| |


 |
| Year : 2013 | Volume
: 7
| Issue : 4 | Page : 132-138 |
|
|
|
|
|
SURGICAL TECHNIQUE Acromioclavicular reconstruction using hook plate and anterior tibial tendon allograft with triple tunnel: The early results of revision surgery using a novel surgical technique
Alper Deveci1, Ahmet Firat2, Serdar Yilmaz1, Ahmet Ozgur Yildirim3, Halil I Acar4, Kazim O Unal1, Murat Bozkurt5
1 Department of Orthopaedics and Traumatology, Ankara Etlik Ihtisas Educational and Research Hospital, Ankara, Turkey
2 Department of Orthopaedics and Traumatology, Ankara Kecioren Educational and Research Hospital, Ankara, Turkey
3 Department of Orthopaedics and Traumatology, Ankara Numune Educational and Research Hospital, Ankara, Turkey
4 Department of Anatomy, Faculty of Medicine, Ankara University, Ankara, Turkey
5 Department of Orthopaedics and Traumatology, Faculty of Medicine, Yildirim Beyazit University, Ataturk Training and Research Hospital, Ankara, Turkey
Correspondence Address:
Serdar Yilmaz
Department of Orthopaedics and Traumatology, Orthopaedics and Traumatology Clinic, Etlik Ihtisas Training and Research Hospital, Ankara
Turkey
 Source of Support: None, Conflict of Interest: None
DOI: 10.4103/0973-6042.123513

|
|
|
|
| Date of Web Publication | 24-Dec-2013 |
 Abstract Abstract | | |
In this study, a new modified surgical technique is presented for anatomic acromioclavicular (AC) joint reconstruction made by the application of anterior tibialis tendon autograft, three-way tunnel (two clavicular and one coracoid) and hook plate. The study is aimed to evaluate the post-operative short-term results of patients who underwent this treatment. A total of 11 patients underwent AC joint reconstruction because of persistent AC subluxation. In this reconstruction, a triple tunnel was made between the coracoid and the clavicle to anatomically restore the coracoclavicular (CC) ligament and an allograft was passed through the tunnels resembling conoid and trapezoid ligaments. The tendon had to be non-weight bearing at the appropriate tension to provide rapid and appropriate integration of the tendon in the tunnel. This was maintained by applying a hook plate. The hook plate method was used to protect the reconstructed ligament during the healing process as it has a similar hardness to that of the natural AC joint and provides rigid fixation. For a more comprehensive description of the technique, a cadaver demonstration was also performed. The mean follow-up period was 25.3 months (range: 18-34 month). None of the patients had a loss of reduction at the final follow-up. When the constant scores were examined, of the total 11 patients, 2 (18.2%) 38,39 had excellent results, 6 (54.5%) had good results and 3 (27.3%) had fair results. It can be seen that this newly described reconstruction technique has successful short-term results as an anatomic method and can be used effectively in revision cases. However, there is a need for further biomechanical and clinical studies to make comparisons with other techniques.
Keywords: Acromioclavicular joint, allograft, cadaver, reconstruction, surgical revision
How to cite this article:
Deveci A, Firat A, Yilmaz S, Yildirim AO, Acar HI, Unal KO, Bozkurt M. Acromioclavicular reconstruction using hook plate and anterior tibial tendon allograft with triple tunnel: The early results of revision surgery using a novel surgical technique. Int J Shoulder Surg 2013;7:132-8 |
How to cite this URL:
Deveci A, Firat A, Yilmaz S, Yildirim AO, Acar HI, Unal KO, Bozkurt M. Acromioclavicular reconstruction using hook plate and anterior tibial tendon allograft with triple tunnel: The early results of revision surgery using a novel surgical technique. Int J Shoulder Surg [serial online] 2013 [cited 2016 May 22];7:132-8. Available from: http://www.internationalshoulderjournal.org/text.asp?2013/7/4/132/123513 |
| Introduction | |  |
The acromioclavicular (AC) and coracoclavicular (CC) ligaments have a synergistic role in the stabilization of the AC joint. The AC ligament controls horizontal movements in particular while the CC ligament has more control of vertical movements. [1],[2] There are currently more than 60 defined surgical techniques for acute and chronic AC joint injuries. [3],[4],[5] Of these, the Weaver-Dunn and Bosworth procedures are the oldest and still the most widely used techniques. [6],[7] A rate of 10% impairment has been reported in the literature after surgery with standard techniques. [5],[7],[8],[9],[10] Although Bosworth and its modified techniques are easy to apply, fixation failure may occur. [9],[10] The success rates vary depending on the surgical technique used, the severity of the injury and the integrity of the anatomic structures.
Treatment of recurrent AC joint dislocation is difficult after primary surgery. It is difficult to achieve adequate ligament recovery because of ruptured and altered anatomic structures associated with the surgery undertaken. Obtaining reduction and stabilization is yet another problem. In the literature, although there have been reports of successful results of using graft alone for repair in primary cases, the reliability of this technique is reduced in persistent subluxation cases and there is generally a need for a more rigid fixation. [10] The application of hook plate is one of the alternatives, which can be applied as a means of rigid fixation in persistent subluxation cases, despite complications such as subacromial pain and osteolysis. Reconstruction of the CC ligament with an allograft is important to achieve anatomic recovery and in the stabilization of AC joint reduction. [11],[12],[13],[14],[15],[16] In order to avoid overloading and to maintain appropriate tension of the graft, which is being used in the reconstruction, a hook plate is used to protect the reconstructed ligament during the recovery process by achieving rigid stabilization of the AC joint.
This study presents a new modified surgical technique which was applied to cases of persistent AC joint subluxation following previous treatment by various surgical techniques. In this technique, anatomic AC joint reconstruction was made by the application of anterior tibialis tendon (ATT) autograft, three-way tunnel (two clavicular and one coracoid) and hook plate. The study is aimed to evaluate the post-operative short-term results of patients who underwent this treatment.
| Patients and Methods | | |
Patient characteristics
Approval for this retrospective study was granted by the relevant Institutional Review Board. Informed consent was obtained from all the study participants. A retrospective evaluation was made in our clinic of the results of patients who underwent surgery using ATT allograft and triple tunnel and hook plate technique due to the failure of various surgical techniques, which had been applied to these patients with a diagnosis of AC joint dislocation between 2009 and 2010. Patient data and anamnesis were recorded on the patient file and the clinic routine evaluation form for shoulder pathology. Criteria for inclusion in the study were defined as pre-operative radiological data of Grade 3 or above AC joint damage and less than 3 weeks from the initial trauma to surgery.
Exclusion criteria were previous shoulder joint pathology on either side, patients who had cervical spine pathology of root lesions on the same side or other neurological lesions. The study comprised 11 patients (9 male, 2 female) who met these criteria and were able to be contacted. The mean age of the patients was 32.6 years (range: 26-49 years) and the mean follow-up period was 25.3 months (range: 18-34 months).
The first surgical treatment applied to patients was the Bosworth procedure in three cases and modified Bosworth (screw + anchor) procedure in seven cases. In one case, as failure developed after the first Bosworth procedure, ATT tendon reconstruction was applied in a second operation. A subsequent failure occurred 6 weeks after the second surgery. Data related to the demographics of patients, the initial injury and treatment are shown in [Table 1]. Screw pull-out in the Bosworth procedure and tendon elongation in ATT reconstruction were determined as the causes of failure according to the observations during surgery and from radiographs taken prior to revision [Figure 1].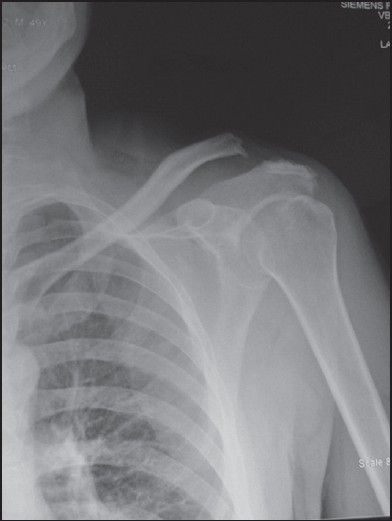 | Figure 1: Anterior-posterior radiograph of the left shoulder of a 36-year-old male patient showing the failed reconstruction of the acromioclavicular (AC) joint with an allograft because of type 5 AC separation
Click here to view |
Surgical technique
To be able to describe the technique, a demonstration was made on a cadaver shoulder, in which the palmaris longus tendon was used to facilitate the procedure. All patients were operated on by two of the authors (Deveci A, Firat A). A horizontal incision was made starting at the AC joint extending 7-10 cm along the anterior surface of the clavicle. The fixation materials (screw, tendon graft etc.), which were used in the first operation were removed. The adhesion sites of the conoid and trapezoid ligaments on the clavicle inferior surface were determined by measurements. The trapezoid ligament site was indicated as 20 mm medial and anterior from the clavicle lateral end; whereas the conoid ligament site was 45 mm medial and posterior from the clavicle lateral end [Figure 2]a.
Using a 5 mm drill, the conoid and trapezoid tunnels were opened in a manner, which did not hinder the plate placement. With the same drill, the coracoid tunnel was opened from the base of the coracoid process in a vertical direction [Figure 2]b. To achieve bone graft integration, 6 mm ATT graft was used to completely fill the inside of the tunnel. The two ends of the ATT graft were sutured using green braided polyester sutures, USP No. 2 (Ethibond® , Ethicon, Sommerville, NJ, USA) with a modified Krakow method. The graft was initially passed through the coracoid process tunnel, then one end of the graft was passed from the trapezoid tunnel and one end from the conoid tunnel from the inferior of the clavicle toward the superior [Figure 2]c and d.
The hook plate was placed with the residual fibrous tissue of the AC joint so as not to close the screw holes of the conoid and trapezoid tunnels [Figure 2]e. After achieving stabilization, as a result of the reduction of the hook plate with the AC joint, the two ends of the graft (trapezoid and conoid) were tightly joined together on the inferior surface of the clavicle [Figure 2]f.
The graft was not tied above the clavicle to avoid graft failure in cases, which would require the removal of the hook plate in the future. Fixation material was not used in the clavicle to avoid the formation of stress fractures of the clavicle. Hook plate and AC joint reduction and fixation was obtained first to avoid excessive loading on the graft. The aim was to provide anatomic recovery, not load-bearing of the graft.
Post-operative management
For 3 weeks post-operatively, the shoulder was immobilized with an abduction sling and only pendular shoulder exercises were allowed. Active elbow and wrist range of motion exercises were started post-operatively. From the 3 rd week to the 6 th week, passive stretching and active assisted shoulder exercises were recommended and after the 6 th week active exercises were started. The exercises were continued until the 12 th week.
Outcome assessment
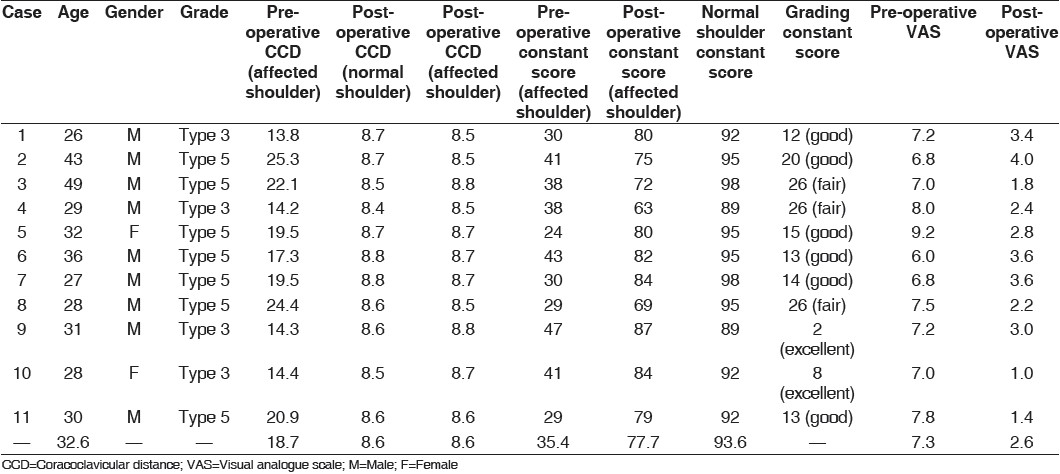
The patient data obtained pre-operatively and at the final follow-up, were examined. Standard plain radiographs, taken pre-operatively and in the post-operative follow-up of both affected and healthy shoulder were examined. The coracoclavicular distance (CCD) and subacromial osteolysis were evaluated on these radiographs. The CCD was calculated by measuring the distance between the coracoid upper limit and the clavicle inferior edge on the standard anterior-posterior (AP) radiograph. Functional results were evaluated with the Constant Shoulder Score and pain with the visual analog score (VAS). In the constant scoring, the difference between the healthy and affected shoulder was defined as >30 poor, 21-30 fair, 11-20 good, <11 excellent. [17],[18] The pre-operative and final follow-up results were compared radiologically and clinically.
| Results | | |
The mean follow-up period was 25.3 months (range: 18-34 months).
Radiological outcomes
No loss of reduction was observed in any case when compared with the healthy shoulder during follow-up. Pre-operative mean CCD was measured as 18.7 mm (mean 13.8-25.3 mm). At the final follow-up, it was observed to have reduced to mean 8.6 mm (range: 8.5-8.8 mm). The healthy shoulder was measured as mean 8.6 mm (range 8.4-9.0 mm). The normal CCD value has been reported in literature as below 11-13 mm. [19] At the final follow-up, 1 case was determined with subacromial osteolysis. No implant failure was observed during follow-up.
Functional outcomes
At the final follow-up, no patient had complaints of pain at a level affecting comfort or function. The mean VAS score reduced from 7.3 (range: 6.8-9.2) to 2.6 (range: 1.0-4.0) and the mean constant score increased from 35.4 (range: 24-47) to 77.7 (63-87). When the constant scores were examined, of the total 24 11 patients, 2 (18.2%) had excellent results, 6 (54.5%) had good 25 results and 3 (27.3%) had fair results [Table 2].
Complications
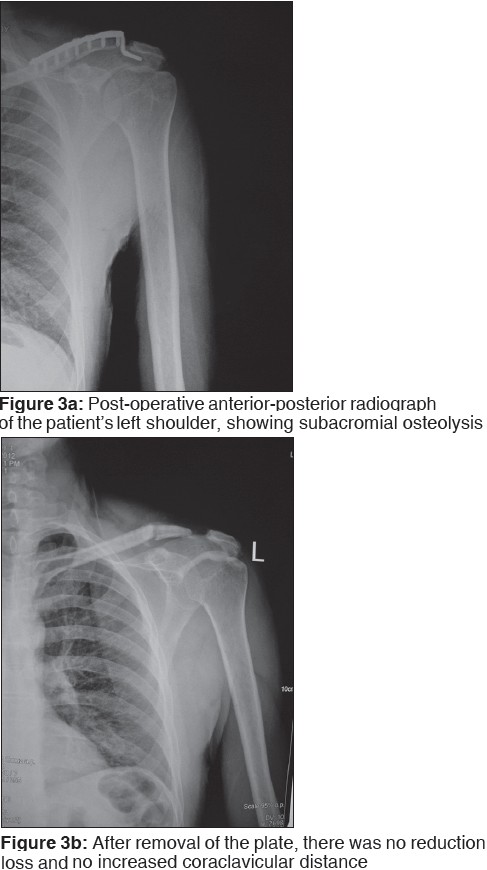
There were no infections in patients who were included in the study. In one patient who had previously undergone surgery twice and to whom revision surgery was applied, complaints developed in the 3 rd post-operative month of pain on the acromion, which increased with movement. Subacromial osteolysis was determined by radiographs. As there was no response to conservative treatment and persistent pain was caused by functional limitation, the hook plate was removed at the 7 th month. After removal of the plate, the pain receded. At the final follow-up, reduction loss and increased CCD were not determined [Figure 3]a and b.
| Discussion | | |
In this study, an evaluation was made of the results of surgery using ATT graft with a triple tunnel and hook plate technique on cases that had undergone various surgical techniques for AC separation and then developed recurrence. With this technique, excellent and good results were obtained in the short term for eight patients. At the final follow-up, the CCD was determined radiologically to be within normal limits in all patients. In the short term, except for one patient, a pain-free and functional shoulder was obtained in all patients. After removal of the hook plate in one patient, a functional shoulder was obtained.
The limitations of this study are that the number of cases was low the follow-up period was short and there was no group for comparison.
Revision cases are problematic in respect of both the technical difficulties of surgical treatment and the results. In these cases, anatomic recovery of the CC ligament may not be possible depending on the effects of previous surgery and the passing of a long time period. Therefore, in revision cases it must be aimed to have recovery with anatomic reconstruction and strong stabilization. In a study by Tauber et al. revision surgery was applied with autogenous semitendinosus graft to 12 patients with AC joint dislocation who developed failure after primary surgery. In that study, after passing the graft under the coracoid process, the two ends were tied above the clavicle by passing through two tunnels in the clavicle openings. To protect the reconstruction and increase stability, the Bosworth procedure was added. [20] LaPrade and Hilger achieved successful results using semitendinosus graft on two cases of Grade 5 AC dislocation in whom recurrence developed following previously applied Weaver-Dunn procedure. [21]
In revision cases, it is extremely difficult to sustain reduction because of muscle retraction and scar tissue with AC joint reduction. In this situation, hook plate is an appropriate fixation technique in terms of providing rigid fixation and preventing fractures developing in the coracoid and clavicle associated with the tendon graft by transferring distraction strength to the acromion. Although it provides a strong and rigid fixation, the plate needs to be removed in cases of subacromial osteolysis and persistent pain. [11],[15],[16],[22] It has also been reported that when the plate has been applied alone in primary cases, even 1 year after plate removal, there is the possibility of recurrence in 12% of cases. [23] Therefore, to achieve anatomic ligament recovery in revision cases, it should be applied together with tendon reconstruction.
Hook plate and suture-button technique is currently widely used as a stable fixation technique. Although, the use of the button technique has become increasingly widespread, there are complications such as suture breakage, the breaking free of the button inside the coracoid and the development of coracoid fractures. [9],[24] As all patients in the current study had undergone Bosworth and its modified techniques in the initial operations, the application of the button technique would have been difficult because of the screws, which were removed from the clavicle and coracoid sites. It was thought that coracoid fracture or button failure could have developed.
In the current study, the graft passed through a triple tunnel. For integration of the ATT graft with bone tissue and to act functionally, the graft was passed through the conoid and trapezoid tunnels in the clavicle and through the coracoid tunnel. This was because the aim was to have anatomic reconstruction at the CC ligament adhesion sites. Passing the graft through the coracoid bone provides vertical stability in addition to horizontal stability. [25] At the same time, integration between the graft and the coracoid bone tunnel will be better than in techniques where the graft passes below the coracoid.
Without fixing both ends of the graft to the clavicle, they were tied to each other below the clavicle. Thus, it was aimed to facilitate integration between the graft and the bone tunnel and to reduce the effect of deforming forces on the graft by means of the hook plate. In addition, as fixation materials were not used for the graft on the clavicle, fracture development via the tunnel was avoided.
Costic et al. compared anatomic restoration using semitendinosus tendon with intact CC ligament. [26] Although the reconstruction resulted in a significant development in biomechanic terms, properties of strength of up to 40% of the normal CC ligament and maximum resistance of up to 75% were shown. In this cadaver study of anatomic reconstruction with semitendinosus graft, reasons for graft failure were clavicular fracture, impairment of the graft integrity and fractures forming in the coracoid process. Lee et al. also showed impairment of the graft internal integrity and coracoid layer fractures to be the reason for failure in studies of anatomic reconstruction. [4]
In applications of anatomic reconstruction with ATT and semitendinosus graft by Turman et al. tendons were passed under the coracoid and the two ends were fixed with interference screws to the holes in the clavicle. At the final follow-up, fractures at the screw sites and cases of recurrence were determined. [27] When the complications resulting from tendon graft applications were examined, it was thought that it is necessary to use a method of providing anatomic recovery rather than stabilization of the tendon. To relieve the stress on the reconstructed tendon, separate fixation material should be used.
| Conclusion | | |
It can be seen that this newly described reconstruction technique has successful short-term results as an anatomic method and can be used effectively in revision cases. However, there is a need for further biomechanical and long-term clinical studies to make comparisons with other techniques.
| Acknowledgements | | |
No benefits in any form have been received or will be received from a commercial party related directly or indirectly to the subject of this article.
| References | | |
| 1. | Rios CG, Arciero RA, Mazzocca AD. Anatomy of the clavicle and coracoid process for reconstruction of the coracoclavicular ligaments. Am J Sports Med 2007;35:811-7. 
[PUBMED] |
| 2. | Fukuda K, Craig EV, An KN, Cofield RH, Chao EY. Biomechanical study of the ligamentous system of the acromioclavicular joint. J Bone Joint Surg Am 1986;68:434-40.
[PUBMED] |
| 3. | Jiang C, Wang M, Rong G. Proximally based conjoined tendon transfer for coracoclavicular reconstruction in the treatment of acromioclavicular dislocation. Surgical technique. J Bone Joint Surg Am 2008;90 Suppl 2 Pt 2:299-308.
[PUBMED] |
| 4. | Lee SJ, Nicholas SJ, Akizuki KH, McHugh MP, Kremenic IJ, Ben-Avi S. Reconstruction of the coracoclavicular ligaments with tendon grafts: A comparative biomechanical study. Am J Sports Med 2003;31:648-55.
[PUBMED] |
| 5. | Tauber M, Gordon K, Koller H, Fox M, Resch H. Semitendinosus tendon graft versus a modified Weaver-Dunn procedure for acromioclavicular joint reconstruction in chronic cases: A prospective comparative study. Am J Sports Med 2009;37:181-90.
[PUBMED] |
| 6. | Bosworth BM. Complete acromioclavicular dislocation. N Engl J Med 1949;241:221-5.
[PUBMED] |
| 7. | Weaver JK, Dunn HK. Treatment of acromioclavicular injuries, especially complete acromioclavicular separation. J Bone Joint Surg Am 1972;54:1187-94.
[PUBMED] |
| 8. | Kirchhoff C, Braunstein V, Buhmann S, Mutschler W, Biberthaler P. A salvage procedure for failed Weaver-Dunn reconstruction. Oper Orthop Traumatol 2008;20:176-81.
[PUBMED] |
| 9. | Geaney LE, Miller MD, Ticker JB, Romeo AA, Guerra JJ, Bollier M, et al. Management of the failed AC joint reconstruction: Causation and treatment. Sports Med Arthrosc 2010;18:167-72.
[PUBMED] |
| 10. | Weinstein DM, McCann PD, McIlveen SJ, Flatow EL, Bigliani LU. Surgical treatment of complete acromioclavicular dislocations. Am J Sports Med 1995;23:324-31.
[PUBMED] |
| 11. | McConnell AJ, Yoo DJ, Zdero R, Schemitsch EH, McKee MD. Methods of operative fixation of the acromio-clavicular joint: A biomechanical comparison. J Orthop Trauma 2007;21:248-53.
[PUBMED] |
| 12. | Ejam S, Lind T, Falkenberg B. Surgical treatment of acute and chronic acromioclavicular dislocation tossy type III and V using the hook plate. Acta Orthop Belg 2008;74:441-5.
[PUBMED] |
| 13. | Faraj AA, Ketzer B. The use of a hook-plate in the management of acromioclavicular injuries. Report of ten cases. Acta Orthop Belg 2001;67:448-51.
[PUBMED] |
| 14. | Habernek H, Weinstabl R, Schmid L, Fialka C. A crook plate for treatment of acromioclavicular joint separation: Indication, technique, and results after one year. J Trauma 1993;35:893-901.
[PUBMED] |
| 15. | Koukakis A, Manouras A, Apostolou CD, Lagoudianakis E, Papadima A, Triantafillou C, et al. Results using the AO hook plate for dislocations of the acromioclavicular joint. Expert Rev Med Devices 2008;5:567-72.
[PUBMED] |
| 16. | Sim E, Schwarz N, Höcker K, Berzlanovich A. Repair of complete acromioclavicular separations using the acromioclavicular-hook plate. Clin Orthop Relat Res 1995;314:134-42.
|
| 17. | Constant CR, Murley AH. A clinical method of functional assessment of the shoulder. Clin Orthop Relat Res 1987;214:160-4.
[PUBMED] |
| 18. | Fabre T, Piton C, Leclouerec G, Gervais-Delion F, Durandeau A. Entrapment of the suprascapular nerve. J Bone Joint Surg Br 1999;81:414-9.
[PUBMED] |
| 19. | Rogers LF. Radiology of Skeletal Trauma. 3 rd ed. New York: Churchill Livingstone; 2002. p. 602.
|
| 20. | Tauber M, Eppel M, Resch H. Acromioclavicular reconstruction using autogenous semitendinosus tendon graft: Results of revision surgery in chronic cases. J Shoulder Elbow Surg 2007;16:429-33.
[PUBMED] |
| 21. | LaPrade RF, Hilger B. Coracoclavicular ligament reconstruction using a semitendinosus graft for failed acromioclavicular separation surgery. Arthroscopy 2005;21:1277.
[PUBMED] |
| 22. | Nadarajah R, Mahaluxmivala J, Amin A, Goodier DW. Clavicular hook-plate: Complications of retaining the implant. Injury 2005;36:681-3.
[PUBMED] |
| 23. | Di Francesco A, Zoccali C, Colafarina O, Pizzoferrato R, Flamini S. The use of hook plate in type III and V acromio-clavicular Rockwood dislocations: Clinical and radiological midterm results and MRI evaluation in 42 patients. Injury 2012;43:147-52.
[PUBMED] |
| 24. | Beitzel K, Obopilwe E, Chowaniec DM, Niver GE, Nowak MD, Hanypsiak BT, et al. Biomechanical comparison of arthroscopic repairs for acromioclavicular joint instability: Suture button systems without biological augmentation. Am J Sports Med 2011;39:2218-25.
[PUBMED] |
| 25. | Yoo YS, Tsai AG, Ranawat AS, Bansal M, Fu FH, Rodosky MW, et al. A biomechanical analysis of the native coracoclavicular ligaments and their influence on a new reconstruction using a coracoid tunnel and free tendon graft. Arthroscopy 2010;26:1153-61.
[PUBMED] |
| 26. | Costic RS, Labriola JE, Rodosky MW, Debski RE. Biomechanical rationale for development of anatomical reconstructions of coracoclavicular ligaments after complete acromioclavicular joint dislocations. Am J Sports Med 2004;32:1929-36.
[PUBMED] |
| 27. | Turman KA, Miller CD, Miller MD. Clavicular fractures following coracoclavicular ligament reconstruction with tendon graft: A report of three cases. J Bone Joint Surg Am 2010;92:1526-32.
[PUBMED] |
[Figure 1], [Figure 2], [Figure 3]
[Table 1], [Table 2]
| This article has been cited by | | 1 |
Biologic Solutions to anatomic AC joint reconstruction |
|
| Gregory L. Cvetanovich,Scott Trenhaile,Rachel M. Frank | | Operative Techniques in Sports Medicine. 2014; | | [Pubmed] | [DOI] | |
|
|
|
|