. Twenty-two subjects underwent isolated physical therapy consisting of range-of-motion, stretching, hot pack, ultrasound, and TENS (transcutaneous electrical nerve stimulation) modalities and 20 subjects were instructed on Codman exercises and stretches once and asked to perform at home as tolerated as little or as frequently as desired (control). Therefore, two groups (n=29) met the a priori definition of control subjects (small-volume lidocaine intra-articular injection [n=9] and no formal treatment group [n=20]).
Clinical follow-up after treatment was 9.0 ± 8.3 weeks (range 1 to 26 weeks). All seven studies reported at least one clinical outcome measure, while two utilized post-treatment gadolinium-enhanced shoulder MRI [24],[25] and one utilized post-treatment ultrasound. [23] There were no complications reported after any of the treatments.
Following isolated intra-articular glenohumeral joint injection of sodium hyaluronate, constant score significantly improved by 15 days (8 points) and 3 months (20 points) (n=27) (P<0.001); forward elevation significantly improved (22 ± 14 degrees) by 6 weeks (n=91) (P<0.001); abduction significantly improved (21 ± 4.9 degrees) by two to three weeks (n=56) and by two to three months (26 ± 14 degrees) (n=89) (P<0.001, P<0.01); external rotation significantly improved (14 ± 7.1 degrees) by two to three months (n=89) (P<0.001); and internal rotation significantly improved (5 degrees) by two months (n=62).
Following isolated intra-articular glenohumeral joint injection of triamcinolone, constant score significantly improved by 15 days (8 points) and 3 months (15 points) (n=26) (P<0.01). The constant score did not improve after triamcinolone injection as much as after sodium hyaluronate injection, however this difference was not statistically significant. Following isolated intra-articular glenohumeral joint injection of triamcinolone, abduction significantly improved by three to six months (25 ± 9.9 degrees) (n=40) (P<0.01); external rotation significantly improved (20 ± 4.5 degrees) (n=40) (P<0.01) by three to six months; and internal rotation improvement (2 degrees) (n=14) (P>0.05) was not significant. At three to six months, the difference in abduction between intra-articular triamcinolone and hyaluronate was not significant (P=0.942), nor was the difference in external rotation (P=0.463) or internal rotation.
Following combined intra-articular glenohumeral joint injection of hyaluronate and triamcinolone (either simultaneous or subsequent injections), forward elevation significantly improved 47 degrees by 6 weeks post-injection (P<0.05). The difference in forward elevation was not significantly different between combined triamcinolone and hyaluronate versus isolated hyaluronate (P=0.386). Following combined intra-articular injection of hyaluronate and triamcinolone, abduction significantly improved 34 ± 17 degrees by mean 16 weeks post-injection (P<0.05). The difference in abduction was not significantly different between combined triamcinolone and hyaluronate versus isolated hyaluronate (P=0.660). Following combined intra-articular injection of hyaluronate and triamcinolone by mean 16 weeks post-injection, external rotation significantly improved 28 ± 2.8 degrees (P<0.05) and this was significantly greater improvement than hyaluronate injection alone (P=0.039). Following combined intra-articular injection of hyaluronate and triamcinolone by mean 16 weeks post-injection, internal rotation significantly improved 34 ± 11 degrees (P<0.05) and this was significantly greater improvement than hyaluronate injection alone (P=0.031).
Comparison of intra-articular sodium hyaluronate injection and control demonstrated significantly (P<0.05) greater improvement in constant score (20 points versus 10 points) at 3 months post-treatment. The difference in improvement in external rotation by 10 weeks after injection versus control (14 ± 7.1 degrees versus 9 degrees) was not statistically significant (P=0.333), nor was the difference in improvement in abduction by 8 weeks post-injection (25 ± 10 degrees versus 20 degrees) (P=0.346).
| Discussion | | |
The purpose of this systematic review was to comprehensively analyze the literature with regard to the efficacy of intra-articular sodium hyaluronate injections in the treatment of primary adhesive capsulitis. We identified seven studies (four of Level I evidence) that reported clinical outcomes following treatment of adhesive capsulitis with intra-articular hyaluronate injection. Our hypothesis was confirmed, demonstrating that sodium hyaluronate injection into the glenohumeral joint significantly improves shoulder range-of-motion, constant scores, and pain at short-term follow-up following treatment of adhesive capsulitis. Comparison of isolated intra-articular hyaluronate and triamcinolone injections demonstrated that there were no significant differences in constant scores or range-of-motion. Comparison of isolated intra-articular hyaluronate injection and control demonstrated that hyaluronate injections had significantly greater improvement in constant scores. Improvement in range-of-motion following isolated hyaluronate injection was greater than control; however, the difference was not significant. Following combined intra-articular glenohumeral joint injection of hyaluronate and triamcinolone versus isolated hyaluronate, the improvements in range-of-motion after combined injection were significantly greater than isolated hyaluronate in internal and external rotation, but not in abduction or forward elevation.
Hyaluronate is a major component of the extracellular matrix of articular cartilage. The intertwined scaffold network between hyaluronate and aggrecan proteoglycans containing keratan sulfate and chondroitin sulfate glycosaminoglycans is a major mechanical structure within joint cartilage. This known biological composition prompted the use of different preparations of viscosupplementation in the treatment of knee osteoarthritis and has demonstrated success. [27],[28] The anti-adhesive properties of hyaluronate have found utility in preventing postoperative adhesions in gynecologic and abdominal surgery. [29],[30],[31],[32] These lubricating effects of hyaluronate have led to use in orthopedic surgery as well, via prevention of adhesion formation after both wrist and finger flexor tendon repair [33],[34],[35],[36],[37],[38] and tenolysis. [39] Use of hyaluronate in the treatment of shoulder pain has also yielded success. [1],[10],[20],[21],[22],[23],[24],[25],[40],[41] Thus, extrapolation to treatment of stiff shoulder and adhesive capsulitis has demonstrated success and improvements in range-of-motion, pain, and function. [1],[10],[21],[22],[23],[24],[25]
Six different preparations are commonly used in the United States and are both avian- and bacterial-derived products of variable molecular weight and viscosity. The normal hyaluronate molecule (mean 800 kDa [11] to 5000 kDa [42] molecular weight) has similar molecular weight and viscosity to these commercial products (500 kDa to 6000 kDa molecular weight). Hyaluronate injection into synovial joints is safe. [20],[43],[44] Our review further supported this, with no complications in any of the seven studies analyzed. Further, intra-articular injection of corticosteroid may elevate blood glucose levels in diabetic patients, thus warranting vigilance and careful monitoring of blood glucose concentrations and likely adjustments of insulin requirements. Hyaluronate may serve as a viable, equally efficacious alternative to corticosteroid to avoid the risk of elevated blood glucose level following injection.
Despite incomplete understanding, evidence of mechanism of action in the treatment of osteoarthritis is based on several theories: Reduction of friction via increased viscoelasticity with injection of hyaluronate into the joint, [27] coating and protecting damaged cartilage, [11] anti-inflammation [45] and subsequent pain reduction, [15],[23] and improved synovial fluid concentrations and synovium abnormalities. [24],[25] Gadolinium-enhanced MRI in the shoulders of adhesive capsulitis patients has shown significant signal enhancement in the synovium and subsequent attenuation of this hyperintensity with treatment. [24],[25] A calculated value, the coefficient of enhancement (CE), using this latter MRI technique, has been shown to negatively correlate with clinical improvements. [24] Glenohumeral intra-articular injection with hyaluronate has shown improved clinical outcome and decreased MRI CE values. Since decreased CE is indicative of decreased synovitis, transitivity indicates intra-articular hyaluronate is anti-inflammatory. [24]
Despite the Level 1 evidence nature of four of the studies within this systematic review, several limitations are present. Properly conducted randomization attempts to eliminate selection bias and support the internal validity of a study. [46] None of the four studies that randomized patients within this review utilized a valid randomization method. Further, it was not directly stated whether or not the study authors were involved in the randomization of subjects. Another source of selection bias includes unequal numbers of subjects within each compared group. The control group defined within one study [1] in the analyzed studies in the review and a priori defined for the review yielded a control population of 10% of the overall analyzed subject population within the review.
The presence of concurrent intervention (performance bias) confounders within the studies limits conclusions drawn. These include concomitant intra-articular steroid injection preceding five weekly hyaluronate injections, [10] concomitant low-volume intra-articular injections of local anesthetic and saline, [10],[24],[25] subacromial versus intra-articular glenohumeral joint injection in one study, [21] and different physical therapy regimens following injection among all studies or the presence / absence of physical therapy in one study. [21] The accuracy of blind intra-articular glenohumeral joint injection ranges from 33% to 47%, versus 93% accuracy with assistance of ultrasound. [47] The use of imaging in intra-articular injection may be necessary to optimize true results. Use of ultrasound was only present in one study. [10] Assessment of range-of-motion via goniometer (as was done in only two studies in this review [1],[10] ) has high intra-tester reliability (though, is limited by the tester's experience and ability to properly identify bony landmarks) but only fair to moderate inter-tester reliability. [48] Nevertheless, range-of-motion measurement was either not reported or visually assessed in 5 out of the 7 included studies, despite recommendations for calibrated goniometer use in the performance of high-level evidence. [48] Dissimilar doses, molecular weights, and viscosities of the different hyaluronate preparations introduce further bias. Also, incomplete understanding of the true natural history of adhesive capsulitis precludes definitive conclusions on how treatment affects the course of disease.
Assessment of outcomes via an independent observer is necessary to minimize detection bias. However, independent evaluators of clinical outcome or range-of-motion following treatment were utilized in only three of seven studies. [1],[10],[23] Heterogeneity in outcome measures used in the 7 studies within this review precludes meta-analysis and complete assimilation of data for larger sub-group subject numbers and comparisons. The best assessment of an orthopedic disease process and its response to treatment is via a general health outcome tool and a joint- or body-part-specific outcome tool. The primary outcome measures used in the studies analyzed were shoulder range-of-motion and constant score, [1],[10] Cho function score, [10] JOA score, [24],[25] and variable VAS pain scores. [1],[10],[21],[22],[23] A general health assessment tool was not utilized in any of the studies within this review.
A significant limiting factor in this review is the very short-term follow-up duration (minimum one week to maximum 26 week follow-up). Although the natural history of adhesive capsulitis is incompletely understood, it is well-recognized that regardless of treatment most patients achieve their maximal outcome between two to four years after following treatment. [3],[5] Despite this, studies have demonstrated severe loss of motion, inability to perform activities of daily living, and mild residual pain and weakness at longer term follow-up (up to seven years). [6],[7],[8],[9]
| Conclusion | | |
This systematic review showed that sodium hyaluronate injection into the glenohumeral joint significantly improves shoulder range-of-motion, constant scores, and pain at short-term follow-up following treatment of adhesive capsulitis. Isolated intra-articular hyaluronate injection has significantly better outcomes than control. Isolated intra-articular hyaluronate injection has equivalent outcomes compared to intra-articular corticosteroid injection. Intra-articular hyaluronate injection was safe, with no reported complications within the studies in this review.
| References | | |
| 1. | Calis M, Demir H, Ulker S, Kirnap M, Duygulu F, Calis HT. Is intraarticular sodium hyaluronate injection an alternative treatment in patients with adhesive capsulitis? Rheumatol Int 2006;26:536-40. 
|
| 2. | Neviaser J. Adhesive capsulitis of the shoulder. J Bone Joint Surg Am 1945;27:211-22.
|
| 3. | Grey RG. The natural history of "idiopathic" frozen shoulder. J Bone Joint Surg Am 1978;60:564.
|
| 4. | Neviaser AS, Hannafin JA. Adhesive capsulitis: A review of current treatment. Am J Sports Med 2010;38:2346-56.
|
| 5. | Miller MD, Wirth MA, Rockwood CA Jr. Thawing the frozen shoulder: The "patient" patient. Orthopedics 1996;19:849-53.
|
| 6. | Binder AI, Bulgen DY, Hazleman BL, Roberts S. Frozen shoulder: A long-term prospective study. Ann Rheum Dis 1984;43:361-4.
|
| 7. | Hand C, Clipsham K, Rees JL, Carr AJ. Long-term outcome of frozen shoulder. J Shoulder Elbow Surg 2008;17:231-6.
|
| 8. | O'Kane JW, Jackins S, Sidles JA, Smith KL, Matsen FA 3rd. Simple home program for frozen shoulder to improve patients' assessment of shoulder function and health status. J Am Board Fam Pract 1999;12:270-7.
|
| 9. | Shaffer B, Tibone JE, Kerlan RK. Frozen shoulder. A long-term follow-up. J Bone Joint Surg Am 1992;74:738-46.
|
| 10. | Lee HJ, Lim KB, Kim DY, Lee KT. Randomized controlled trial for efficacy of intra-articular injection for adhesive capsulitis: Ultrasonography-guided versus blind technique. Arch Phys Med Rehabil 2009;90:1997-2002.
|
| 11. | Iwata H. Pharmacologic and clinical aspects of intraarticular injection of hyaluronate. Clin Orthop Relat Res 1993;289:285-91.
|
| 12. | Obremskey WT, Pappas N, Attallah-Wasif E, Tornetta P 3rd, Bhandari M. Level of evidence in orthopaedic journals. J Bone Joint Surg Am 2005;87:2632-8.
|
| 13. | Reeves B. The natural history of the frozen shoulder syndrome. Scand J Rheumatol 1975;4:193-6.
|
| 14. | Cho K, Song J, Lee H, Kim J, Rhee Y. The effect of subacromial bursa injection of hyaluronate in patients with adhesive capsulitis of shoulder joint: Multicenter, prospective study. J Korean Acad Rehab Med 2002;26:73-80.
|
| 15. | Kim H, Kim H, Ahn K. The effect of intraarticular injection of hyaluronic acid and steroid in adhesive capsulitis of shoulder. J Korean Acad Rehab Med 1999;23:117-23.
|
| 16. | Takagishi N, Minamikawa H, Iwamoto H, Kida H, Okuyama S, Tanaka M. Clinical evaluation of SPH (high molecular weight sodium hyaluronate) on periarthritis of the shoulder, Jpn J Pharmacol Ther 1998;16;3553-67.
|
| 17. | Yamamoto R, Namiki O, Iwata H, Shinmei M, Mikasa M, Ogawa N. Randomized cooperative study of sodium hyaluronate (SPH) on perarthritis scapulohumeralis, Jpn J Pharmacol Ther 1988;19:717-33.
|
| 18. | Meloni F, Milia F, Cavazzuti M, Doria C, Lisai P, Profili S, et al. Clinical evaluation of sodium hyaluronate in the treatment of patients with sopraspinatus tendinosis under echographic guide: experimental study of periarticular injections. Eur J Radiol 2008;68:170-3.
|
| 19. | Tagliafico A, Serafini G, Sconfienza LM, Lacelli F, Perrone N, Succio G, et al. Ultrasound-guided viscosupplementation of subacromial space in elderly patients with cuff tear arthropathy using a high weight hyaluronic acid: prospective open-label non-randomized trial. Eur Radiol 2010;21:182-7.
|
| 20. | Blaine T, Moskowitz R, Udell J, Skyhar M, Levin R, Friedlander J, et al. Treatment of persistent shoulder pain with sodium hyaluronate: A randomized, controlled trial. A multicenter study. J Bone Joint Surg Am 2008;90:970-9.
|
| 21. | Itokazu M, Matsunaga T. Clinical evaluation of high-molecular-weight sodium hyaluronate for the treatment of patients with periarthritis of the shoulder. Clin Ther 1995;17:946-55.
|
| 22. | Leardini G, Perbellini A, Franceschini M, Mattara L. Intra-articular injections of hyaluronic acid in the treatment of painful shoulder. Clin Ther 1988;10:521-6.
|
| 23. | Rovetta G, Monteforte P. Intraarticular injection of sodium hyaluronate plus steroid versus steroid in adhesive capsulitis of the shoulder. Int J Tissue React 1998;20:125-30.
|
| 24. | Tamai K, Mashitori H, Ohno W, Hamada J, Sakai H, Saotome K. Synovial response to intraarticular injections of hyaluronate in frozen shoulder: A quantitative assessment with dynamic magnetic resonance imaging. J Orthop Sci 2004;9:230-4.
|
| 25. | Tamai K, Yamato M, Hamada J, Mashitori H, Saotome K. Response of frozen shoulder to intraarticular corticosteroid and hyaluronate: A quantitative assessment with dynamic magnetic resonance imaging. Dokkyo J Med Sci 1999;26:235-41
|
| 26. | Finnoff J. Musculoskeletal problems of the upper limb. Philadelphia, Pa.: Saunders; 2007.
|
| 27. | Altman RD, Moskowitz R. Intraarticular sodium hyaluronate (Hyalgan) in the treatment of patients with osteoarthritis of the knee: A randomized clinical trial. Hyalgan Study Group. J Rheumatol 1998;25:2203-12.
|
| 28. | Wang CT, Lin J, Chang CJ, Lin YT, Hou SM. Therapeutic effects of hyaluronic acid on osteoarthritis of the knee. A meta-analysis of randomized controlled trials. J Bone Joint Surg Am 2004;86-A:538-45.
|
| 29. | Ahmad G, Duffy JM, Farquhar C, Vail A, Vandekerckhove P, Watson A, et al. Barrier agents for adhesion prevention after gynaecological surgery. Cochrane Database Syst Rev 2008;16:CD000475.
|
| 30. | Becker JM, Dayton MT, Fazio VW, Beck DE, Stryker SJ, Wexner SD, et al. Prevention of postoperative abdominal adhesions by a sodium hyaluronate-based bioresorbable membrane: A prospective, randomized, double-blind multicenter study. J Am Coll Surg 1996;183:297-306.
|
| 31. | Mais V, Bracco GL, Litta P, Gargiulo T, Melis GB. Reduction of postoperative adhesions with an auto-crosslinked hyaluronan gel in gynaecological laparoscopic surgery: A blinded, controlled, randomized, multicentre study. Hum Reprod 2006;21:1248-54.
|
| 32. | Sutton C. Adhesions following surgery: pathogenesis and current experience with adhesion barriers. Surg Technol Int 2009;18:144-56.
|
| 33. | Hagberg L. Exogenous hyaluronate as an adjunct in the prevention of adhesions after flexor tendon surgery: A controlled clinical trial. J Hand Surg Am 1992;17:132-6.
|
| 34. | Hagberg L, Gerdin B. Sodium hyaluronate as an adjunct in adhesion prevention after flexor tendon surgery in rabbits. J Hand Surg Am 1992;17:935-41.
|
| 35. | Hu J. Barrier effects of various high polymer biomaterials on prevention of tendon adhesion: A systemic evaluation. J Clin Rehab Tissue Eng Res 2008;13:5793-7.
|
| 36. | Isik S, Ozturk S, Gurses S, Yetmez M, Güler MM, Selmanpakoðlu N, et al . Prevention of restrictive adhesions in primary tendon repair by HA-membrane: Experimental research in chickens. Br J Plast Surg 1999;52:373-9.
|
| 37. | Miller JA, Ferguson RL, Powers DL, Burns JW, Shalaby SW. Efficacy of hyaluronic acid/nonsteroidal anti-inflammatory drug systems in preventing postsurgical tendon adhesions. J Biomed Mater Res 1997;38:25-33.
|
| 38. | Weiss C, Suros JM, Michalow A, Denlinger J, Moore M, Tejeiro W. The role of Na-hylan in reducing postsurgical tendon adhesions: Part 2. Bull Hosp Jt Dis Orthop Inst 1987;47:31-9.
|
| 39. | Karakurum G, Buyukbebeci O, Kalender M, Gulec A. Seprafilm interposition for preventing adhesion formation after tenolysis. An experimental study on the chicken flexor tendons. J Surg Res 2003;113:195-200.
|
| 40. | Brander VA, Gomberawalla A, Chambers M, Bowen M, Nuber G. Efficacy and safety of hylan G-F 20 for symptomatic glenohumeral osteoarthritis: a prospective, pilot study. PM R 2010;2:259-67.
|
| 41. | Fernandez-Palazzi F, Viso R, Boadas A, Ruiz-Sáez A, Caviglia H, De Bosch NB. Intra-articular hyaluronic acid in the treatment of haemophilic chronic arthropathy. Haemophilia 2002;8:375-81.
|
| 42. | Aviad AD, Houpt JB. The molecular weight of therapeutic hyaluronan (sodium hyaluronate): how significant is it? J Rheumatol 1994;21:297-301.
|
| 43. | Nakagawa K, Nozaki F, Sugawara H, Suzuki K, Yamaguchi T. Antigenicity studies on sodium hyaluronate (SPH) Part 1: experiments in guinea pig. JPN J Pharmacol Ther 1984;12:141-50.
|
| 44. | Nakagawa K, Nozaki F, Sugawara H, Yamaguchi T. Antigenicity studies on sodium hyaluronate (SPH) Part 2: experiments in mouse and rabbit. JPN J Pharmacol Ther 1984;12:151-61.
|
| 45. | Goldberg RL, Toole BP. Hyaluronate inhibition of cell proliferation. Arthritis Rheum 1987;30:769-78.
|
| 46. | Sherman OH, Fox JM, Snyder SJ, Del Pizzo W, Friedman MJ, Ferkel RD, et al. Arthroscopy-"no-problem surgery". An analysis of complications in two thousand six hundred and forty cases. J Bone Joint Surg Am 1986;68:256-65.
|
| 47. | Yi T, Kim S, Kim J, Park J, Lee J. Comparison of blind technique and ultrasonography guided technique of intra-articular injection of the shoulder. J Korean Acad Rehab Med 2006;30:45-50.
|
| 48. | McFarland E, Kim T. Examination of the shoulder: The complete guide. New York, N.Y: Thieme Medical Publishers; 2006.
|
[Table 1], [Table 2], [Table 3]
| This article has been cited by | | 1 |
Adhesive capsulitis: One sonographic-guided injection of 20 mg triamcinolon into the rotator interval |
|
| Juel, N.G. and Oland, G. and Kvalheim, S. and Løve, T. and Ekeberg, O.M. | | Rheumatology International. 2013; 33(6): 1547-1553 | | [Pubmed] | | | 2 |
Evaluation of mulliganæs technique for adhesive capsulitis of the shoulder |
|
| Doner, G. and Guven, Z. and Atalay, A. and Celiker, R. | | Journal of Rehabilitation Medicine. 2013; 45(1): 87-91 | | [Pubmed] | | | 3 |
Adhesive capsulitis: one sonographic-guided injection of 20 mg triamcinolon into the rotator interval |
|
| Niels Gunnar Juel,Gunnar Oland,Synnøve Kvalheim,Tormod Løve,Ole Marius Ekeberg | | Rheumatology International. 2013; 33(6): 1547 | | [Pubmed] | [DOI] | | | 4 |
Intra-articular injection of hyaluronic acid for the reduction in joint adhesion formation in a rabbit model of knee injury |
|
| Min Wang,Chao Liu,Wei Xiao | | Knee Surgery, Sports Traumatology, Arthroscopy. 2013; | | [Pubmed] | [DOI] | | | 5 |
Addition of Intra-articular Hyaluronate Injection to Physical Therapy Program Produces No Extra Benefits in Patients With Adhesive Capsulitis of the Shoulder: A Randomized Controlled Trial |
|
| Lin-Fen Hsieh,Wei-Chun Hsu,Yi-Jia Lin,Hsiao-Lan Chang,Chiao-Chien Chen,Vincent Huang | | Archives of Physical Medicine and Rehabilitation. 2012; 93(6): 957 | | [Pubmed] | [DOI] | | | 6 |
Addition of intra-articular hyaluronate injection to physical therapy program produces no extra benefits in patients with adhesive capsulitis of the shoulder: A randomized controlled trial |
|
| Hsieh, L.-F. and Hsu, W.-C. and Lin, Y.-J. and Chang, H.-L. and Chen, C.-C. and Huang, V. | | Archives of Physical Medicine and Rehabilitation. 2012; 93(6): 957-964 | | [Pubmed] | | | 7 |
Magnetic resonance-guided interventions of large and small joints |
|
| Garmer, M. and Grönemeyer, D. | | Topics in Magnetic Resonance Imaging. 2011; 22(4): 153-169 | | [Pubmed] | | | 8 |
Magnetic Resonance–Guided Interventions of Large and Small Joints |
|
| Marietta Garmer,Dietrich Grönemeyer | | Topics in Magnetic Resonance Imaging. 2011; 22(4): 153 | | [Pubmed] | [DOI] | |
|
|
|


|
|
|
|
|