|
| Article Access Statistics | | | Viewed | 1001 | | | Printed | 39 | | | Emailed | 0 | | | PDF Downloaded | 4 | | | Comments | [Add] | | |
|


Click on image for details.
|
|
| |


 |
| Year : 2013 | Volume
: 7
| Issue : 3 | Page : 124-125 |
|
|
|
|
|
LETTER TO THE EDITOR An uncommon complication following synthetic ligament reconstruction of the acromioclavicular joint
Catherine T Platts, Anik D Chatterjee, Amol A Tambe
Department of Trauma and Orthopaedic Surgery, Royal Derby Hospital, Derby, United Kingdom
Correspondence Address:
Catherine T Platts
Royal Derby Hospital, Uttoxeter Road, Derby
United Kingdom
 Source of Support: None, Conflict of Interest: None
DOI: 10.4103/0973-6042.118913

|
|
|
|
| Date of Web Publication | 25-Sep-2013 |
How to cite this article:
Platts CT, Chatterjee AD, Tambe AA. An uncommon complication following synthetic ligament reconstruction of the acromioclavicular joint. Int J Shoulder Surg 2013;7:124-5 |
Sir,
We highlight a method of addressing the problem of lateral clavicle fracture post acromioclavicular joint reconstruction, in the presence of a ligament loop and the screw used to anchor the ligament. This is an uncommon presentation and poses a management dilemma.
We present this case to highlight the problem and our management plan giving a good functional end result, and demonstrate a successful clinical outcome.
A 21-year-old gentleman presented to our institution in March 2009 after sustaining a direct injury to the tip of his left shoulder whilst playing rugby. He was found to have an acute type III acromioclavicular (AC) joint dislocation. This was a closed isolated injury with no neurovascular compromise.
After appropriate counselling with the patient, a plan of conservative treatment was proposed. 3 months later the patient returned to the clinic. He had been unable to partake in any sporting activity and had difficulty in doing his activities of daily living. At this point, the decision was taken to perform a left shoulder AC joint reconstruction on the basis of his ongoing symptoms. This was duly carried out using the Nottingham Surgilig. The lateral end of clavicle was excised during the procedure. 4 months post-operatively there were no concerns, and the patient demonstrated a good range of movement, returning to his activities. He was thus discharged.
In March 2011, the patient was tackled during a football match, sustaining an injury to the lateral end of his left clavicle. He sustained a fracture through the clavicle at the surgilig site where it is anchored to the lateral end of the clavicle with a small fragment screw.
This appeared undisplaced, the patient was otherwise asymptomatic, and hence was treated conservatively in a sling being mindful that the Ligament might cheese-wire through the fracture site. At 2 months, the patient had developed increasing pain around the fracture site [Figure 1]. There was a step deformity laterally over the clavicle which was reducible. The patient also suffered with a restricted range of movement. X-rays showed osteolysis around the screw site in the clavicle, with non-union of the fracture. | Figure 1: X-ray at 2 months after initial operation demonstrating osteolysis at the fracture site
Click here to view |
This posed a problem as the lateral fragment of the clavicle was too small to be captured effectively by a plate and a repeat coracoclavicular reconstruction would have been difficult given the osteolysis around the screw.
We decided to use a clavicle hook plate (Synthes) to address this problem along with removal of the screw in the fracture site. During surgery, the loose screw was removed easily. The polyester ligament appeared to be encapsulated with fibrous tissue and was left undisturbed. The 3.5 mm hook plate spanned across the lateral clavicle fragment and was anchored below the acromion as per hook plate technique. Autogenous bone graft was used to supplement the fracture area with a screw gaining purchase in the lateral clavicle fragment. Sling was provided for 6 weeks. 14 weeks post-surgery the patient demonstrated a full range of movement without pain, no deformity and a stable AC joint. The clavicle had healed clinically and radiologically [Figure 2]. We plan to remove the Hook plate electively.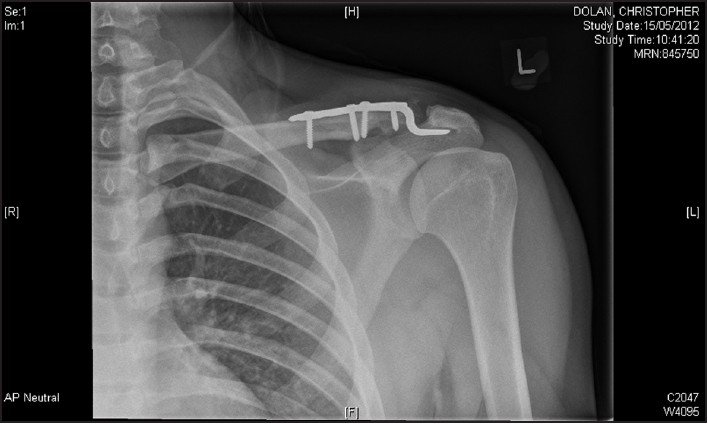 | Figure 2: Final radiological result after screw removal and hook plate fixation
Click here to view |
We highlight a method of addressing the problem of lateral clavicle fracture post AC joint reconstruction in the presence of a ligament loop and the screw used to anchor the ligament.
The clavicle hook plate has been used as a treatment option for acute displaced lateral clavicle fractures as well as acromioclavicular joint injuries. There has been some concern particularly regarding acromial erosion, plate pull off and rotator cuff damage with the clavicle hook plate. [1],[2]
In this particular case, the hook plate was used effectively to deal with a traumatic fracture following AC joint reconstruction with a good result. There are no similar reported cases.
Surgeons dealing with and treating these injuries need to be aware of the potentially unusual complication of fracture of the lateral clavicle through the screw site and consider using the hook plate if deemed appropriate, should they encounter this problem. This is an uncommon complication of a fracture, with adapted revision reconstruction. However, it is important that such complications are presented, to highlight any further cases of fracture through the ligament site.
 References References | |  |
| 1. | Muramatsu K, Shigetomi M, Matsunaga T, Murata Y, Taguchi T. Use of the AO hook-plate for treatment of unstable fractures of the distal clavicle. Arch Orthop Trauma Surg 2007;127:191-4. 
|
| 2. | Chandrasenan J, Badhe S, Cresswell T, De Beer J. The clavicular hook plate: Consequences in three cases. Eur J Trauma Emerg Surg 2007;33:557-9.
|
[Figure 1], [Figure 2]
|
|











