| |


 |
| Year : 2012 | Volume
: 6
| Issue : 1 | Page : 15-18 |
|
|
|
|
|
ORIGINAL ARTICLE Partial-thickness articular surface rotator cuff tears in patients over the age of 35: Etiology and intra-articular associations
Chetan S Modi1, Christopher D Smith2, Stephen J Drew1
1 Department of Trauma and Orthopaedic Surgery, Upper Limb Unit, University Hospitals Coventry and Warwickshire NHS Trust, Coventry, CV2 2DX, United Kingdom
2 Department of Trauma and Orthopaedic Surgery, Upper Limb Unit, University Hospitals Coventry and Warwickshire NHS Trust, Coventry, CV2 2DX; University of Warwick Faculty of Medicine, Coventry, CV4 7AL, United Kingdom
Correspondence Address:
Chetan S Modi
University Hospitals Coventry and Warwickshire NHS Trust, Clifford Bridge Road, Coventry CV2 2DX
United Kingdom
 Source of Support: None, Conflict of Interest: None  | 2 |
DOI: 10.4103/0973-6042.94309

|
|
|
|
| Date of Web Publication | 26-Mar-2012 |
 Abstract Abstract | | |
Purpose: Partial-thickness articular-sided rotator cuff tears have a multifactorial etiology and are associated with degeneration of the tendon. They are often described as an injury of the young athlete, although they are also found in the older population. The aim of this study was to investigate the frequency and associations of partial-thickness articular-sided tears in patients over the age of 35 years.
Design: Retrospective
Materials and Methods: A retrospective study of all arthroscopic procedures for rotator cuff pathology in patients over the age of 35 years over a 2-year period by a single surgeon was performed. The included patients were divided into two groups based on the arthroscopic findings: those with a partial-thickness articular-sided rotator cuff tear and those with pure tendinopathy. The groups were then compared to identify the associated pathology with the rotator cuff lesions. 2×2 contingency table analysis and unpaired Student's t-test were used for statistical analysis.
Results: One hundred patients were included in the study of whom 62 had a partial articular-sided tear. Those with a partial articular-sided tear were older (P=0.0001), were more commonly associated with a documented injury (P=0.03), and more commonly had biceps degeneration (P=0.001) and synovitis (P=0.02) within the joint.
Conclusion: Partial-thickness articular-sided tears are a common occurrence in patients requiring arthroscopic surgery for rotator cuff pathology over the age of 35 years. This probably reflects an injury in an already degenerate cuff. This would support the theory of intrinsic degeneration of the tendon in this age group and probably represent a different etiology to those seen in the young athletes.
Level of Evidence: Level 3
Keywords: Associated pathology, etiology, partial-thickness, rotator cuff tears
How to cite this article:
Modi CS, Smith CD, Drew SJ. Partial-thickness articular surface rotator cuff tears in patients over the age of 35: Etiology and intra-articular associations. Int J Shoulder Surg 2012;6:15-8 |
| Introduction | |  |
The incidence of partial-thickness rotator cuff tears documented by magnetic resonance imaging (MRI) or ultrasound is approximately 8% in symptomatic patients and 16% in asymptomatic patients, with a mean age of 45-55 years. [1] Ultrasound and MRI, however, have been shown to have poor sensitivity for the detection of partial-thickness tears [2],[3],[4] and the incidence has been reported to be higher in cadaveric studies at 19-32%. [1],[5] Partial-thickness articular surface rotator cuff tears (PTASRCTs) are at least twice as common as bursal-sided tears [6],[7] and usually involve the supraspinatus tendon. [7,8] They have been described in the literature as an injury of the young athlete with a traumatic mechanism [9],[10] and are thought to be due to internal impingement of the under surface of the supraspinatus against the glenoid within the athletic population. [11],[12]
For the population as a whole, there is a debate about the etiology of partial-thickness rotator cuff tears. The extrinsic theory relies on an abnormal acromion causing external abrasion and damage to the bursal side of the cuff. [13],[14] The intrinsic theory hypothesises that degeneration occurs within the tendon. Histological tendon degeneration has been demonstrated more commonly on the articular side in cadaveric specimens [15] and this side of the rotator cuff is known to have a half the ultimate stress to failure compared to the bursal side. [16] Furthermore, histological changes to the under surface of the acromion have been associated with bursal-sided tears but not seen in association with articular-sided tears. [17] Clinical studies, however, have also shown that external impingement due to coracoacromial arch narrowing can lead to partial tears on the articular and bursal side of the rotator cuff. [18]
Symptomatic partial tears have been demonstrated to progress to full-thickness tears both with non-operative treatment [19] and with surgical interventions. [20],[21] Therefore, an understanding of their pathology is crucial. The aim of this study was to document the frequency of PTASRCTs in patients with rotator cuff pathology, analyze the association with other abnormalities within the joint, and document the association with injury in patients aged over 35 years.
| Materials and Methods | | |
A retrospective review of operation notes was performed for all arthroscopic procedures related to the rotator cuff (rotator cuff repair and subacromial decompression) in patients over the age of 35 years, performed over a 2-year period by a single surgeon. Patients having isolated rotator cuff pathology with/without concomitant acromioclavicular joint (ACJ) pathology were identified. Patients with full-thickness rotator cuff tears were excluded. All patients included in the study had completed a minimum 6-month period of non-operative treatment including physiotherapy and injections. Preoperative range of motion for these patients was mean forward flexion 142° (range 115°-165°), mean abduction 130° (range 95°-160°), and mean external rotation 32° (range 25°-50°). All patients had clinical signs of impingement (+ve Hawkins test [22] and +ve Neer test with local anesthetic injection [14] and a clinically intact cuff) and had radiological evidence of tendiopathy or a partial-thickness tear (MRI or ultrasound) with plain X-rays to assess gleno-humeral and acromial morphology.
The patients were subsequently divided into two groups based on the arthroscopic findings: those with a PTASRCT and those with pure tendinopathy. The PTASRCT group was subdivided into those with a tear greater than 50% and those with a tear less than 50% thickness.
Arthroscopy was performed by the senior author in the beach chair position using a standardized technique. After establishing a posterior, lateral, and anterior portal, an assessment of the joint and bursa was performed, similar to the 15-point examination described by Snyder. [23] This included the introduction of a 4-mm arthroscopic probe through the anterior portal to probe the labrum, articular surfaces, and rotator cuff insertion within the joint. During bursectomy, the probe would also be used to assess the under surface of the acromion and the bursal side of the rotator cuff. This would allow documentation of any associated lesions found. The condition of the articular surfaces was classified according to Outerbridge, [24] any synovitis was noted, and damage to the labrum was documented and classified according to Snyder [25] and Maffet [26] where appropriate. PTASRCTs were measured using the technique of Ellmann [6] with the 4-mm probe. The presence of intratendinous changes was assessed using the Bubble sign as described by Lo et al. [27] Other pathology of the glenohumeral ligaments and the rotator cuff was also documented. The impingement lesion within the bursa was graded using a shortened version of the Copeland-Levy classification [28] (grade B0 - Normal; grade B1 - Minor scuffing; grade B2 - Partial-thickness tear). The recorded mechanism of injury was established from the first consultation note.
Currently the senior author performs an intratendinous repair in situ with decompression for tears greater than 50% (unless the patient is unsuitable for a repair) and performs a decompression with debridement for those under 50%. Although definitive evidence for the best surgical treatment for PTASRCTS is not known, this algorithm corresponds to the current recommendations within the literature. [29],[30]
For statistical analysis, a 2×2 contingency table was constructed for frequency data and was analyzed by Yates corrected Chi-squared test for frequencies under five and by Pearson's uncorrected Chi-squared test for samples over five. The age of the groups was analyzed with an unpaired Student's t-test. Significance was documented for any result with a P-value less than 0.05.
| Results | | |
One hundred and seventy-seven patients over the age of 35 years underwent an arthroscopic procedure related to the rotator cuff within the study period. Of these, 55 patients had a full-thickness tear, 18 had an associated capsular release for adhesive capsulitis, and 4 had an associated arthroscopic stabilization (Bankart repair) procedure. This left 100 patients who had isolated primary cuff pathology (±ACJ pathology) for further analysis.
In total, 62 patients had a PTASRCT, of which 7 were greater than 50% thickness. Of these 62 patients, 7 had no bursal-sided pathology, 2 had an associated bursal-sided partial-thickness tear, and the rest had a grade B1 impingement lesion.
All the remaining 38 patients without a PTASRCT had a grade B1 impingement lesion with minor scuffing, hemorrhage or inflammation on the bursal side but no evidence of a partial tear. The mean age of the patients with a PTASRCT was 61 years (range 35-80, SD±10), and those without PTASRCT had a mean age of 52 years (range 35-73, SD ±9.6) (P=0.0001). The mean patient age for a PTASRCT over 50% was 67 years, whereas the mean age for a PTASRCT under 50% was 69 years (P=0.04). The operations performed for each group are presented in [Table 1]. Thirty-one patients had concomitant ACJ pathology requiring surgical treatment, of whom 17 had a PTASRCT and 14 had pure tendinopathy.
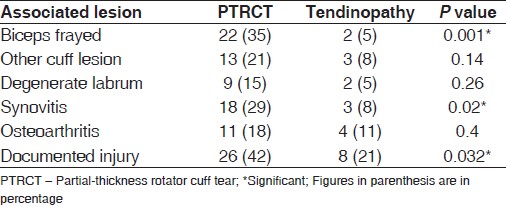
The patients with a PTASRCT had a significantly increased frequency of associated synovitis, biceps degeneration (fraying or tearing), and a documented injury [Table 2]. Of the patients with partial tears, 16 had sustained a fall, 6 had sustained the injury lifting a heavy weight, 3 had sustained the injury after strenuous exercise, and 1 was involved in a road traffic accident. All of the patients with a documented injury had symptoms commencing on the day of injury and all, except one, were asymptomatic prior to the injury. The mean time from injury to surgery was 19.5 months (range 7-72, SD ±15.6).
Apart from age, there was no significant difference between the groups for the size of the partial tears. There was also no significant difference in the grade of the bursal impingement or frequency of Superior Labrum Anterior to Posterior lesions and glenohumeral ligament abnormalities.
| Discussion | | |
This study has demonstrated that PTASRCTs are a common occurrence in patients requiring arthroscopic surgery for rotator cuff pathology over the age of 35 years. Almost two-thirds of our patients had some size of partial tear. This compares to an accumulated incidence of 18.5% within the literature for partial-thickness tears in the cadaveric population of mean age 70 years. [1] Predictably, this is an age-related phenomenon and the severity of the tear is also associated with age. The correlation with a degenerate biceps reflects the close association of degeneration of this structure with degeneration of the supraspinatus tendon, which has been well documented in rotator cuff tears. [31] The higher frequency of associated synovitis reflects that this is likely to be an intra-articular pathology and would support the theory that partial-thickness tears begin on the articular side.
It is an interesting fact that a documented injury is more frequently seen in patients with a partial tear compared to those with tendinopathy. Previously, clinical examination and pain have been found to be poor indicators in the diagnosis of partial tears. [32],[33] As only 42% of patients had a documented injury and 21% had tendinopathy, this is unlikely to be useful in the diagnosis. However, it may reflect an injury in a previously degenerate cuff. There is little evidence to suggest that internal impingement has taken a role in the etiology of these injuries. As only two patients had an associated bursal-sided partial tear, it is unlikely that extrinsic abrasion by the acromion has contributed either.
The age of 35 was chosen as an arbitrary age at which high-end athletic sports are unlikely to be performed, although this may be argued as a limitation. Both the Ellmann classification [6] and the Habermeyer classification [34] have three grades of articular-sided tears. However, as the inter-observer agreement of tear depth using an arthroscopic probe is poor [35] and as anatomical studies have shown a large variation in the medial to lateral dimension of the footprint (9.6-16 mm), [36],[37],[38] the tears were graded into just two groups. Other limitations of this study include the small sample size and its retrospective design that limits the data collection especially regarding further details of the injury patterns and severity sustained in the documented injuries. There was also a variation in the time from injury to surgery in patients with a documented injury that may have had an effect on the associated intra-articular findings at arthroscopy, although many of these were degenerative in nature.
| Conclusion | | |
This study has demonstrated that PTASRCTs are a common finding in patients undergoing arthroscopy for supraspinatus tendinopathy and can be associated with a recorded injury. They are associated with increasing age and degeneration of the biceps tendon with few associated bursal-sided tears. This would support the theory of intrinsic degeneration of the tendon in this age group and probably represent a different etiology to those seen in the young athletes.
| References | | |
| 1. | Reilly P, Macleod I, Macfarlane R, Windley J, Emery RJ. Dead men and radiologists don't lie: A review of cadaveric and radiological studies of rotator cuff tear prevalence. Ann R Coll Surg Engl 2006;88:116-21. 
|
| 2. | de Jesus JO, Parker L, Frangos AJ, Nazarian LN. Accuracy of MRI, MR arthrography, and ultrasound in the diagnosis of rotator cuff tears: A meta-analysis. AJR Am J Roentgenol 2009;192:1701-7.
|
| 3. | Dinnes J, Loveman E, McIntyre L, Waugh N. The effectiveness of diagnostic tests for the assessment of shoulder pain due to soft tissue disorders: A systematic review. Health Technol Assess 2003;7:iii,1-166.
|
| 4. | Modi CS, Smith CD, Ho K, Karthikeyan S, Boer R, Rai S, et al. Accuracy of high resolution ultrasonography in the diagnosis of articular-sided partial thickness rotator cuff tears. Shoulder and Elbow 2010;2:267-70.
|
| 5. | Löhr JF, Uhthoff HK. Epidemiology and pathophysiology of rotator cuff tears. Orthopade 2007;36:788-95.
|
| 6. | Ellman H. Diagnosis and treatment of incomplete rotator cuff tears. Clin Orthop Relat Res 1990;254:64-74.
|
| 7. | Weber SC. Arthroscopic debridement and acromioplasty versus mini-open repair in the treatment of significant partial-thickness rotator cuff tears. Arthroscopy 1999;152:126-31.
|
| 8. | McConville OR, Iannotti JP. Partial-thickness tears of the rotator cuff: Evaluation and management. J Am Acad Orthop Surg 1999;7:32-43.
|
| 9. | Andrews JR, Broussard TS, Carson WG. Arthroscopy of the shoulder in the management of partial tears of the rotator cuff: A preliminary report. Arthroscopy 1985;1:117-22.
|
| 10. | Brockmeier SF, Dodson CC, Gamradt SC, Coleman SH, Altchek DW. Arthroscopic intratendinous repair of the delaminated partial-thickness rotator cuff tear in overhead athletes. Arthroscopy 2008;24:961-5.
|
| 11. | Jobe CM. Superior glenoid impingement. Orthop Clin North Am 1997;28:137-43.
|
| 12. | Walch G, Boileau P, Noel E, Donell ST. Impingement of the deep surface of the supraspinatus tendon on the posterosuperior glenoid rim: An arthroscopic study. J Shoulder Elbow Surg 1992;1:238-45.
|
| 13. | Bigliani LU, Morrison DS, April EW. The morphology of the acromion and its relationship to the rotator cuff tears. Orthop Trans 1986;10:228.
|
| 14. | Neer CS. Anterior acromioplasty for the chronic impingement syndrome in the shoulder: A preliminary report. J Bone Joint Surg Am 1972;54:41-50.
|
| 15. | Sano H, Ishii H, Trudel G, Uhthoff HK. Histologic evidence of degeneration at the insertion of 3 rotator cuff tendons: a comparative study with human cadaveric shoulders. J Shoulder Elbow Surg 1999;8:574-9.
|
| 16. | Nakajima T, Rokuuma N, Hamada K, Tomatsu T, Fukuda H. Histologic and biomechanical characteristics of the supraspinatus tendon: Reference to rotator cuff tearing. J Shoulder Elbow Surg 1994;3:79-87.
|
| 17. | Ozaki J, Fujimoto S, Nakagawa Y, Masuhara K, Tamai S. Tears of the rotator cuff of the shoulder associated with pathological changes in the acromion. A study in cadavera. J Bone Joint Surg Am 1988;70:1224-30.
|
| 18. | Gartsman GM, Milne JC. Articular surface partial-thickness rotator cuff tears. J Shoulder Elbow Surg 1995;4:409-15.
|
| 19. | Yamanaka K, Matsumoto T. The joint side tear of the rotator cuff. A followup study by arthrography. Clin Orthop Relat Res 1994(304:68-73.
|
| 20. | Kartus J, Kartus C, Rostgard-Christensen L, Sernert N, Read J, Perko M. Long-term clinical and ultrasound evaluation after arthroscopic acromioplasty in patients with partial rotator cuff tears. Arthroscopy 2006;22:44-9.
|
| 21. | Liem D, Alci S, Dedy N, Steinbeck J, Marquardt B, Mollenhoff G. Clinical and structural results of partial supraspinatus tears treated by subacromial decompression without repair. Knee Surg Sports Traumatol Arthrosc 2008;16:967-72.
|
| 22. | Hawkins RJ, Kennedy JC. Impingement syndrome in athletes. Am J Sports Med 1980;8:151-8.
|
| 23. | Snyder SJ. Shoulder Arthroscopy. 2 nd ed. Philadelphia: Lippincott Williams and Wilkins; 2002.
|
| 24. | Outerbridge RE. The etiology of chondromalacia patellae. J Bone Joint Surg Br 1961;43:752-7.
|
| 25. | Snyder SJ. Arthroscopic classification of rotator cuff lesions and surgical decision-making. In: Snyder SJ, editor. Shoulder Arthroscopy. Philadelphia: Lippincott Williams and Wilkins; 2003. p. 201-7.
|
| 26. | Maffet MW, Gartsman GM, Moseley B. Superior labrum-biceps tendon complex lesions of the shoulder. Am J Sports Med 1995;23:93-8.
|
| 27. | Lo IK, Gonzalez DM, Burkhart SS. The bubble sign: an arthroscopic indicator of an intratendinous rotator cuff tear. Arthroscopy 2002;18:1029-33.
|
| 28. | Levy O, Sforza G, Dodenhoff RM, Copeland SA. Arthroscopic evaluation of the impingement lesion: pathoanatomy and classification. Subacromial plica as a cause of impingement in the shoulder. J Bone Joint Surg Br 2000;82(Supp. III):233.
|
| 29. | Finnan RP, Crosby LA. Partial-thickness rotator cuff tears. J Shoulder Elbow Surg 2010;19:609-16.
|
| 30. | Smith CD, Corner T, Morgan D, Drew S. Partial thickness rotator cuff tears: what do we know? Shoulder and Elbow 2010;2:77-82.
|
| 31. | Chen CH, Hsu KY, Chen WJ, Shih CH. Incidence and severity of biceps long head tendon lesion in patients with complete rotator cuff tears. J Trauma 2005;58:1189-93.
|
| 32. | Brownlow H, Smith C, Corner T, Neen D, Pennington R. Pain and stiffness in partial-thickness rotator cuff tears. Am J Orthop 2009;38:338-40.
|
| 33. | Bryant L, Shnier R, Bryant C, Murrell GA. A comparison of clinical estimation, ultrasonography, magnetic resonance imaging, and arthroscopy in determining the size of rotator cuff tears. J Shoulder Elbow Surg 2002;11:219-24.
|
| 34. | Habermeyer P, Krieter C, Tang KL, Lichtenberg S, Magosch P. A new arthroscopic classification of articular-sided supraspinatus footprint lesions: A prospective comparison with Snyder's and Ellman's classification. J Shoulder Elbow Surg 2008;17:909-13.
|
| 35. | Kuhn JE, Dunn WR, Ma B, Wright RW, Jones G, Spencer EE, et al. Interobserver agreement in the classification of rotator cuff tears. Am J Sports Med 2007;35:437-41.
|
| 36. | Curtis AS, Burbank KM, Tierney JJ, Scheller AD, Curran AR. The insertional footprint of the rotator cuff: an anatomic study. Arthroscopy 2006;22:609.
|
| 37. | Dugas JR, Campbell DA, Warren RF, Robie BH, Millett PJ. Anatomy and dimensions of rotator cuff insertions. J Shoulder Elbow Surg 2002;11:498-503.
|
| 38. | Ide J, Maeda S, Takagi K. Arthroscopic transtendon repair of partial-thickness articular-side tears of the rotator cuff: anatomical and clinical study. Am J Sports Med 2005;33:1672-9.
|
[Table 1], [Table 2]
| This article has been cited by | | 1 |
Development of a mouse model of supraspinatus tendon insertion site healing |
|
| Rebecca Bell,Peter Taub,Paul Cagle,Evan L. Flatow,Nelly Andarawis-Puri | | Journal of Orthopaedic Research. 2014; : n/a | | [Pubmed] | [DOI] | |
|
|
|
|