| |


 |
| Year : 2011 | Volume
: 5
| Issue : 2 | Page : 54-59 |
|
|
|
|
|
CASE REPORT Arthroscopic arthrodesis of the shoulder: Fourteen-year follow-up
Antonio Jiménez-Martín, Santiago Pérez-Hidalgo
Department of Orthopaedic Surgery, Hospital FREMAP Sevilla, Spain
Correspondence Address:
Antonio Jiménez-Martín
Hospital FREMAP Sevilla, Avda. de Jerez s/n. CP 41012., Sevilla 34-609012308
Spain
 Source of Support: None, Conflict of Interest: None  | 3 |
DOI: 10.4103/0973-6042.83199

|
|
|
|
| Date of Web Publication | 26-Jul-2011 |
 Abstract Abstract | | |
Shoulder arthrodesis is indicated in infections, brachial paralysis, irreparable rotator cuff tears, osteoarthritis without indication of prosthesis, rescue after arthroplasty, or after surgery for cancer. Arthroscopic arthrodesis is exceptional. Our aim is presenting our result after 14 years of follow-up of one patient. We present a case report of a 17-year-old male patient. He suffered fracture of left scapula (type V, Ideberg), fracture of left clavicle (type I, Craig), and fracture of left distal ulna. We realized osteosynthesis of clavicle (plate and screws) with the aim of treating this floating shoulder. Electromyography showed partial axonotmesis of axilar nerve. After 7 months of follow-up, axonotmesis was still present. We realized arthroscopic shoulder arthrodesis (three cannulated screws). Fourteen years later, shoulder movement was as follows: Flexion, 0-90°; maximum abduction, 40° with shoulder atrophy; Constant, 47 points; and UCLA, 17 points, without pain. Arthrodesis with screws reaches a subjective benefit in 82% of patients. Percentage of pseudarthrosis is less than in patients treated with plates, although the risks of infections, fractures, and material removal are greater than in patients treated with plates. Shoulder arthroscopic arthrodesis is exceptional, but it allows minimal surgical aggression.
Keywords: Arthrodesis, arthroscopy, shoulder
How to cite this article:
Jiménez-Martín A, Pérez-Hidalgo S. Arthroscopic arthrodesis of the shoulder: Fourteen-year follow-up. Int J Shoulder Surg 2011;5:54-9 |
| Introduction | |  |
Arthrodesis of the shoulder is a surgical procedure that is indicated in cases of infection, obstetrical brachial plexus palsy, [1] post-traumatic brachial plexus palsy, [2] massive unrepairable rotator cuff tears, combined paralysis and insufficiency of the rotator cuff and deltoid muscle, omarthrosis without indication for arthroplasty, salvage surgery after failed glenohumeral arthroplasty (with bone loss and muscular insufficiency of the rotator cuff and deltoid [3] ), recurrent shoulder dislocations, or stabilization after resection of a neoplastic lesion. [4]
Arthroscopic arthrodesis of the shoulder is a procedure that is only carried out in exceptional circumstances. [5],[6],[7] Our aim is to present the results in a patient who was operated on using this method with arthroscopic techniques, after 14-year follow-up.
| Case Report | | |
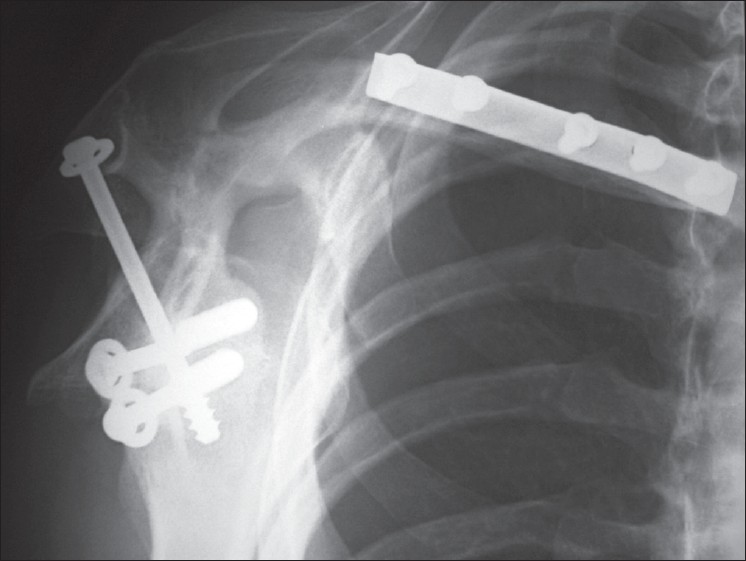
We present a case report of a 17-year-old male who suffered an accident in 1996, which caused cranioencephalic trauma, thoracic trauma with fracture of the left fourth rib, comminuted fracture of the left scapula (Ideberg type V, [Figure 1], [Figure 2] and [Figure 3]), fracture of the left clavicle (middle third, Craig type I), left acromioclavicular dislocation (Rockwood grade I), and fracture of the left distal cubitus, as well as multiple contusions. The patient reported loss of sensitivity and mobility in the left shoulder. Movements like abduction, anterior flexion, and rotations were impossible. An emergency operation was performed with open reduction and osteosynthesis using a plate and screws in order to stabilize the clavicle of this floating shoulder. An electromyography (EMG) was performed 2 months later, and motor affection of the axillary nerve was detected, with lengthened latency and reduced amplitude. Musculocutaneous nerve conduction was normal. In deltoid muscle, partial moderate-to-severe denervation was observed, whereas in supraspinatus muscle, there was no denervation. All of these results indicated left axillary neuropathy (partial axonotmesis). After 7 months of follow-up, axillary nerve still presented a low motor potential. There was an intermediate recruitment without denervation in supraspinatus muscle in repose, and there was a moderate denervation in deltoid muscle at rest, with simple recruitment. These aspects indicated that axonotmesis of the axillary nerve had persisted and it was becoming established.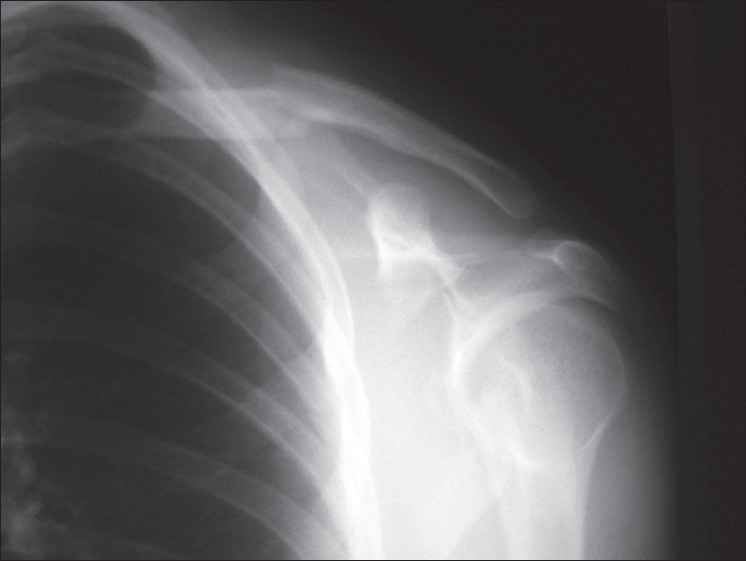 | Figure 1: Craig type I fracture of clavicle (middle third), fracture of scapula (probably Ideberg type V), floating shoulder
Click here to view |
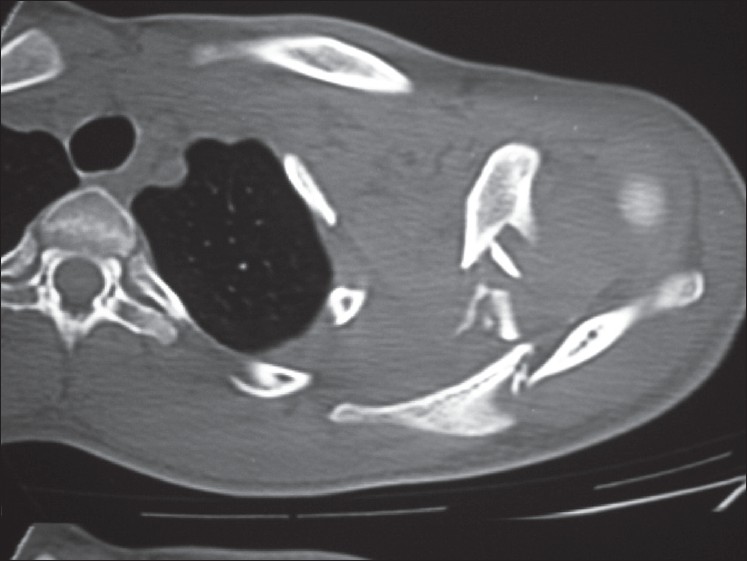 | Figure 2: CT image. Observe the high degree of comminution in the area of the scapula
Click here to view |
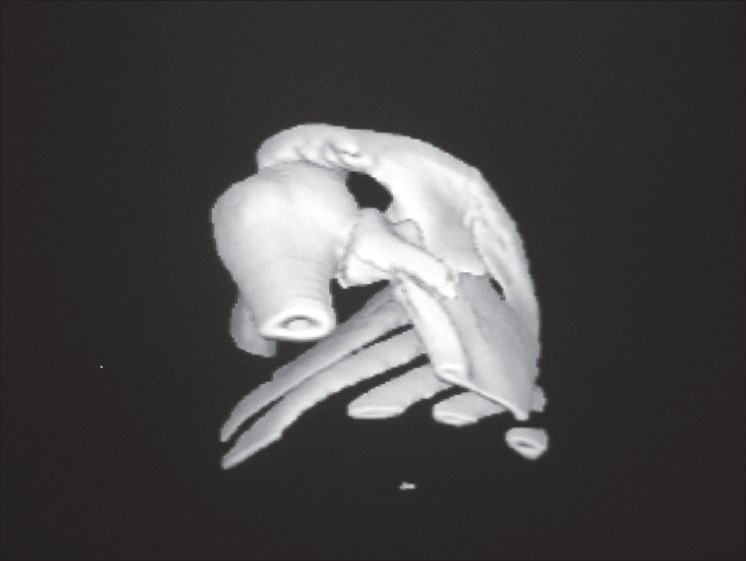 | Figure 3: Three-dimensional CT reconstruction. Original image from 1996. Comminuted fracture of scapula, probably Ideberg type V
Click here to view |
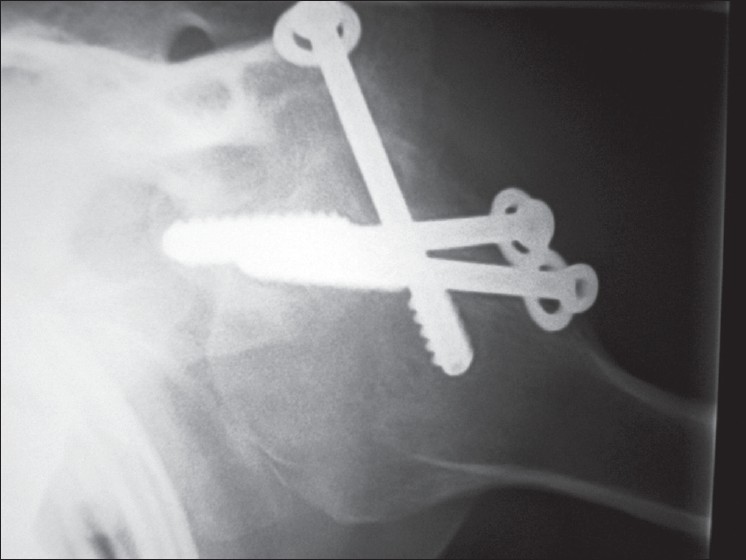
We considered the situation of the paralyzed shoulder, with omarthrosis, instability, and floating shoulder. Due to these findings, we decided that arthrodesis should be performed percutaneously with arthroscopic support, using three cannulated screws, under scopic control [Figure 4].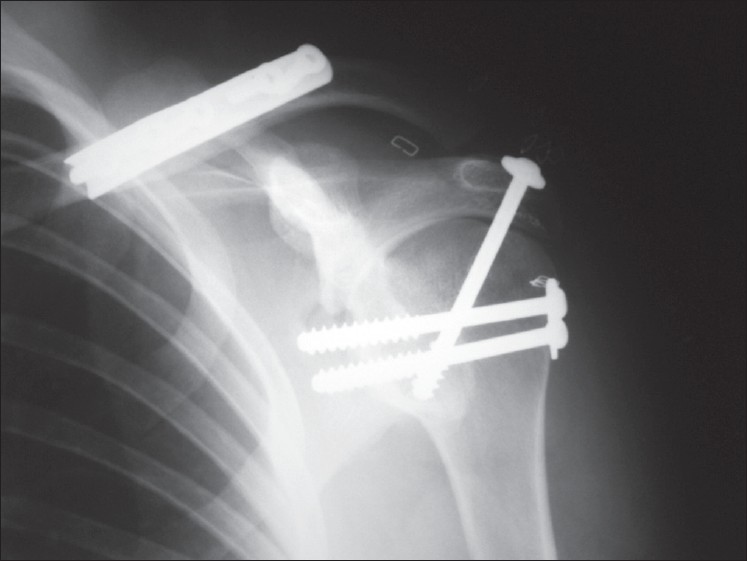 | Figure 4: Radiographic image of arthrodesis of the shoulder with three cannulated screws. Observe the staples which close arthroscopic portals, without requiring larger incisions. Glenohumeral and acromiohumeral stability is ascertained by the degree of compression that is achieved. Clavicle osteosynthesis is also noteworthy; this had been performed 7 months previously, using an osteosynthesis plate (1996)
Click here to view |
Surgical technique
Under general anesthesia, patient was placed in beach chair position, with circumferential accessibility to the left shoulder, and the operative arm was draped free.
The arthroscope was placed through a standard posterior arthroscopic portal and an arthroscopic cannula anteriorly. The shoulder was held in a position of 30° of flexion, 30° of abduction, and 30° of internal rotation, while a radius bur was used to denude the articular surfaces of both the humeral head and glenoid to bleeding subchondral bone.
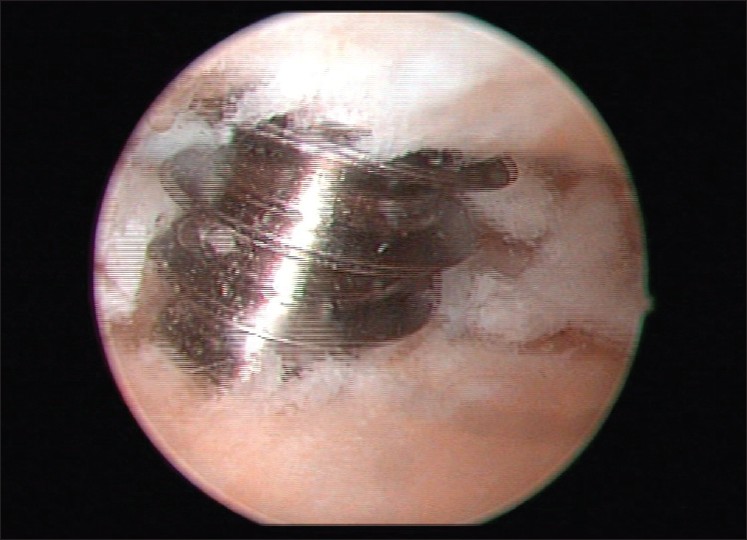
An anterior cruciate ligament guide was used to direct percutaneous placement of two guidewires through the proximal humerus from lateral to medial and into the joint under direct arthroscopic visualization. Both guidewires were driven through the center of the glenoid, where they were then measured and reamed for placement of 6.5-mm cannulated cancellous screws. With the arm held in the appropriate position, sequential tightening of the screws achieved adequate compression of the glenohumeral surfaces. The positions of the two glenohumeral screws were verified with biplanar fluoroscopy before a third 6.5-mm cannulated cancellous screw was placed from the lateral edge of the acromion into the humeral head inferiorly toward the shaft-glenoid. The acromiohumeral screw position was verified with biplanar fluoroscopy. Finally, we did not need bone graft, because we achieved total compression into the glenohumeral joint before incisions were closed. An abduction pillow was placed under the operative arm, holding it in the appropriate position, and kept in place for 3 months. Rehabilitation consisted of passive assisted exercises and progressed to active assisted exercises after 4 weeks [Figure 5], [Figure 6] and [Figure 7]. | Figure 6: After we denuded articular surfaces of both humeral head and glenoid to bleeding subchondral bone, we used two guidewires through the proximal humerus from lateral to medial and into the joint under direct arthroscopic visualization. We can see one of them. Both guidewires were driven through the center of the glenoid
Click here to view |
 | Figure 7: See initial placement of one 6.5-mm cannulated cancellous screw
Click here to view |
Pearls and pitfalls
Arthroscopic shoulder orientation, a good level of experience in glenolabral arthroscopic surgery, and management of anterior cruciate ligament guides are very important points in this procedure. We think these points are essential in this procedure. One typical pitfall is tightening of screws without previous correct arthroscopic control or loosening of guide position before tightening cannulated cancellous screws. Another interesting point is that threads of the screws must engage across the joint into the glenoid to ensure solid bone compression.
Advantages over open techniques
We consider that this arthroscopic technique is better than the open one, because it is a less-invasive procedure. With two arthroscopic portals and percutaneous cancellous screws, we can achieve similar results, without problems like intolerance of the material, due to protrusion at the side of the acromion with posterior removal, risk of infection, and risk of fractures of the humerus after surgery with plates.
Follow up
Clinical evolution developed favorably, since surgery pain disappeared, and the arm became functional for everyday activities.
At this moment, 14 years later, this patient is still working with the same paralysis, in a workplace that has been adapted to his pathology. He presents movement arc of 0-90° for anterior flexion, maximum abduction of 20°, and atrophy of the deltoid, supraspinatus, and infraspinatus. We have measured 47 points on Constant's test and 17 points on the UCLA scale. Although these are poor results, he denies any pain. We tried to achieve radiographic arthrodesis, but finally, we could see a gap between the bone of the glenoid and the humeral head, with no secondary displacement, infectious complications, or intolerance of material, and patient is satisfied with results of this surgery [Figure 8] and [Figure 9]. We consider that it is very important fact that the threads of the screws cross the joint, in order to achieve solid compression of the bone. We only had these screws several years ago, with a long area of threads. This design and its position perhaps precluded to fibrous union. We think we have to warn the readers to ensure that the threads of the screws engage across the joint into the glenoid to ensure solid bone compression. With this warning, a better technical and radiological result could have been achieved.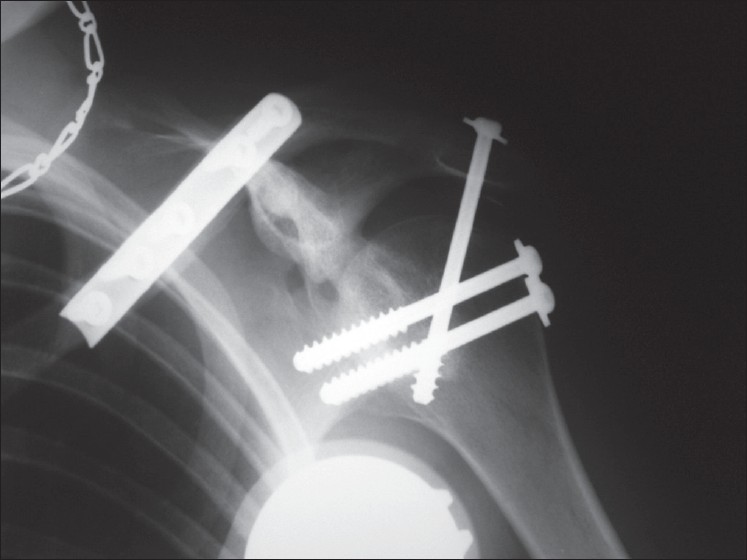 | Figure 8: Fourteen years later, we think that structure stability is present, although with gap between the bone of the glenoid and the humeral head, glenohumeral fibrous union, and no secondary displacement
Click here to view |
 | Figure 9: At present, movement arc is 0-90°anterior flexion, maximum abduction of 20°, with atrophy of the deltoid, supraspinatus, and infraspinatus muscles. 47 points on the constant scale and 17 points on the UCLA scale
Click here to view |
Recently, in the last revision, after 14 years and 8 months of follow-up, patient suffered a trauma on the affected shoulder, with minimal pain. However, movement arc did not change: 0-90° for anterior flexion, maximum abduction of 40°, and atrophy of the deltoid, with the same result in Constant's and UCLA scales. We only have seen one broken screw, and fibrous union is reached on the x-ray study. Patient is very satisfied with evolution [Figure 10], [Figure 11], [Figure 12], [Figure 13] and [Figure 14].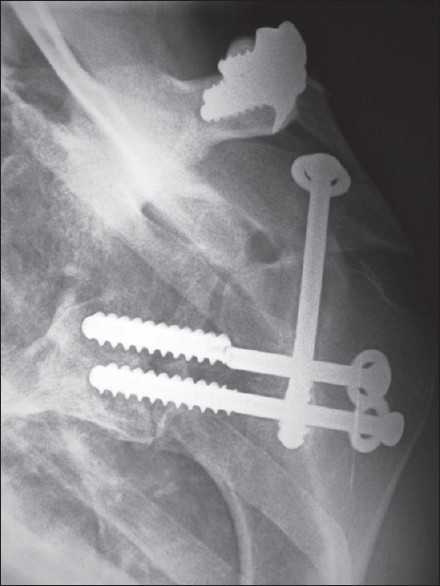 | Figure 10: X-ray. After a new trauma, one screw seems to be broken. However, fibrous union with no secondary displacement can be seen
Click here to view |
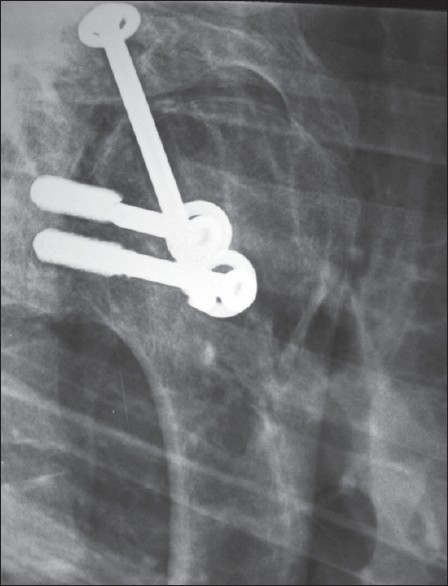 | Figure 11: X-ray. Another actual projection. Transthoracic view. Glenohumeral fibrous union
Click here to view |
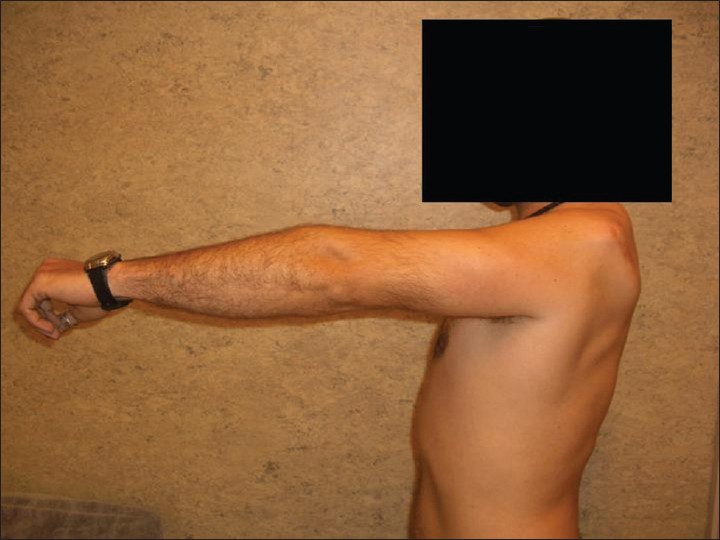 | Figure 14: Fourteen years and 8 months later. We can observe the same movement arc from 1 year ago. Although one screw broke, anterior flexion was until 90°. We can observe deltoid atrophy
Click here to view |
| Discussion | | |
Among the procedures that have been described for arthrodesis of the shoulder, various alternatives have been suggested. Osteosynthesis using 1 or 2 plates is a priori the most solid system, although it has the drawback that material has to be withdrawn, which involves risk of infection and skin necrosis. [4] Pelvic reconstruction plates [4],[8] and Locking Compression Plates (LCP) have been proposed. They are easier to adapt to this type of surgical procedure, as described by Richards et al. [9] Klonz et al.[10] suggest that the use of plates under the acromion offers advantages. This place avoids the problem of intolerance of the material, because it decreases protrusion at the side of the acromion when screws are inserted. There is also a high degree of compression, and physiotherapy can be started at an early stage.
On the other hand, arthrodesis with cancellous bone screws offers the most effective system, with a subjective improvement reported by patients in 82% of cases, when three screws are used: two glenohumeral screws and one acromiohumeral screw. [11]
Rühmann et al.[4] compared systems based on plates and screws, and observed that although the degree of pseudoarthrosis appeared to be less severe when plates were used, there was a greater risk of infection, there were more fractures of the humerus after surgery, and material needed to be removed more often than when screws were used. Arthrodesis performed with screws offered more benefits, because it required less-invasive surgery, even though the patient had to be immobilized for longer time than when plates were used.
Finally, external fixation is another possibility. However, it has certain complications, such as loosening of the pins, infection of their route, or fracture at the insertion points. This procedure should be reserved for cases of open fracture. [12]
Arthroscopic arthrodesis with screws has only been described in a few cases, [5],[6],[7] although it is a procedure that allows complete visualization of joint surface so that accurate acromiohumeral and glenohumeral decortication can be performed, [13] with a minimum degree of surgical aggressiveness. It has also been described in exceptional cases of instability of the shoulder. [6] We think we have to warn the readers to ensure that the threads of the screws engage across the joint into the glenoid to ensure solid bone compression, in order to achieve a better technical and radiological result.
To obtain an optimum functional result in arthrodesis, trapezius, levator scapulae, serratus anterior, and rhomboid muscles must be able to function properly. [13] Moreover, according to Safran and Iannotti, the use of a vascularized autologous graft from the iliac crest or fibula improves the rates of consolidation in such procedures. [14]
Arthrodesis position has been described by Nagy et al.[15] Shoulder is placed at 15-30° flexion, 35-45° abduction, and 30-40° internal rotation. Safran and Iannotti [14] recommend another position of 20° of anterior flexion, 20° of abduction, and 40° of internal rotation.
The most frequent complications of shoulder arthrodesis are pseudoarthrosis (4-12% or 5-20% [16] ), humerus fractures (10-15%, 50% of which are in patients with brachial plexus palsy [1] ), pain (25% or 30% [9] ), infection (3-5% [16] ), skin necrosis, and acromioclavicular arthrosis.
| Conclusion | | |
We consider that arthroscopic shoulder arthrodesis should be the procedure of choice in post-traumatic omarthrosis where there is injury of brachial plexus, because clinical results are favorable and there are few complications. Threads of the screws must engage across the joint into the glenoid to ensure solid bone compression, in order to achieve solid bone compression and no fibrous union.
| References | | |
| 1. | Richards RR, Waddell JP, Hudson AR. Shoulder arthrodesis for the treatment of brachial plexus palsy. Clin Orthop Relat Res1985;198:250-8. 
|
| 2. | Chammas M, Goubier JN, Coulet B, Reckendorf GM, Picot MC, Allieu Y. Glenohumeral arthrodesis in upper and total brachial plexus palsy. A comparison of functional results. J Bone Joint Surg Br 2004;86:692-5.
|
| 3. | Scalise JJ, Iannotti JP. Glenohumeral arthrodesis after failed prosthetic shoulder arthroplasty. Surgical technique. J Bone Joint Surg Am 2009;91:30-7.
|
| 4. | Rühmann O, Schmolke S, Bohnsack M, Flamme C, Wirth CJ. Shoulder arthrodesis: Indications, technique, results, and complications. J Shoulder Elbow Surg 2005;14:38-50.
|
| 5. | Syal A, MacDonald P. Arthroscopic arthrodesis of the shoulder: A report of two cases. J Shoulder Elbow Surg 2008;17:e23-5.
|
| 6. | Hiersemann K, Patsalis T, Saxler G. Arthroscopy-assisted glenohumeral arthrodesis: A case of uncontrollable shoulder instability. Unfallchirurg 2007;110:456-9.
|
| 7. | Morgan CD, Casscells CD. Arthroscopic-assisted glenohumeral arthrodesis. Arthroscopy 1992;8:262-6.
|
| 8. | Chun JM, Byeon HK. Shoulder arthrodesis with a reconstruction plate. Int Orthop 2009;33:1025-30 .
|
| 9. | Richards RR, Sherman RM, Hudson AR, Waddell JP. Shoulder arthrodesis using a pelvic-reconstruction plate. A report of eleven cases. J Bone Joint Surg Am 1988;70:416-21.
|
| 10. | Klonz A, Habermeyer P. Arthrodesis of the shoulder. A new and soft-tissue-sparing technique with a deep locking plate in the supraspinatus fossa. Unfallchirurg 2007;110:891-5.
|
| 11. | Cofield RH, Briggs BT. Glenohumeral arthrodesis. Operative and long-term functional results. J Bone Joint Surg Am 1979;61:668-77.
|
| 12. | Johnson CA, Healy WL, Brooker AF Jr, Krackow KA. External fixation shoulder arthrodesis. Clin Orthop Relat Res 1986;211:219-23.
|
| 13. | Clare DJ, Wirth MA, Groh GI, Rockwood CA Jr. Shoulder arthrodesis. J Bone Joint Surg Am 2001;83-A:593-600.
|
| 14. | Safran O, Iannotti JP. Arthrodesis of the shoulder. J Am Acad Orthop Surg 2006;14:145-53.
|
| 15. | Nagy L, Koch PP, Gerber C. Functional analysis of shoulder arthrodesis. J Shoulder Elbow Surg 2004;13:386-95.
|
| 16. | González-Díaz R, Rodríguez-Merchán EC, Gilbert MS. The role of shoulder fusion in the era of arthroplasty. Int Orthop 1997;21:204-9.
|
[Figure 1], [Figure 2], [Figure 3], [Figure 4], [Figure 5], [Figure 6], [Figure 7], [Figure 8], [Figure 9], [Figure 10], [Figure 11], [Figure 12], [Figure 13], [Figure 14]
| This article has been cited by | | 1 |
Arthroscopically Assisted Shoulder Arthrodesis: Is It an Effective Technique? |
|
| Giuseppe Porcellini,Felix H. Savoie,Fabrizio Campi,Giovanni Merolla,Paolo Paladini | | Arthroscopy: The Journal of Arthroscopic & Related Surgery. 2014; | | [Pubmed] | [DOI] | | | 2 |
Arthroscopic Glenohumeral Arthrodesis With O-Arm Navigation |
|
| Alexandre Lädermann,Patrick J. Denard | | Arthroscopy Techniques. 2014; | | [Pubmed] | [DOI] | |
|
|
|
|