|
| Article Access Statistics | | | Viewed | 1515 | | | Printed | 75 | | | Emailed | 0 | | | PDF Downloaded | 6 | | | Comments | [Add] | | | Cited by others | 1 | | |
|


Click on image for details.
|
|
| |


 |
| Year : 2012 | Volume
: 6
| Issue : 1 | Page : 23-24 |
|
|
|
|
|
LETTER TO THE EDITOR Giant cell tumor of the supraspinatus tendon sheath causing shoulder impingement
Vignesh P Krishnamoorthy, Korula M Jacob, Pradeep M Poonnoose
Department of Orthopaedics-Unit II, Christian Medical College, Vellore, Tamil Nadu, India
Correspondence Address:
Vignesh P Krishnamoorthy
Department of Orthopaedics-Unit II, Christian Medical College, Vellore, Tamil Nadu - 632 004
India
 Source of Support: None, Conflict of Interest: None
DOI: 10.4103/0973-6042.94316

|
|
|
|
| Date of Web Publication | 26-Mar-2012 |
How to cite this article:
Krishnamoorthy VP, Jacob KM, Poonnoose PM. Giant cell tumor of the supraspinatus tendon sheath causing shoulder impingement. Int J Shoulder Surg 2012;6:23-4 |
Sir,
We report a case of a 44-year-old gentleman who presented with signs and symptoms of impingement of his left shoulder. He was found to have giant cell tumor (GCT) of the supraspinatus tendon sheath, which was the cause of impingement.
The patient presented to us with progressive left shoulder pain for a year, which worsened on overhead activity. He had consulted several surgeons and had received five intra-articular/subacromial injections in an attempt to relieve his pain, but with little success.
Clinical examination revealed marked wasting of the supraspinatus and infraspinatus muscles, with an ill-defined fullness located just above the spine of the scapula near the angle of the acromion. There was no local warmth, but the area was minimally tender. There was painful arc of abduction and a negative drop arm test. Neer's impingement test was positive.
Plain radiographs were unremarkable and ultrasonographic assessment done to rule out an associated cuff tear reported an infected subacromial bursa. No cuff tear was identified. Clinical features, however, suggested a non-infectious etiology. C-reactive protein (CRP) and erythrocyte sedimentation rate (ESR) were normal and the patient was never septic. A magnetic resonance imaging (MRI) scan was not done preoperatively due to a long waiting list and financial constraints. The patient was counseled about surgery and an arthroscopic subacromial decompression was planned, with the intention of assessing the swelling peri-operatively.
Under general anesthesia, the patient was positioned in the right lateral decubitus position. Arthroscopy of the glenohumeral joint was done and was unremarkable. The subacromial space was visualized from the posterior portal and there was no evidence of inflammation or infection. A minimal debridement was performed; the subacromial space was found to be adequate, and no cuff tear was seen. As the arthroscopic evaluation was negative, a transverse incision was made in the region of the swelling, over the supraspinatus fossa [Figure 1]. A well-encapsulated soft tissue swelling was found arising from the supraspinatus tendon, posterior to the subacromial bursa, which was excised en bloc for biopsy. The postoperative period was uneventful and the patient regained a full pain-free range of movement by the third week. The biopsy of the excised swelling showed a GCT of the left supraspinatus muscle tendon sheath [Figure 2].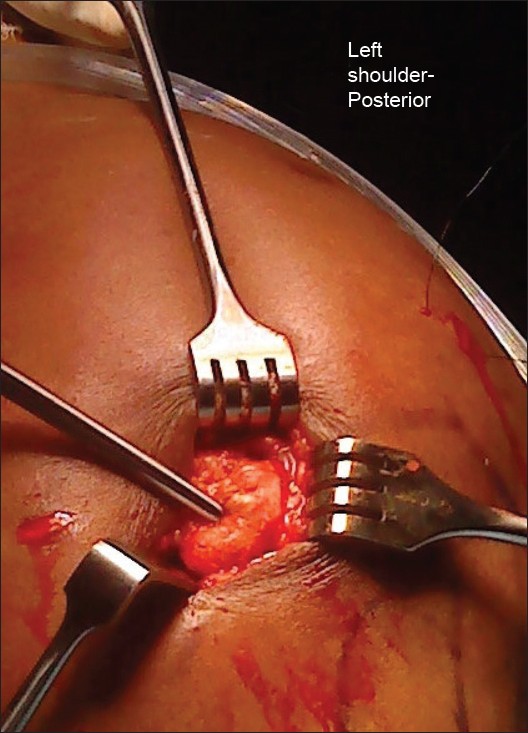 | Figure 1: Surgical exposure through a transverse incision in the supraspinatus fossa
Click here to view |
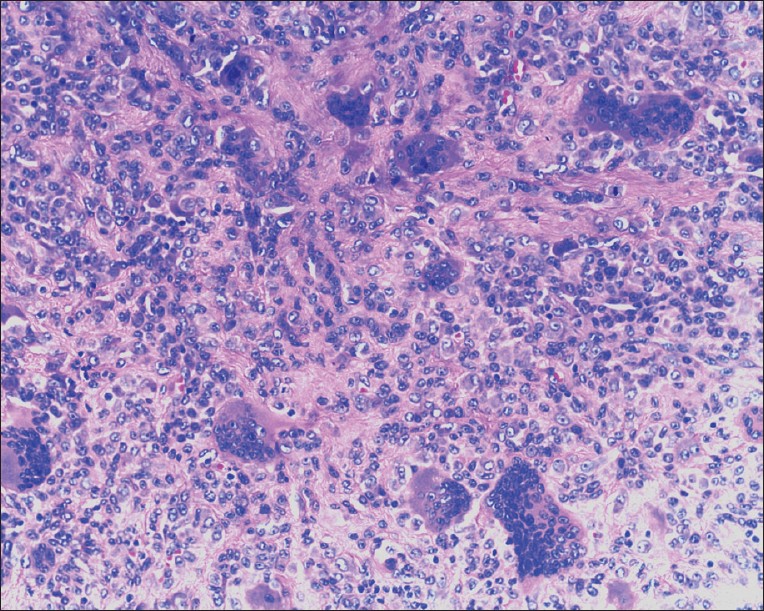 | Figure 2: ×20 photomicrograph showing an encapsulated tumor composed of sheets of polygonal to spindle-shaped mononuclear cells with interspersed osteoclast type multinucleate giant cells, histiocytes, and aggregates of foamy macrophages
Click here to view |
Giant cell tumors of tendon sheaths (GCTTS) are well-described entities, most commonly seen in the region of the hand and foot. [1] They are especially uncommon around the shoulder joint. To the best of our knowledge, there have been no reports of supraspinatus GCTTS presenting with impingement syndrome.
Bigliani and Levine [2] proposed a classification schema that organizes the various contributory factors for impingement syndrome. They can be broadly classified as intrinsic (intratendinous) or extrinsic (extratendinous), and further subdivided into primary or secondary etiologies. A primary etiology is either an intrinsic or extrinsic factor that is the direct cause of the impingement process. A secondary etiology is an independent factor such as instability or neurological injury that results in impingement. Based on this classification schema, GCT of the supraspinatus tendon sheath can be considered an intrinsic (intratendinous) primary pathology. [2]
In our case, the patient regained excellent motion postoperatively and the shoulder remained pain free at follow-up, a year after the surgery. He has had no recurrence to date.
Thus, GCTs of the supraspinatus tendon sheath should be considered a possible cause of subacromial impingement. This case showed that simple surgical excision of the tumor resulted in complete resolution of symptoms with immediate effect.
 References References | |  |
| 1. | Vasconez HC, Nisanci M, Lee EY. Giant cell tumour of the flexor tendon sheath of the foot. J Plast Reconstr Aesthet Surg 2008;61:815-8. 
[PUBMED] [FULLTEXT] |
| 2. | Bigliani LU, Levine WN. Current concepts review-subacromial impingement syndrome. J Bone Joint Surg Am 1997;79:1854-68.
[PUBMED] [FULLTEXT] |
[Figure 1], [Figure 2]
| This article has been cited by | | 1 |
Document Tenosynovial giant cell tumor arising on the scapular region |
|
| Fukuda, A., Ueno, T., Takayama, R., Futagami, A., Kawana, S. | | Case Reports in Dermatology. 2013; 5(3): 267-271 | | [Pubmed] | |
|
|
|
|
|











