|
| Article Access Statistics | | | Viewed | 771 | | | Printed | 19 | | | Emailed | 0 | | | PDF Downloaded | 6 | | | Comments | [Add] | | |
|


Click on image for details.
|
|
| |


 |
| Year : 2013 | Volume
: 7
| Issue : 3 | Page : 125-126 |
|
|
|
|
|
LETTER TO THE EDITOR Arthroscopic assisted removal of screws from proximal humeral locking plates
Rupen Dattani, Vipul R Patel
South West London Elective Orthopaedic Centre, Epsom, Surrey, KT18 7EG, United Kingdom
Correspondence Address:
Rupen Dattani
South West London Elective Orthopaedic Centre, Dorking Road, Epsom, Surrey, KT18 7EG
United Kingdom
 Source of Support: None, Conflict of Interest: None
DOI: 10.4103/0973-6042.118914

|
|
|
|
| Date of Web Publication | 25-Sep-2013 |
How to cite this article:
Dattani R, Patel VR. Arthroscopic assisted removal of screws from proximal humeral locking plates. Int J Shoulder Surg 2013;7:125-6 |
Sir,
Osteosynthesis using the proximal humeral locking plates has shown promising results in the management of displaced and unstable proximal humeral fractures. [1] However, unrecognized screw penetration of the humeral head during the surgery and loss of fracture reduction, especially in patients over 60 years of age, [2] resulting in screw cut out accounts for nearly one-third of all patients requiring a re-operation to remove or exchange the offending screw. We describe a minimally invasive technique for removal or exchange of prominent screws enabling surgery to be undertaken as soon as the problem is recognized.
Pre-operative planning on patients requiring removal of screws includes radiographs in two planes Anterior-Posterior (AP) and axillary lateral) to identify the prominent screw(s), which require removal. If doubt remains about the precise location of the offending screw then fluoroscopy using an image intensifier may be undertaken prior to the arthroscopy. Shoulder arthroscopy is performed in the lateral decubitis position with balanced traction. Glenohumeral arthroscopy and subacromial bursoscopy is performed using a 30° arthroscope introduced through standard posterior and postero-lateral portals respectively. Diagnostic glenohumeral arthroscopy will reveal the prominent screw(s) [Figure 1]a and any associated glenoid erosion [Figure 1]b. Through subacromial bursoscopy, scar tissue overlying the plate is excised with a combination of a radiofrequency device, a shaver and a labral elevator to expose the heads of the screws [Figure 1]c. The screw(s) to be removed are identified and a spinal needle used to determine the position of an accessory portal, which will allow insertion of a screw driver along the axis of the screw to be removed [Figure 1]d. This portal, which is often at the level of the surgical neck of the humerus, is established by incising the skin only with a knife and then inserting a round-tipped arthroscopic trocar through the deeper tissues to avoid injury to branches of the axillary nerve. Axial pressure is maintained along the screwdriver to prevent disengagement of the tip of the screw driver from head of the screw. When the last few threads of the screw remain engaged the screw driver may be withdrawn and the screw held with a toothed grasper as it is removed [Figure 1]e. The glenohumeral joint can be examined after the screw is withdrawn to ensure that the correct screw has been removed. The removed screw can be exchanged with a shorter screw if deemed necessary for fracture stability.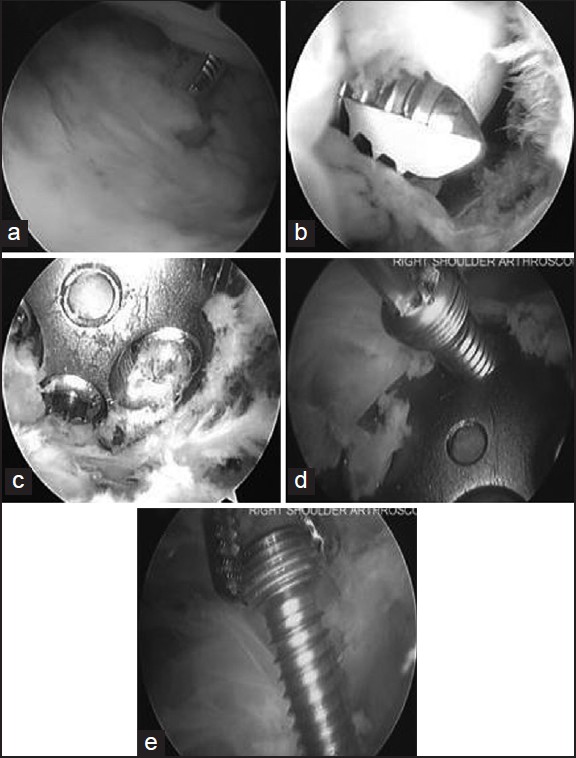 | Figure 1: Right shoulder arthroscopic images obtained from a posterior portal using a 30° arthroscope and performed in the lateral decubitis position, in a patient undergoing screw removal. Diagnostic glenohumeral arthroscopy reveals the prominent screw (a) and associated glenoid erosion (b). Through subacromial bursoscopy, the plate is exposed after excision of scar tissue with a combination of a radiofrequency device, a shaver and a labral elevator (c). The screw to be removed is identified (d) and grasped with a needle holder as it is withdrawn (e)
Click here to view |
Anatomic studies assessing the relationship of the axillary nerve and proximal humerus plates have shown that the six most proximal screw holes of commonly used plates are in the "safe zone" and do not pose a risk to the axillary nerve. [3] We therefore only advocate this technique for removal of proximal screws and not the calcar and shaft screws. An open procedure to remove the prominent screw(s) may be associated with potential complications such as pain related to an open surgical approach, infection, soft-tissue disruption and neurovascular injury. [4] Arthroscopic-assisted screw removal after osteosynthesis of the proximal humerus fractures provides all of the benefits of hardware removal without the risks associated with open surgery.
 References References | |  |
| 1. | Leonard M, Mokotedi L, Alao U, Glynn A, Dolan M, Fleming P. The use of locking plates in proximal humeral fractures: Comparison of outcome by patient age and fracture pattern. Int J Shoulder Surg 2009;3:85-9. 
[PUBMED]  |
| 2. | Brunner F, Sommer C, Bahrs C, Heuwinkel R, Hafner C, Rillmann P, et al. Open reduction and internal fixation of proximal humerus fractures using a proximal humeral locked plate: A prospective multicenter analysis. J Orthop Trauma 2009;23:163-72.
|
| 3. | Stecco C, Gagliano G, Lancerotto L, Tiengo C, Macchi V, Porzionato A, et al. Surgical anatomy of the axillary nerve and its implication in the transdeltoid approaches to the shoulder. J Shoulder Elbow Surg 2010;19:1166-74.
|
| 4. | Kirchhoff C, Braunstein V, Kirchhoff S, Sprecher CM, Ockert B, Fischer F, et al. Outcome analysis following removal of locking plate fixation of the proximal humerus. BMC Musculoskelet Disord 2008;9:138.
|
[Figure 1]
|
|











