| |


 |
| Year : 2013 | Volume
: 7
| Issue : 4 | Page : 139-142 |
|
|
|
|
|
SURGICAL TECHNIQUE Lateral releases of the subscapularis tendon
Ian K.Y. Lo1, Atiba A Nelson1, Stephen S Burkhart2
1 Department of Surgery, The University of Calgary, Alberta, Canada
2 Department of Orthopaedic Surgery, University of Texas Health Science Center at San Antonio, San Antonio, Texas, USA
Correspondence Address:
Ian K.Y. Lo
Department of Surgery, The University of Calgary, 3330 Hospital Drive, NW, Calgary, AB, T2N 1N4
Canada
 Source of Support: None, Conflict of Interest: None
DOI: 10.4103/0973-6042.123520

|
|
|
|
| Date of Web Publication | 24-Dec-2013 |
 Abstract Abstract | | |
The technique of arthroscopic subscapularis repair continues to evolve. A three-sided subscapularis release (e.g. anterior, posterior, superior) is commonly advocated for improving tendon excursion to bone. However, a lateral release is commonly required as well, particularly for full thickness, upper subscapularis tears and full thickness, complete subscapularis tears. We describe the techniques to identify and release the lateral subscapularis border, which aids in the completion of other releases.
Keywords: Lateral release, release, subscapularis repair, subscapularis, three-sided subscapularis release
How to cite this article:
Lo IK, Nelson AA, Burkhart SS. Lateral releases of the subscapularis tendon. Int J Shoulder Surg 2013;7:139-42 |
| Introduction | |  |
Subscapularis tears represent a spectrum of disease from partial articular surface tears to full thickness, complete tears with retraction and scarring. [1],[2] In cases with significant retraction, advanced releases may be required for improving tendon excursion and obtaining a tension free repair to bone.
We have previously described a three-sided release of the subscapularis tendon in a step-wise fashion progressing superiorly, anteriorly and then posteriorly. [2],[3],[4],[5],[6] Inferior release is generally not necessary and avoids risking the axillary nerve.
However, an additional lateral release of the subscapularis tendon is commonly required. This release must be commonly performed since it identifies the lateral border of the subscapularis and facilitates access of instruments from the anterosuperolateral portal to the anterior aspect of the subscapularis, the subcoracoid space, and the lesser tuberosity.
In the following technical note we described the two most common scenarios where a lateral release is required: An upper subscapularis tears and a retracted subscapularis tear which has become scarred to the inner deltoid fascia and anterior structures.
| Surgical Technique | | |
The patient is placed in the lateral decubitus position and a standard posterior glenohumeral portal is created. The view to the subscapularis tendon is augmented by internal rotation, abduction and posterior translation in addition to using a 70 o arthroscope. There are two scenarios in which a lateral release maybe required: The upper subscapularis tear and the retracted complete subscapularis tears with scarring to the inner deltoid fascia.
The first scenario is the upper subscapularis tear and is the more common tear pattern. Since even upper subscapularis tears lead to disruption of the medial sling, medial subluxation of the biceps tendon commonly occurs splitting the subscapularis into a deep lower portion and a more superficial upper portion [Figure 1].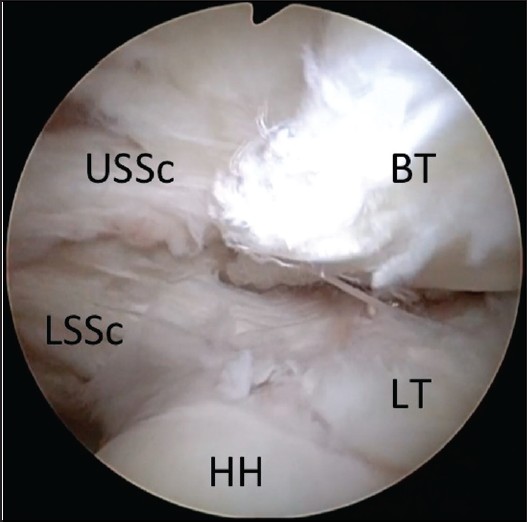 | Figure 1: Arthroscopic view of a right shoulder through a posterior glenohumeral portal demonstrating an upper subscapularis tear with subluxation of the biceps between the proximal, superficial upper subscapularis and the distal, deep lower subscapularis (BT, biceps tendon; HH, humeral head; LT, lesser tuberosity; USSc, upper subscapularis; LSSc, lower subscapularis)
Click here to view |
A standard anterosuperolateral portal is created 1-2 cms lateral to the anterolateral corner of the acromion and parallel to the lesser tuberosity. In this scenario the superficial upper subscapularis component remains in continuity with the transverse ligament of the bicipital groove [Figure 2]a. It is this extension of the subscapularis which prevents access to the lesser tuberosity and bone bed.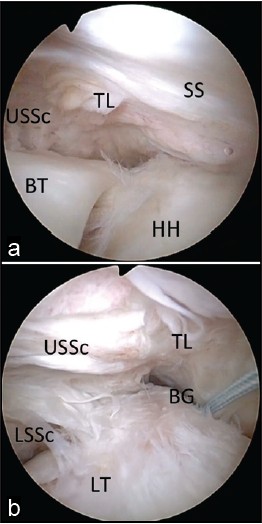 | Figure 2: Arthroscopic view of a right shoulder through a posterior glenohumeral portal demonstrating an upper subscapularis tear with extension of the lateral border to the transverse ligament and supraspinatus tendon. The transverse ligament extends laterally draping over the long head of the biceps tendon and the bicipital groove. (a) Prior to biceps tenotomy. (b) Following biceps tenotomy. Sutures have been placed in the residual end of the long head of the biceps, which has been allowed to retract distally in the arm. (BG, bicipital groove; BT, biceps tendon; HH, humeral head; LT lesser tuberosity; USSc, upper subscapularis; LSSc, lower subscapularis; SS, supraspinatus; TL, transverse ligament)
Click here to view |
The biceps tendon is then tagged and released from its origin at the superior labrum. Once the biceps tendon has been released the extension to the transverse ligament is more readily apparent [Figure 2]b. The comma sign is then identified [7] and the biceps tendon pulled laterally or allowed to retract distally down the arm. The release is then performed using a combination of electrocautery and punches introduced through the anterosuperolateral portal. The location of the lateral release is at the lateral aspect of the lesser tuberosity along the medial aspect of the bicipital groove [Figure 3]a. The release begins superiorly and extends inferior splitting the subscapularis tendon away from the transverse ligament [Figure 3]b.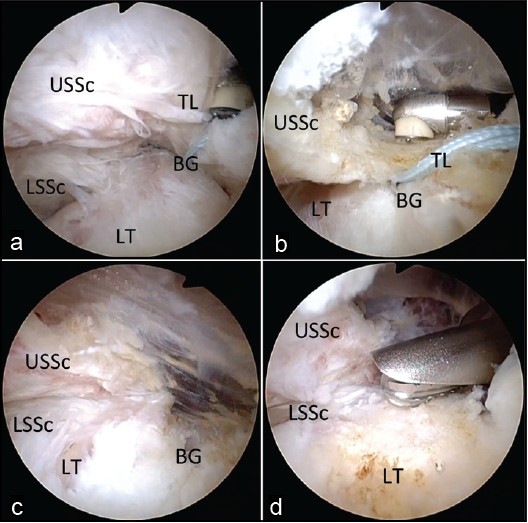 | Figure 3: Arthroscopic view of a right shoulder through a posterior glenohumeral portal demonstrating the lateral release. (a) The lateral border of the upper subscapularis is defined by releasing the lateral extension of the transverse ligament. The release begins at the upper border of the subscapularis. (b) The release continues inferiorly separating the transverse ligament from the upper subscapularis and exposing the bicipital groove. (c) The completed release exposes the bicipital groove completely and the distal deep intact lower subscapularis. (d) With the lateral release completed, the entire upper
lesser tuberosity may now be accessed with ease for eventual repair. (BG, bicipital groove; LT, lesser tuberosity; USSc, upper subscapularis; LSSc, lower subscapularis; TL, transverse ligament)
Click here to view |
The release continues until the deep, distal intact portion of the subscapularis tendon and the bicipital groove is revealed [Figure 3]c. With the lateral release completed this defines the lateral margin of the subscapularis tendon, which allows for access to the lesser tuberosity [Figure 3]d. Further releases may now be performed as required with definitive fixation to bone.
In the second scenario, a complete subscapularis tendon has retracted and scarred to the inner deltoid fascia. In this scenario, the long head of the biceps tendon is again commonly dislocated medially. An anterosuperolateral portal is created and the long head of the biceps is tagged and released.
However, because of scarring the lateral margin of the subscapularis tendon is obscured. In this case, the lateral margin becomes scarred to the inner deltoid fascia laterally (e.g. lateral leader) and also the conjoint tendon anteriorly [Figure 4]. This prevents access to the anterior aspect of the subscapularis tendon, and the subcoracoid space. Furthermore, this scarring prevents passage of a traction stitch to the comma sign, usually the first step prior to beginning a three sided subscapularis release.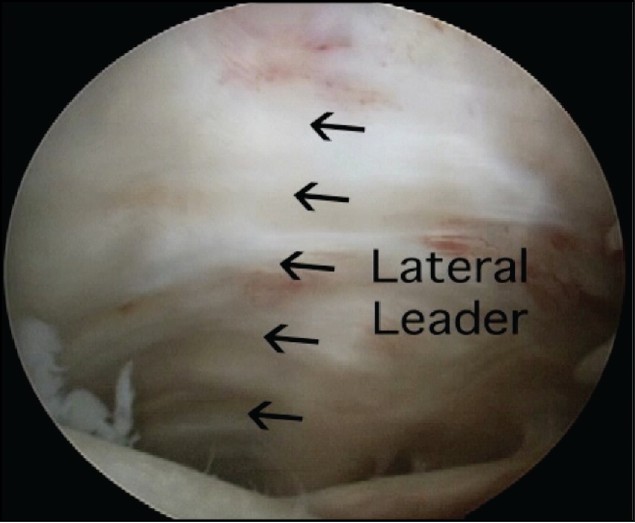 | Figure 4: Arthroscopic view of a left shoulder through a posterior glenohumeral portal demonstrating a tear of the subscapularis tendon with the lateral border scarred to the inner deltoid fascia (i.e. lateral leader)
Click here to view |
When a complete subscapularis tears has scarred to the inner deltoid fascia the key is the comma sign. This is identified and traction is applied to the medial aspect of the comma sign. This not only draws the superior border of the subscapularis laterally but also defines the lateral border as well [Figure 5].
The lateral release is performed using a combination of electrocautery (Arthrocare, Inc., Naples, FL) and punches; introduced through an anterosuperolateral portal. It is easiest to start the lateral release at the same level of the superior margin of the subscapularis tendon [Figure 6]a. Care is taken as the lateral margin of the subscapularis is dissected off the deltoid fascia laterally [Figure 6]b and the conjoint tendon anteriorly [Figure 6]c. The release is continued inferiorly until the lateral margin of the subscapularis is freed and also superiorly releases the comma sign from the inner deltoid fascia. With the lateral margin free, the subcoracoid space can now be accessed and a traction stitch can be applied to its lateral margin [Figure 7].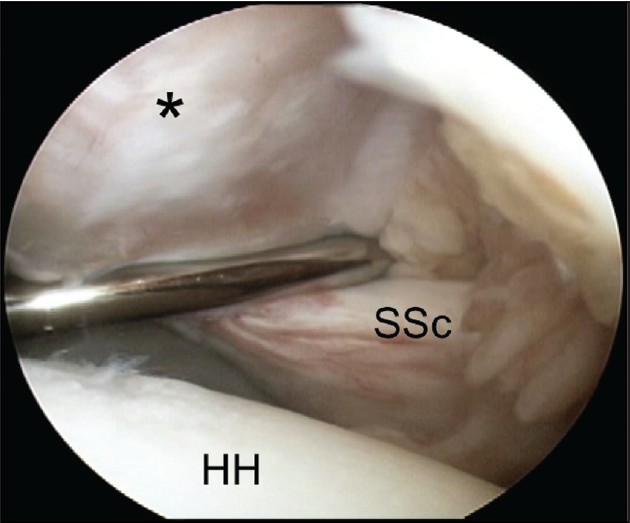 | Figure 5: Arthroscopic view of a left shoulder through a posterior glenohumeral portal demonstrating traction on the comma sign (*) defining the superior and lateral borders of the subscapularis tendon (SSc). (HH, humeral head)
Click here to view |
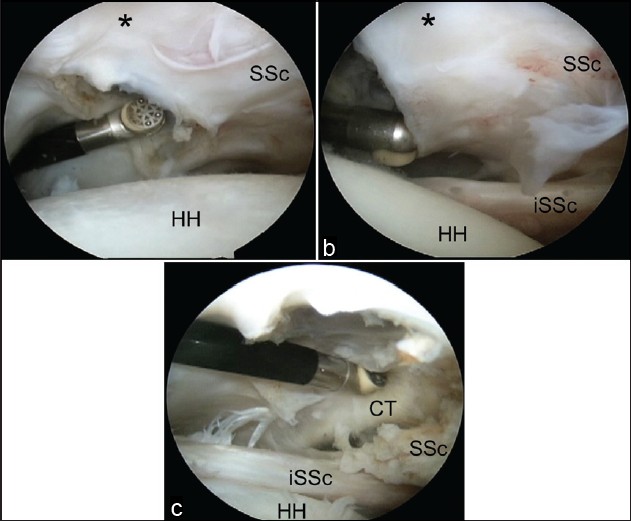 | Figure 6: Arthroscopic view of a left shoulder through a posterior glenohumeral portal. (a) The initial release is started adjacent to the upper border of the subscapularis tendon (SSc) and the comma sign (*). (b) The release is continued inferiorly separating the subscapularis from the inner deltoid fascia and the conjoint tendon. (c) (CT, conjoint tendon; G, glenoid; HH, humeral head; iSSc, intact lower subscapularis)
Click here to view |
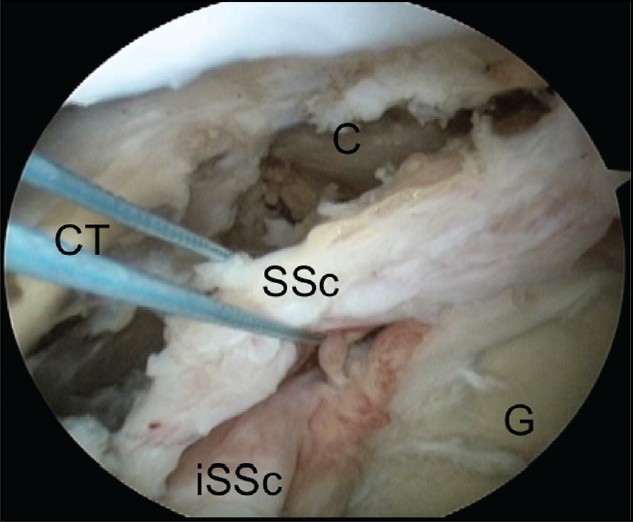 | Figure 7: Arthroscopic view of a left shoulder through an anterosuperolateral portal demonstrating completed release of the
lateral border of the subscapularis allowing access to the subcoracoid space. (C, coracoid; G, glenoid; SSc, torn subscapularis; iSSc, intact lower subscapularis)
Click here to view |
With the traction stitch applied, the three-sided release of the subscapularis tendon can then be performed improving tendon excursion to bone. Standard suture anchor based techniques can then be utilized for definitive tendon fixation to bone.
| Discussion | | |
Arthroscopic subscapularis repair remains one of the more challenging aspects of rotator cuff surgery. [4],[8],[9] This is not only related to difficulties in visualization and the sometimes, awkward angle of approach but also due to the advanced releases required for tension free tendon fixation to bone. While the three-sided release has previously been described for improving tendon excursion to bone, a lateral release is commonly required as well.
In the first case of an upper subscapularis tear, the subscapularis tendon is split by the biceps tendon. It is the upper subscapularis tendon, which is superficial to the biceps that is torn off the bone but remains in continuity with the transverse ligament. This can also sometimes occur with complete subscapularis tendon tears where the entire subscapularis tendon remains in continuity with the transverse ligament. These tendon tears are commonly missed during open approaches where it may appear the subscapularis remains intact.
This extension into the transverse ligament however prevents access to the lesser tuberosity. While a transtendon repair could be performed, it is easier to release the subscapularis tendon from the transverse ligament so that standard suture anchor-based techniques may be performed. Furthermore, the tissue extension may be utilized during repair and incorporated into a double row repair. Care must be taken, however, to ensure that the thicker more medial tendon tissue is fixated as well. A double row repair is commonly possible since upper subscapularis tendon tears are usually minimally retracted and do not require extensive three-sided releases.
The second scenario, however, usually requires an extensive three-sided release of the subscapularis tendon. These tears are usually chronic in nature and tissue quality may be poor as well. In cases of severe retraction, the coracoid insertion of the coracoacromial ligament or the conjoint tendon may be confused with the subscapularis.
The key then is again the comma sign, which will identify the lateral and superior portions of the subscapularis tendon. However, prior to performing a three-sided release the lateral aspect of the subscapularis must be defined to allow passage of a subscapularis traction stitch. Releasing the lateral border will allow access to the anterior aspect of the subscapularis so that subsequent anterior release and subcoracoid decompression may be performed. Furthermore, by defining the lateral border, the tissue lateral to this (i.e. bursal extension) may be debrided to improve visualization. Due to severe retraction and scarring, a double row repair is commonly not possible and single row or modified double row techniques are utilized. [10]
In conclusion, in addition to the three-sided subscapularis release, a lateral release of the subscapularis tendon may be required. This release is required in upper subscapularis tears that extend to the transverse ligament and chronic retracted tears where the lateral border is scarred to the inner deltoid fascia and conjoint tendon.
| References | | |
| 1. | Lo IK, Burkhart SS. The etiology and assessment of subscapularis tendon tears: A case for subcoracoid impingement, the roller-wringer effect, and TUFF lesions of the subscapularis. Arthroscopy 2003;19:1142-50. 
[PUBMED] |
| 2. | Lo IK, Burkhart SS. The interval slide in continuity: A method of mobilizing the anterosuperior rotator cuff without disrupting the tear margins. Arthroscopy 2004;20:435-41.
[PUBMED] |
| 3. | Burkhart SS, Lo IK. Arthroscopic rotator cuff repair. J Am Acad Orthop Surg 2006;14:333-46.
[PUBMED] |
| 4. | Burkhart SS, Tehrany AM. Arthroscopy subscapularis tendon repair: Technique and preliminary results. Arthroscopy 2002;18:454-63.
[PUBMED] |
| 5. | Burkhart SS, Brady PC. Arthroscopic subscapularis repair: Surgical tips and pearls from A to Z. Arthroscopy 2006;22:1014-27.
[PUBMED] |
| 6. | Lo IK, Burkhart SS. Subscapularis tears: Arthroscopic repair of the forgotten rotator cuff tendon. Tech Shoulder Elbow Surg 2002;3:282-91.
|
| 7. | Lo IK, Burkhart SS. The comma sign: An arthroscopic guide to the torn subscapularis tendon. Arthroscopy 2003;19:334-7.
[PUBMED] |
| 8. | Adams CR, Schoolfield JD, Burkhart SS. The results of arthroscopic subscapularis tendon repairs. Arthroscopy 2008;24:1381-9.
[PUBMED] |
| 9. | Denard PJ, Jiwani AZ, Ladermann A, Burkhart SS. Long-term outcome of a consecutive series of subscapularis tendon tears repaired arthroscopically. Arthroscopy 2012;28:1587-91.
|
| 10. | Denard PJ, Ladermann A, Burkhart SS. Double-row fixation of upper a subscapularis tears with single suture anchor. Arthroscopy 2011;27:1142-9.
|
[Figure 1], [Figure 2], [Figure 3], [Figure 4], [Figure 5], [Figure 6], [Figure 7]
|













