| |


 |
| Year : 2011 | Volume
: 5
| Issue : 2 | Page : 50-53 |
|
|
|
|
|
CASE REPORT Isolated avulsion fracture of lesser tuberosity of the humerus: Review of the literature and report of two cases
Bilgehan Tosun, Cumhur Cevdet Kesemenli
Department of Orthopaedics and Traumatology, Kocaeli University, School of Medicine, Kocaeli, Turkey
Correspondence Address:
Bilgehan Tosun
Kocaeli University School of Medicine, Department of Orthopaedics and Traumatology, Umuttepe Merkez Kampüsü, 41380 Umuttepe, Kocaeli
Turkey
 Source of Support: None, Conflict of Interest: None
DOI: 10.4103/0973-6042.83198

|
|
|
|
| Date of Web Publication | 26-Jul-2011 |
 Abstract Abstract | | |
Two cases of acute isolated avulsion fracture of the lesser tuberosity of the humerus and their short-term outcome are presented with a review of previously reported cases. Open reduction and internal fixation was performed. Outcomes were excellent, and the patients regained their normal pain-free shoulder function 3 months after the operation. This was a Level IV study.
Keywords: Fracture, shoulder, tuberculum, tuberosity
How to cite this article:
Tosun B, Kesemenli CC. Isolated avulsion fracture of lesser tuberosity of the humerus: Review of the literature and report of two cases. Int J Shoulder Surg 2011;5:50-3 |
| Introduction | |  |
Isolated avulsion fracture of the lesser tuberosity is an unusual phenomenon that usually occurs in association with fractures involving two or three segments of proximal humerus or as a part of a posterior fracture dislocation. [1],[2],[3] The typical mechanism of injury is an abduction external rotation trauma to shoulder. [2],[4],[5] The subscapularis muscle forcefully contracts to resist, leading to an avulsion of the lesser tuberosity.
The purpose of this paper is to review the current literature and present our two cases of acute avulsion of the lesser tuberosity treated with surgical reduction and fixation.
| Case Reports | | |
Case 1
A 19-year-old boy presented to our institution with right shoulder pain after a traffic crash. On clinical examination, the patient had crepitus and tenderness by palpation over the anterior aspect of the proximal humerus and pain on all active and passive movements. On further examination, no associated visceral or neurovascular injury of the involved limb was detected. Fracture of the lesser tuberosity could not be determined with certainty on the anteroposterior [Figure 1]. Thus the patient underwent a computed tomography examination. Fractured lesser tuberosity was found to be displaced just caudal to the glenoid, and there was a defect on the humeral head [Figure 2]. 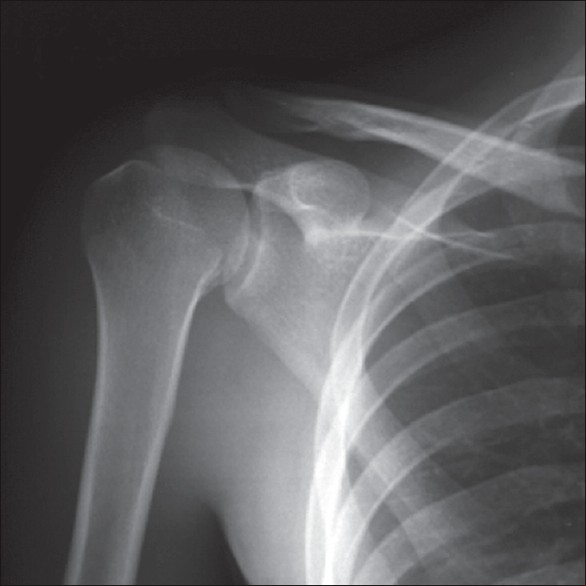 | Figure 1: Anteroposterior radiograph of the shoulder evokes suspicion of a fracture of the lesser tuberosity
Click here to view |
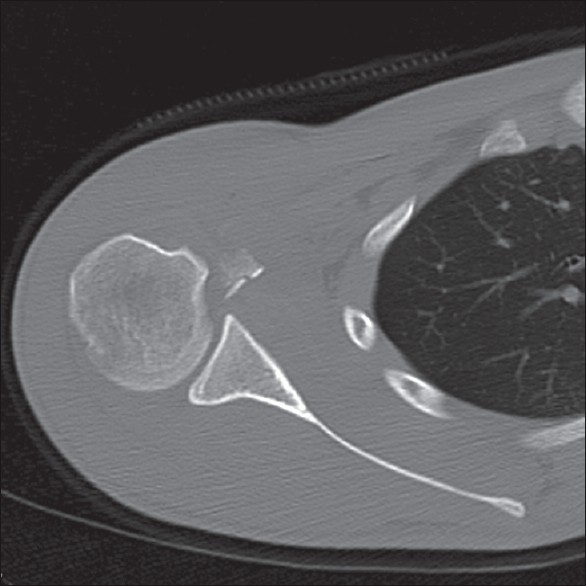 | Figure 2: Preoperative CT. Axial view shows the fractured lesser tuberosity and a defect on the humeral head
Click here to view |
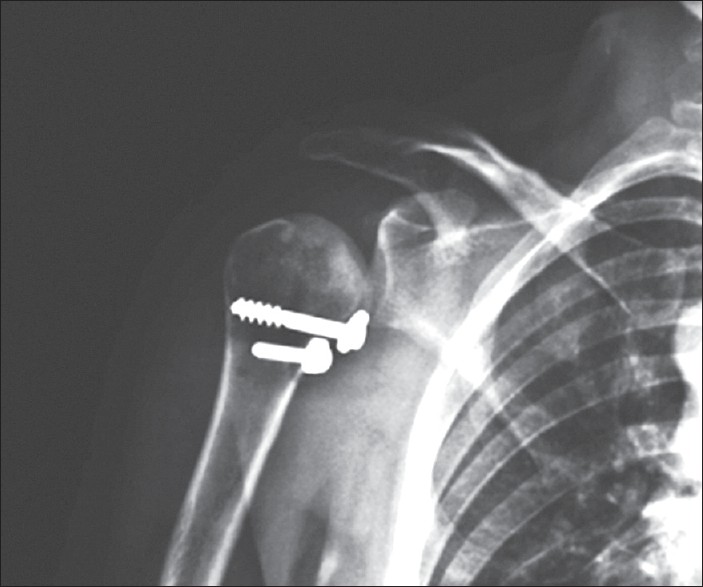
Through a small axilla-based deltopectoral incision, fractured lesser tuberosity was exposed and reattached to its original location. The interval was closed in a standard manner after the fixation of the fragment with two headless fully threaded bone screws [Figure 3]. | Figure 3: Anteroposterior radiograph after the fixation of the lesser tuberosity with two headless fully threaded bone screws
Click here to view |
Case 2
A 33-year-old, 13-week-pregnant woman was referred to our Emergency Department with a history of fall after epileptic attack 3 days ago. She could not recall what the position of her arm was at the time of injury. Physical examination was remarkable for edema and tenderness to palpation over the anterior proximal humerus with restricted joint rotation. A sound of clunk was notable during internal rotation.
Due to the pregnancy, only an anteroposterior radiograph was taken. Proper shields (lead apron) were used to protect the fetus from X-ray beams. On the radiograph, a fracture of the base of the lesser tuberosity was demonstrated [Figure 4]. 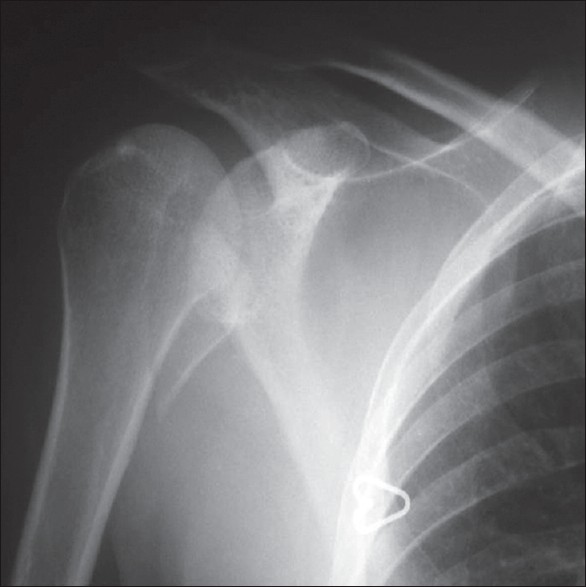 | Figure 4: Anteroposterior radiograph showing an isolated lesser tuberosity fracture
Click here to view |
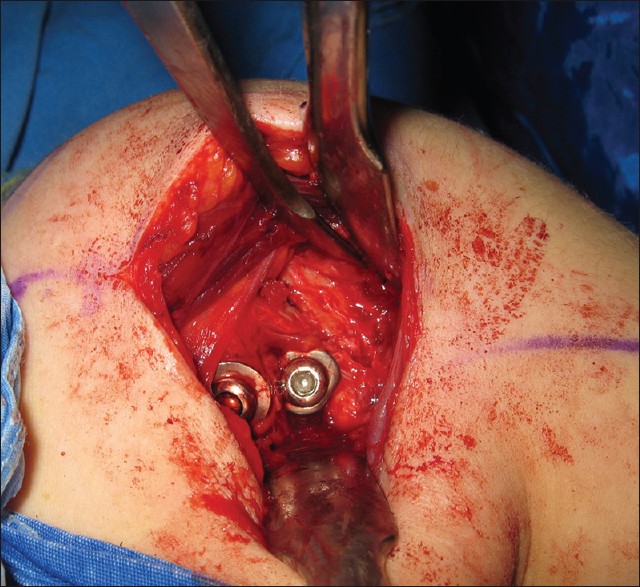
A deltopectoral approach was performed through a small axilla-based incision. The lesser tuberosity was seen to be displaced from its anatomical position to the medial aspect of the surgical neck of the humerus [Figure 5]. The subscapularis tendon was found inserted on the posterior portion of the fragment. The fragment was elevated and restored to its anatomical location [Figure 6]. To secure the tuberosity in its original anatomical position, 6.5-mm cancellous and 4.5-mm cortical bone screws were used [Figure 7], and the interval was repaired in a side-to-side fashion with the use of 2-0 nonabsorbable sutures. 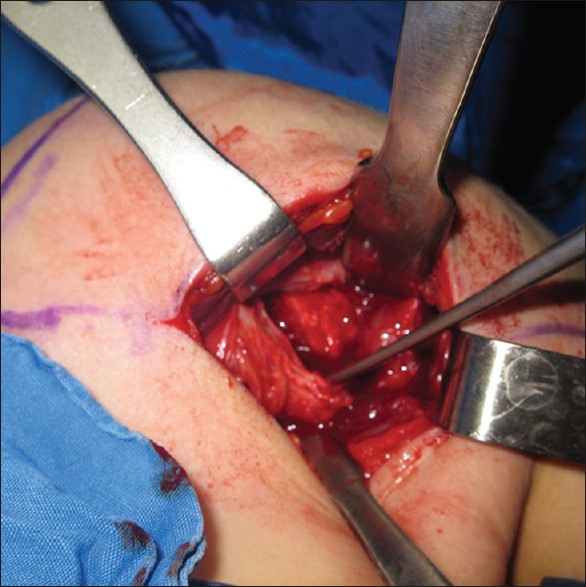 | Figure 5: Intraoperative view of the fractured lesser tuberosity. Fragment is elevated
Click here to view |
 | Figure 7: Postoperative anteroposterior radiograph shows the reduction of the fragment to its anatomical location
Click here to view |
Both the patients underwent the same rehabilitation program. The shoulders were supported in a sling for 2 weeks. Then a program of passive assisted range-of-motion exercises in forward flexion, external rotation, extension and internal rotation was started. Patients progressed to an active range-of-motion program in the fourth week postoperatively. At the end of the sixth week postoperatively, resistive exercises were added. On the follow-up 3 months after the operation, both the patients were found to have regained their normal shoulder functions. Two years after surgery, our patients had full pain-free active range-of-motion.
| Discussion | | |
An isolated avulsion fracture of the lesser tuberosity is an uncommon injury. [3],[6],[7],[8],[9] Far less experience exists in the management of this rare injury. Clinical series remain small or are limited to case reports.
The lesser tuberosity is protected from direct injury by its small size and its location on the medial side of the head of the humerus. Therefore, most of the authors believe the main mechanism of injury is muscular violence. [3]
When the subscapularis muscle forcefully contracts to resist abduction and external rotation of the shoulder, it is forced to extend, and the resultant strong traction force thus avulses the lesser tuberosity. [3] However, less likely mechanisms are also described in the literature.
A sudden involuntary contraction of the subscapularis muscle during sleep may result in fracture. Such fractures have been described to occur during electroconvulsive therapy for psychiatric disorders. [5] Involuntary contraction of the subscapularis muscle might have been the cause of lesser tuberosity fracture in our epileptic patient.
Symptoms specific to acute cases include an exacerbation of pain on external rotation, restricted internal rotation and tenderness on the lesser tuberosity. [3],[10]
On plain radiographs, these fractures may be misdiagnosed as calcific tendonitis of the rotator cuff or osseous Bankart lesions. [2],[11] An anteroposterior view in maximal internal rotation projects the lesser tuberosity in profile and may be helpful in diagnosis. Large displaced fractures can be easily seen on standard anteroposterior radiographs, but the axillary view is often necessary to detect smaller fragments with minimal displacement. [4],[11],[12],[13] An axillary view demonstrates the fragment most clearly and is essential to prevent overlooking such an injury. Axillary views of the shoulders were not taken in our 2 patients. Because of the quite small fragment, we could not diagnose the fracture initially in case 1 with an anteroposterior view. Diagnosis was made with the use of CT examination. Due to pregnancy, only an anteroposterior view was taken in case 2. Fortunately, the fragment was large and thus easily diagnosed without any other diagnostic tools.
There is a possibility of dislocating the biceps tendon if the most superior part of the lesser tuberosity also suffers from a fracture. [12] Medial dislocation of the biceps tendon has been found by Paschal to be associated with disruption of the coracohumeral ligament. [14] While the bicipital groove was not influenced by the fracture, we did not see the biceps tendon dislocation.
Most of the acute cases that have been reported in the literature were treated by open reduction and internal fixation, resulting in consistently excellent clinical outcomes [Table 1]. For acute nondisplaced fractures of the lesser tuberosity, nonoperative management can provide satisfactory results. Operative treatment is recommended in patients with displacement greater than 5 mm or 45° of angulation, blockage to motion, significant clinical weakness, or continued pain. [1] 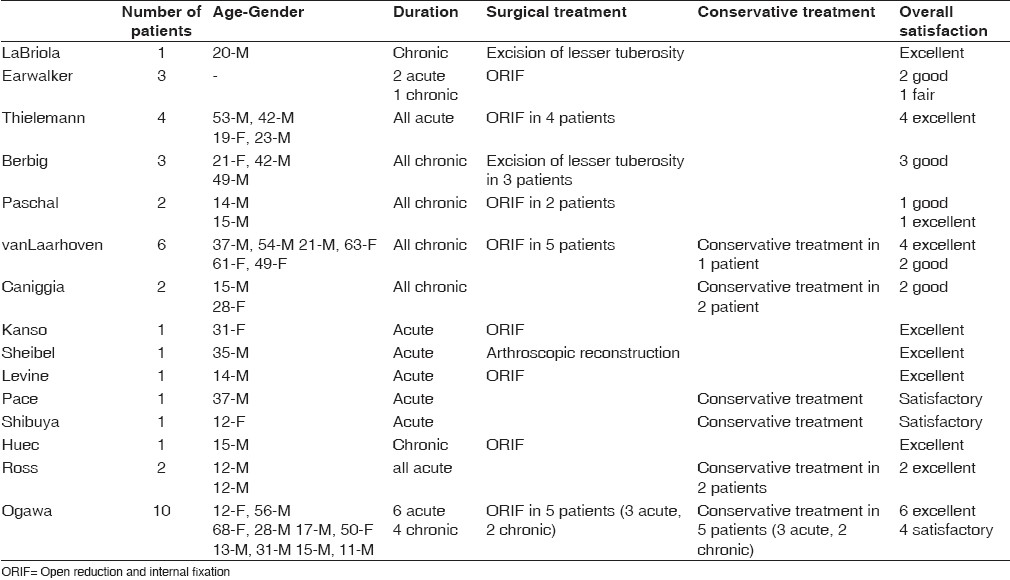 | Table 1: Data and characteristics of the patients that have been reported about the topic in the literature
Click here to view |
Open [1],[3],[10],[14] or arthroscopy-assisted reduction [12] and fixation; and excision of the lesser tuberosity [8],[15] are available treatment modalities that may lead to excellent clinical and radiological results.
Although it is not possible to compare the outcomes of surgical and conservative treatments with those of our two cases, open reduction and fixation of the lesser tuberosity resulted in excellent outcome in our patients.
| Conclusion | | |
A successful functional outcome following isolated lesser tuberosity fractures requires a proper indication, good surgical technique, appropriate postoperative therapy and patient compliance. Open reduction and fixation may be the treatment of choice for acute cases; however, in chronic cases, nonoperative treatment should be administered before surgical intervention.
| References | | |
| 1. | Levine B, Pereira D, Rosen J. Avulsion fractures of the lesser tuberosity of the humerus in adolescents: Review of the literature and case report. J Orthop Trauma 2005;19:349-52. 
|
| 2. | van Laarhoven HA, te Slaa RL, van Laarhoven EW. Isolated avulsion fracture of the lessr tuberosity of the humerus. J Trauma 1995;39:997-9.
|
| 3. | Ogawa K, Takahashi M. Long-term outcome of isolated lesser tuberosity fractures of the humerus. J Trauma 1997;42:955-9.
|
| 4. | Ross GJ, Love MB. Isolated avulsion fracture of the lesser tuberosity of the humerus: Report of two cases. Radiology 1989;172:833-4.
|
| 5. | Pace A, Ribbans W, Kim JH. Isolated lesser tuberosity fracture of the humerus. Orthopedics 2008;31:94.
|
| 6. | Kanso I, Bricout JM. Isolated avulsion fracture of the lesser tuberosity of the humerus. Apropos of a case. Rev Chir Orthop Reparatrice Appar Mot 1998;84:554-7.
|
| 7. | Caniggia M, Maniscalco P, Picinotti A. Isolated avulsion fracture of the lesser tuberosity of the humerus. Report of two cases. Panminerva Med 1996;38:56-60.
|
| 8. | Berbig R, Keller H, Metzger U. Isolated fracture of the lesser tuberosity of the humerus: Case reports and review of the literature. Z Unfallchir Versicherungsmed 1994;87:159-68.
|
| 9. | Thielemann FW, Kley U, Holz U. Isolated injury of the subscapular muscle tendon. Sportverletz Sportschaden 1992;6:26-8.
|
| 10. | Le Huec JC, Schaeverbeke T, Moinard M, Kind M, Chauveaux D, Le Rebeller A. Isolated avulsion fracture of the lesser tubercle of the humerus in children.Acta Orthop Belg 1994;60:427-29.
|
| 11. | Earwaker J. Isolated avulsion fracture of the lesser tuberosity of the humerus. Skeletal Radiol 1990;19:121-5.
|
| 12. | Scheibel M, Martinek V, Imhoff AB. Arthroscopic reconstruction of an isolated avulsion fracture of the lesser tuberosity. Arthroscopy 2005;21:487-94.
|
| 13. | Shibuya S, Ogawa K. Isolated avulsion fracture of the lesser tuberosity of the humerus. A case report. Clin Orthop Relat Res 1986;211:215-8.
|
| 14. | Paschal SO, Hutton KS, Weatherall PT. Isolated avulsion fracture of the lesser tuberosity of the humerus in adolescents. A report of two cases. J Bone Joint Surg Am 1995;77:1427-30.
|
| 15. | LaBriola JH, Mohaghegh HA. Isolated avulsion fracture of the lesser tuberosity of the humerus. A case report and review of the literature. J Bone Joint Surg Am 1975;57:1011.
|
[Figure 1], [Figure 2], [Figure 3], [Figure 4], [Figure 5], [Figure 6], [Figure 7]
[Table 1]
| This article has been cited by | | 1 |
Frattura traumatica di trochine in paziente in postumi di stabilizzazione della spalla con tecnica letarjet: a case report |
|
| G. M. Calori,M. Colombo,E. Mazza,M. Bucci,P. Fadigati,E. Malagoli,S. Mazzola,R. Leo | | Aggiornamenti CIO. 2013; 19(1): 33 | | [Pubmed] | [DOI] | |
|
|
|
|