| |


 |
| Year : 2012 | Volume
: 6
| Issue : 4 | Page : 121-125 |
|
|
|
|
|
CASE REPORT Septic failure is not a septic loosening: A case report of a failed shoulder prosthesis
Yde Engelsma1, Pieter Buma2, Pieter C Geervliet1, Arthur Van Noort1
1 Orthopaedic Department, Spaarne Hospital, Hoofddorp, Netherlands
2 Orthopaedic Research Laboratory, Radboud University Medical Centre Nijmegen, Netherlands
Correspondence Address:
Yde Engelsma
Spaarne Ziekenhuis, Hoofddorp, Ceintuurbaan 230-2, 1072GE Amsterdam
Netherlands
 Source of Support: None, Conflict of Interest: None
DOI: 10.4103/0973-6042.106225

|
|
|
|
| Date of Web Publication | 18-Jan-2013 |
 Abstract Abstract | | |
Septic failure of a shoulder arthroplasty due to a low-grade infection is generally called septic loosening. However, it is often not investigated if a prosthesis is genuinely loose. We present a case of a failed resurfacing prosthesis in a 70-year-old woman. This prosthesis failed due to a low-grade infection and a revision procedure was mandatory. All intraoperative cultures were positive and revealed a combination of bacteria. Nevertheless, histology revealed a macroscopic and a microscopic stable prosthesis with full osseointegration beneath the prosthesis. The general conception is that an infection leads to interface formation (with neutrophils) and loosening of the prosthesis. We debate this with the presentation of this case of a failed shoulder prosthesis and we think that periprosthetic infection and septic prosthetic loosening are two different entities.
Keywords: Infection, loosening, osseointegration, prosthesis, shoulder
How to cite this article:
Engelsma Y, Buma P, Geervliet PC, Noort AV. Septic failure is not a septic loosening: A case report of a failed shoulder prosthesis. Int J Shoulder Surg 2012;6:121-5 |
| Introduction | |  |
Infectious failure of a shoulder arthroplasty is a devastating complication requiring revision surgery. In orthopedic literature, a differentiation between septic and aseptic prosthetic loosening is often made. [1],[2],[3],[4] It is thought that cellular processes of the periprosthetic membrane with mobility of the implant lead to disintegration, osteolysis, and bone defects causing (septic) prosthetic loosening. [1],[2],[4] We present a case of a patient with a failed uncemented resurfacing shoulder arthroplasty due to a low-grade infection. Nevertheless, histology revealed a fully osseointegrated prosthesis. To our knowledge, a prosthetic failure due to low-grade infection with a histological proven stable prosthesis has never been reported.
| Case Report | | |
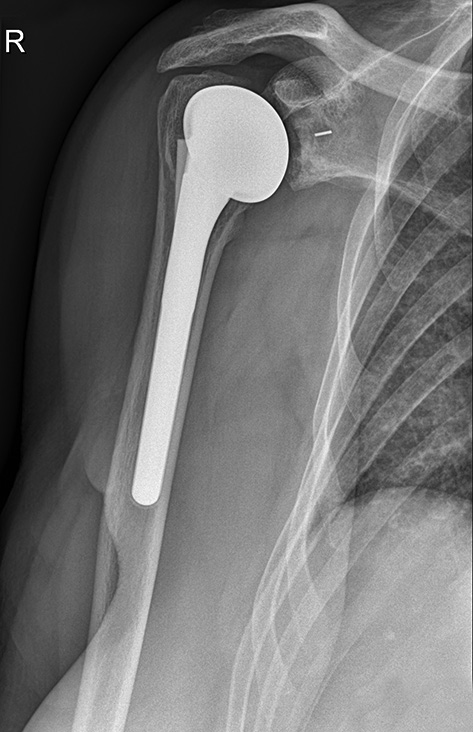
A 70-year-old woman presented at our outpatient department with primary glenohumeral osteoarthritis at the right side [Figure 1]. She had osteoarthritis in multiple joints and underwent previously a bilateral total knee replacement. General medical history revealed diverticulitis, mild chronic obstructive pulmonary disease (COPD), and atrial fibrillation. Because of her persisting pain non-responding to conservative treatment, she was scheduled for a resurfacing shoulder prosthesis on the right side. Standard antibiotic prophylaxis of three gifts of 1 g cefazoline in 24 h was used. A deltopectoral approach was used during surgery and the rotator cuff was intact. The osteophytes were removed and the 44 mm uncemented resurfacing shoulder prosthesis (DePuy; Global Cap) was placed [Figure 2]. The glenoid was sclerotic without any bone loss and microfracturing was performed with the chondropick. No wound problems occurred and the patient was discharged 2 days after surgery. The physiotherapist accompanied a standard rehabilitation program with initial restricted passive range of motion. During the first 4 months, the patient was very satisfied with painless shoulder and full range of motion. | Figure 1: AP X-ray of the right shoulder showing osteoarthritis of the glenohumeral joint
Click here to view |
 | Figure 2: Immediate postoperative X-ray of the resurfacing shoulder prosthesis
Click here to view |
Since this initial period, she suffered progressive shoulder pain. At examination, there was a painful arc and the supraspinatus resistance test was painful, but there were no clinical signs of a cuff rupture. It was thought that rotator cuff tendinitis caused this pain and an arthroscopic subacromial decompression was performed. Preoperative 1 gr of cefazoline was given. During surgery the rotator cuff was intact. At this time, an infection was not considered and therefore the glenohumoral joint was neither inspected nor aspirated. However, the subacromial decompression did not relieve the complaints and the range of motion gradually decreased. At 2 years after the arthroplasty, the patient had pain on the anterior side of the shoulder, mild rest pain, increased pain whilst lifting, and a restricted forward flexion of 90° and external rotation of 50°. No clinical infectious signs were present and the cuff seemed intact. Her erythrocyte sedimentation rate (ESR) was slightly elevated since the first operation (between 30 and 45) with a normal C-reactive protein (CRP). However, the biochemical markers are not completely reliable for an infection due to her diverticulitis. The X-rays showed a well-positioned prosthesis without signs of loosening and some progression in glenoid erosion [Figure 3]. To exclude an infection, a culture of intra-articular fluid (obtained by fine-needle aspiration) was done, which was negative. | Figure 3: Two years postoperative, the X-ray shows progressive glenoid erosion with a well-positioned prosthesis
Click here to view |
Because of the persisting pain and signs of progressive of glenoid erosion on plain radiographs, a conversion from hemi to total shoulder prosthesis was performed [Figure 4]. Three times cefozline was given perioperative. Intraoperative inspection of the joint showed induration of the synovium and a sclerotic glenoid with irregular erosions. The cap was macroscopically solidly incorporated in the bone. Routine swabs and tissue samples from the bone and synovium were taken for cultures. The peri- and postoperative course was uneventful with normal wound healing. However, after 10 days, all intraoperative cultures revealed a combination of micro-organisms and antibiotic therapy was started. The Pantoea agglomerans, Staphylococcus epidermidis, and Propionium acnes were found in all four operative cultures. | Figure 4: Postoperative situation after conversion to a total shoulder prosthesis
Click here to view |
The resected resurfacing prosthesis was sent to a specialized bone lab. It was fixated in buffered formalin at 4°C and the prosthesis was cut along the central stem. After embedding of the halves in polymethyl methacrylate (PMMA), the surfaces were polished, sputter coated with cold, and examined by scanning electron microscope (SEM). Then, surfaces were polished again, acid etched to partially remove the PMMA, and then stained with basic fuchsin and photographed. A microscopic stable prosthesis with full osseointegration was seen. The bone was intact, generally osteoporotic, and in good contact with the coating of the prosthesis. There were no signs of soft tissue interface formation due to loosening or microfractures of the bone trabeculae [Figure 5],[Figure 6],[Figure 7] and [Figure 8].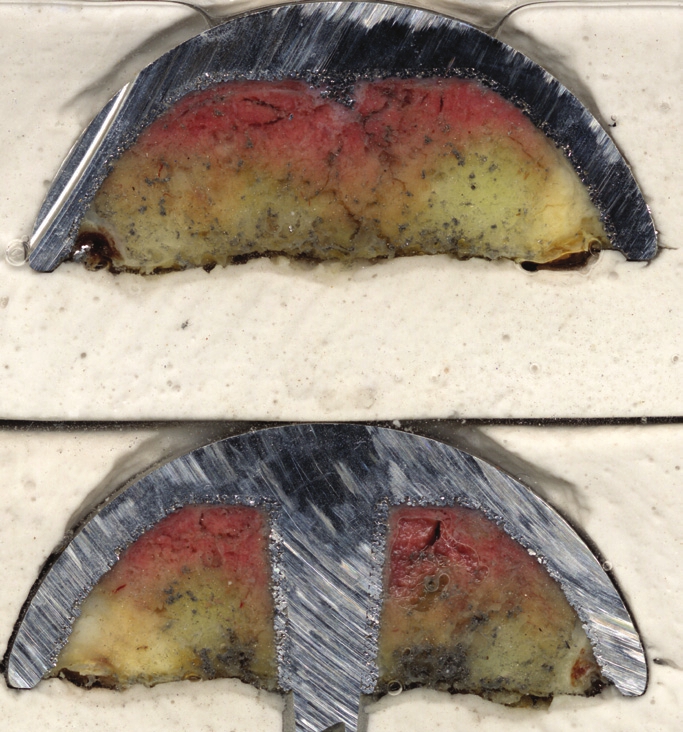 | Figure 5: Cross-sections of the uncemented resurfacing shoulder prosthesis (DePuy; Global Cap). Most tissue under the cup is fatty marrow with some scarce and thin bone trabeculae
Click here to view |
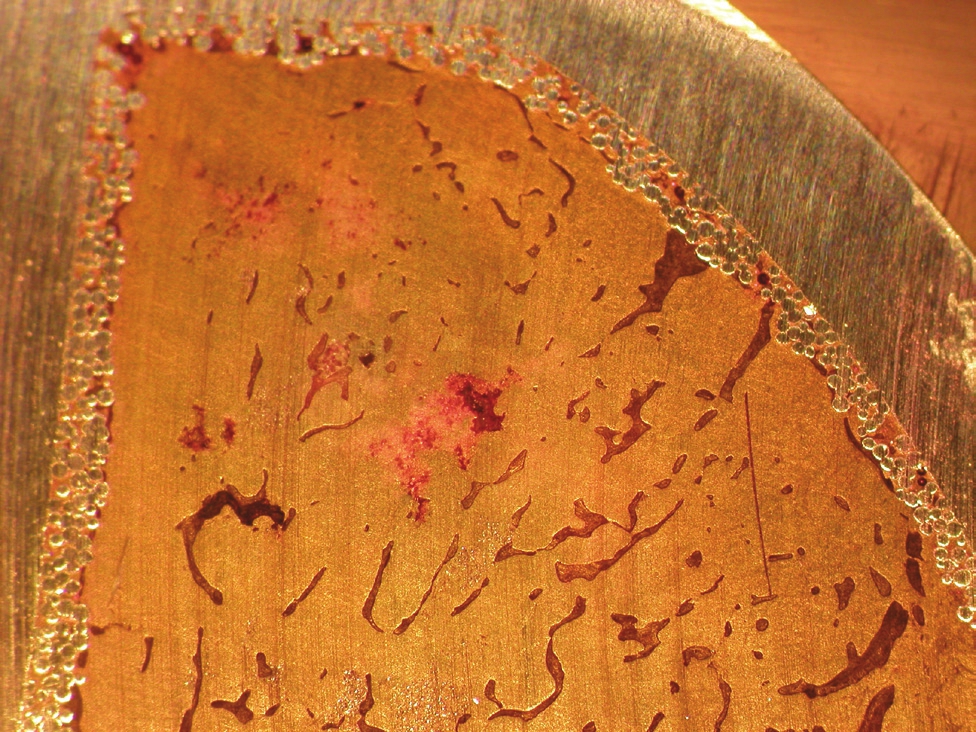 | Figure 6: Enlargement of area directly under the cup. Notice bone trabeculae running in the direction of the porous coating of the cup
Click here to view |
 | Figure 7: Low magnification of plastic embedded and polished surface of area directly under the porous coating
Click here to view |
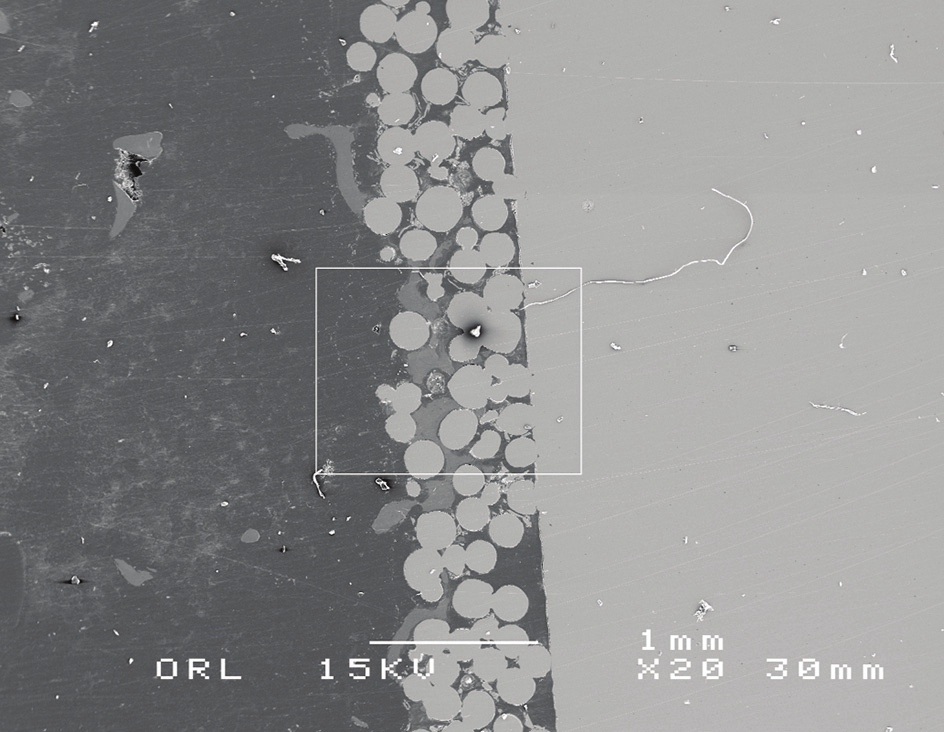
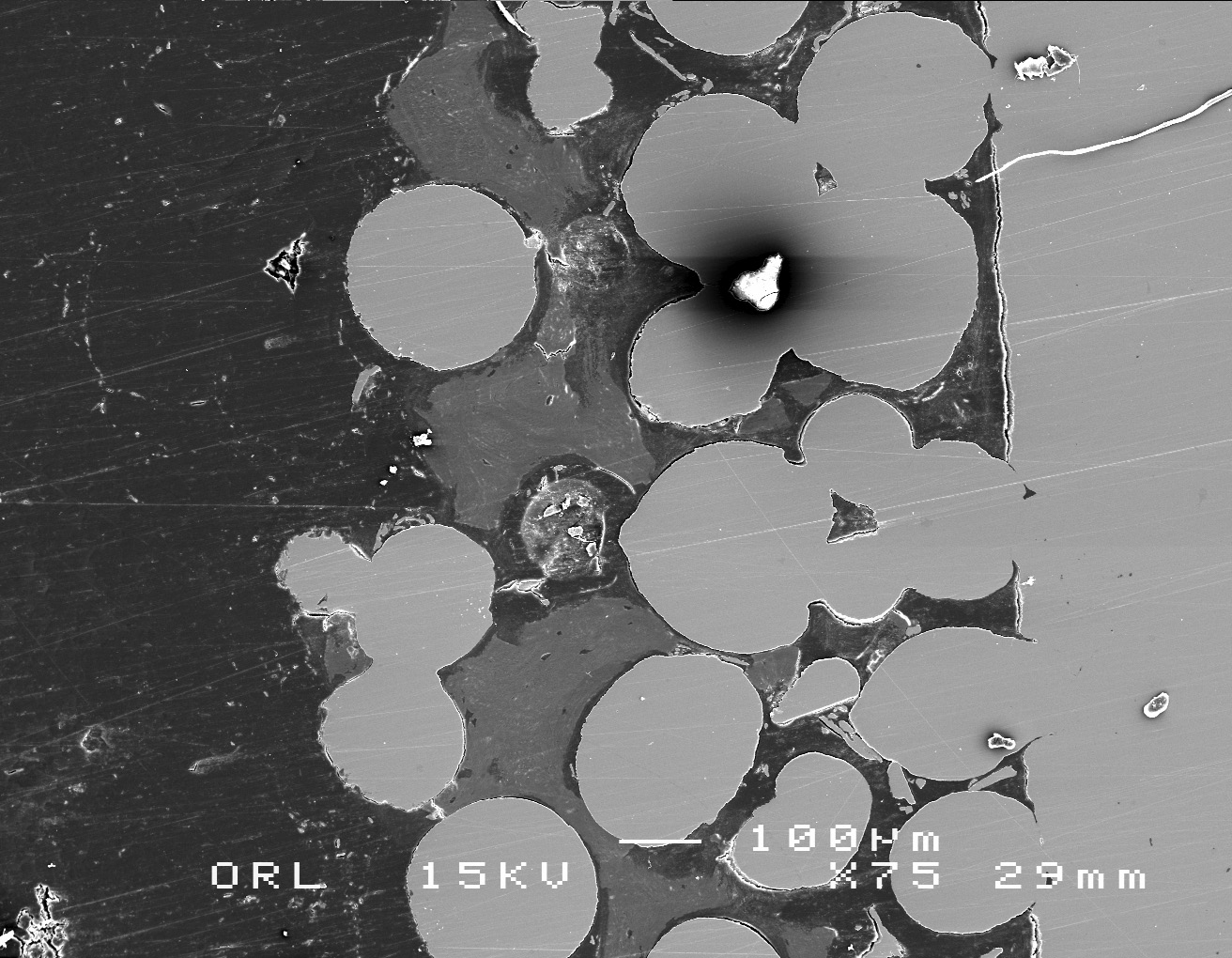 | Figure 8: Higher magnification of boxed area in Figure 3 showing bone trabeculae in close contact with the porous coating
Click here to view |
These findings led to the conclusion that the resurfacing prosthesis failed due to a painful low-grade infection, without loosening of the prosthesis. According to the advice of the microbiologist, prolonged antibiotic regiment was started until the ESR and CRP normalized after 3 months. The rehabilitation period was longer than after the first operation, but uneventful and no wound problems occurred. At the last follow-up, 24 months postoperative, she was satisfied with her shoulder. She had a pain-free active forward flexion of 140°, endorotation of 70°, and exorotation of 30°. There were no clinical or biochemical signs of infection and the X-ray showed a correct position of the prosthesis with no signs of loosening [Figure 9].
| Discussion | | |
The results of shoulder arthroplasty are generally good; however, failures do occur due to prosthesis malalignment, infection, fracture, and prosthesis loosening due to various causes. [5],[6],[7] Infection is a devastating complication requiring revision surgery, with reported rates between 0% and 4% in primary shoulder arthroplasties. [5],[6],[7],[8] The diagnosis of infection is often classified as high (acute) or low grade (chronic). It is based on a combination of symptoms, laboratory tests, findings in physical and radiological examinations, and confirmed by positive intraoperative cultures. [1],[4],[8],[9] While high-grade infections are easily recognizable from clinical signs, chronic or low-grade infection can be a serious diagnostic challenge [4] In these cases, most of the pre-operative investigations prove not to be extremely useful and positive culture rates can be as high as 25% in presumably uninfected shoulders during revision arthroplasty. [1],[6],[7],[9]
Patients with a failed shoulder prosthesis often present with pain and stiffness, whatever the cause is, as illustrated in our case. [6] Although the preoperative analysis (including intra-articular fluid culture) did not reveal a septic cause of the failure, the intraoperative culture revealed a combination of bacteria, including P. acnes. The ideal antibiotic regimen is disputable and we followed the advice of our microbiologist with a prolonged antibiotic treatment of 3 months.
Septic loosening and osseointegration
The development of the definition of a periprosthetic infection is still ongoing; the results of microbiology cultures of the periprosthetic tissues are considered to be gold standard. [10] Confusingly, a periprosthetic infection is often called septic loosening and debate has even been raised concerning whether living (proliferating) microorganisms are indeed necessary for septic loosening. [2] The earliest and probably clinically the most important step in periprosthetic infections is the competition between tissue cell integration and bacterial adhesion to the same surface. When an implant is surgically placed in bone, there are numerous biological, physical, chemical, thermal, and other factors that determine whether or not osseointegration will occur. [2],[11] An acute inflammatory response in bone and the surrounding soft tissues is caused by the surgical procedure. This may resolve and an initial lace-like trabecular bony layer then surrounds the implant, which leads to an osseointegrated implant. Alternatively, inflammation may persist and develop into a chronic phase with eventual fibrosis and loosening. [2] Factors associated with chronic inflammation and fibrosis include poor local blood supply of the bone bed, interfacial motion (especially large shear forces), infection, prolonged allergic or foreign body responses, and chemical and thermal trauma. [2],[11]
It is known that a well-fixed and stable implant is a necessity for long-term pain-free function of a joint replacement. In successfully osseointegrated implants, the junction between implant and host bone ought to be a tight or bony union. [2],[11] On the other hand, it has been described that a layer of connective tissue develops between the bone and prosthesis in both septic and aseptic loosening. [3],[12],[13],[14] And even well-fixed implants may have these membranes, even though they are considerably thinner. [11],[12] Several pathological mechanisms that may lead to loosening have been described and have been summarized in a histological classification which defines four types of periprosthetic membranes. [3],[12],[15] The histological feature that suggests the pathological diagnosis of septic loosening is the presence of numerous inflammatory cells, particularly neutrophil polymorphonuclear leukocytes (neutrophils) in the periprosthetic membrane. Although the reliability of this investigation is questionable, it is agreed that the presence of numerous neutrophils in the periprosthetic tissue strongly correlates with septic loosening. [12],[15] However, whether or not failure of an infected prosthesis is due to loosening with interface formation remains unclear.
In our case, the histological analysis of the shoulder prosthesis did not fit the standardized histological classification. This was due to the fact that we did not find a periprosthetic interface as the bone was fully integrated onto the hydroxyapatite-coated undersurface of the prosthesis. This is in contrast to the theory that an infection leads to interface formation and subsequently loosening of the prosthesis.
In conclusion, we present a case of a failed hemi-shoulder prosthesis due to a periprosthetic infection, which was histologically fully osseointegrated. The general conception is that an infection leads to interface formation (with neutrophils) and loosening of the prosthesis. We debate this with the presentation of this case and we think that periprosthetic infection and septic prosthetic loosening are two different entities.
| References | | |
| 1. | Bauer TW, Schils J. The pathology of total joint arthroplasty. II. Mechanisms of implant failure. Skeletal Radiol 1999;28:483-97. 
|
| 2. | Goodman SB, Barrena EG, Takagi M, Konttinen YT. Biocompatibility of total joint replacements: A review. J Biomed Mater Res A 2008;90:603-18.
|
| 3. | Krenn V, Morawietz L, Jakobs M, Kienapfel H, Ascherl R, Bause L, et al. Joint endoprosthesis pathology: Histopathological diagnostics and classification. Pathologe 2011;32:210-9.
[PUBMED] |
| 4. | Pizzoferrato A, Ciapetti G, Stea S, Toni A. Cellular events in the mechanisms of prosthesis loosening. Clin Mater 1991;7:51-81.
[PUBMED] |
| 5. | Boileau P, Sinnerton RJ, Chuinard C, Walch G. Arthroplasty of the shoulder. J Bone Joint Surg Br 2006;88:562-75.
[PUBMED] |
| 6. | Franta AK, Lenters TR, Mounce D, Neradilek B, Matsen FA 3 rd . The complex characteristics of 282 unsatisfactory shoulder arthroplasties. J Shoulder Elbow Surg 2007;16:555-62.
|
| 7. | Kelly JD 2 nd , Hobgood ER. Positive culture rate in revision shoulder arthroplasty. Clin Orthop Relat Res 2009;467:2343-8.
|
| 8. | Amaravathi. Analysis of infection in shoulder arthroplasty: A multicentre study. Eur J Orthop Surg Traumatol 2012;22:145-50.
|
| 9. | Topolski MS, Chin PY, Sperling JW, Cofield RH. Revision shoulder arthroplasty with positive intraoperative cultures: The value of preoperative studies and intraoperative histology. J Shoulder Elbow Surg 2006;15:402-6.
[PUBMED] |
| 10. | Bauer TW, Parvizi J, Kobayashi N, Krebs V. Diagnosis of periprosthetic infection. J Bone Joint Surg Am 2006;88:869-82.
[PUBMED] |
| 11. | Bauer TW, Schils J. The pathology of total joint arthroplasty. I. Mechanisms of implant fixation. Skeletal Radiol 1999;28:423-32.
|
| 12. | Morawietz L, Classen RA, Schroder JH, Dynybil C, Perka C, Skwara A, et al. Proposal for a histopathological consensus classification of the periprosthetic interface membrane. J Clin Pathol 2006;59:591-7.
|
| 13. | Levy O, Copeland SA. Cementless surface replacement arthroplasty (Copeland CSRA) for osteoarthritis of the shoulder. J Shoulder Elbow Surg 2004;13:266-71.
[PUBMED] |
| 14. | Revell PA. The combined role of wear particles, macrophages and lymphocytes in the loosening of total joint prostheses. J R Soc Interface 2008;5:1263-78.
[PUBMED] |
| 15. | Pandey R, Drakoulakis E, Athanasou NA. An assessment of the histological criteria used to diagnose infection in hip revision arthroplasty tissues. J Clin Pathol 1999;52:118-23.
[PUBMED] |
[Figure 1], [Figure 2], [Figure 3], [Figure 4], [Figure 5], [Figure 6], [Figure 7], [Figure 8], [Figure 9]
|