| |


 |
| Year : 2014 | Volume
: 8
| Issue : 2 | Page : 61-64 |
|
|
|
|
|
CASE REPORT Myositis ossificans of the humeral insertion of pectoralis major
Viga Mogere, David S. K. Thyagarajan, K Julia Fairbairn, Angus Wallace
Nottingham Shoulder and Elbow Unit, City Hospital, Nottingham University Hospital National Health Service Trust, Nottingham, United Kingdom
Correspondence Address:
David S. K. Thyagarajan
Nottingham Shoulder and Elbow Unit, City Hospital, Nottingham University Hospital National Health Service Trust, Nottingham
United Kingdom
 Source of Support: None, Conflict of Interest: None
DOI: 10.4103/0973-6042.137531
 |
|
|
|
| Date of Web Publication | 24-Jul-2014 |
 Abstract Abstract | | |
We report on a rare case of myositis ossificans of the humeral insertion of pectoralis major muscle following a single episode of trauma which, to our knowledge, has not previously been documented.
Keywords: Myositis ossificans, proximal humerus, pectoralis major
How to cite this article:
Mogere V, Thyagarajan DS, Fairbairn K J, Wallace A. Myositis ossificans of the humeral insertion of pectoralis major. Int J Shoulder Surg 2014;8:61-4 |
[TAG:2]INTRODUCTION [/TAG:2]
Myositis ossificans has been defined as a benign solitary self-limiting ossifying soft tissue mass which typically occurs within skeletal muscle. [1] Sixty to seventy-five percent of reported cases of myositis ossificans occur as a result of trauma. [2],[3] Some forms of this disease are known to occur without preceding trauma and are referred to as pseudo-malignant myositis ossificans, which are benign, but due to the fast rate at which they sometimes proliferate have been mistaken for malignant lesions. [4] Nontraumatic cases are commonly seen among patients with paraplegia, polio, tetanus, and burns. [5]
Myositis ossificans has a male preponderance [4] and is seen more commonly in young adults less than 30 years of age with a peak occurrence between 11-20 years. It tends to develop over the shaft of long bones which are areas where the muscles are prone to direct trauma, and is seen commonly in vigorous sports such as football. [6] The peak incidence of myositis ossificans is noted at 4-12 weeks following an injury and can occur up to 5 months following the trauma. An even later onset has been reported but is very rare. The two most commonly affected anatomical sites are the anterior thigh (quadriceps femoris muscle) and the arm (brachialis muscle), [7],[8] with an incidence of 51.9-56% in the femur, and 12-25% in the humerus. [3],[6]
The pectoralis major muscle is a large fan-shaped anterior thoracoappendicular muscle. It originates from the medial end of the clavicle, sternum, the second to sixth ribs and the external oblique muscle fascia. It is generally divided into two heads (clavicular and sternocostal) though some authors have classified it into three segments [9] all of which insert as one tendon into the lateral lip of the bicipital groove. It is a powerful internal rotator, flexor, and adductor of the humerus. [10] Due to these actions, this muscle is commonly injured in weight lifters, notably during bench press exercise, [11] which tends to occur during powerful eccentric contractions. [12]
Here we report on a rare case of myositis ossificans of the humeral insertion of pectoralis major muscle following a single episode of trauma which, to our knowledge, has not previously been documented.
| Case report | |  |
A 16-year-old male patient presented with a history of left shoulder pain after an acute single episode of trauma 5 months prior to his clinic visit. This occurred during his gym training session while doing 'pectoral-fly's' - a chest exercise done when lying supine, with the shoulders in 90 degrees of forward flexion, and using dumbbell weights gradually abducting the shoulder, and thus eccentrically working the pectoralis muscle. During one of the repetitions, he lost control of the weight in the left arm which underwent a forceful abduction injury. He heard a 'snapping' sound followed immediately by pain in the anterior shoulder. He reported an abrupt onset swelling and bruising. He visited the emergency department of his local hospital, was assessed, and then discharged home with a diagnosis of a soft tissue injury. No treatment was recommended. The pain subsided gradually but not completely over the next few months and the injury was not a hindrance to him carrying out his daily activities; however, due to the persistent nature of the pain he sought treatment in our clinic.
His past medical history and general examination were unremarkable. Examination of his left shoulder revealed a hard bony non tender mass in the anteromedial aspect of the limb over the pectoralis major muscle insertion. The rest of the shoulder examination was otherwise normal.
Initial X-ray and MR images were taken 3.5 months after the injury at an outside institution. The X-ray demonstrated an ossifying mass in the upper third of the arm within the pectoralis major muscle that coalesced with the underlying humerus [Figure 1]. The MRI showed some zoning phenomenon especially on the coronal T1 scan [Figure 2] and the water sensitive sequences also showed some swelling and high signal around the mass. A second series of imaging X-ray [Figure 3]a and b and CT scan [Figure 4] at 5 months showed further maturation especially of the outer compact bone of the mass with resolution of the surrounding soft tissue swelling at the insertion of the pectoralis major muscle.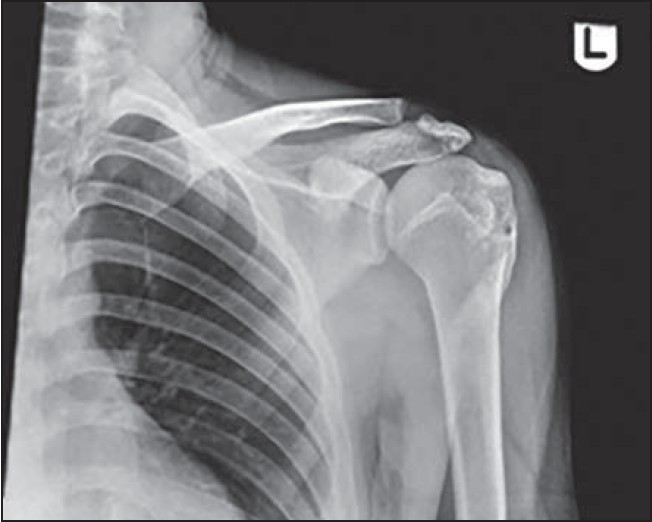 | Figure 1: AP X-ray of shoulder at 3.5 months showing an ossifying mass coalescing with the proximal humerus
Click here to view |
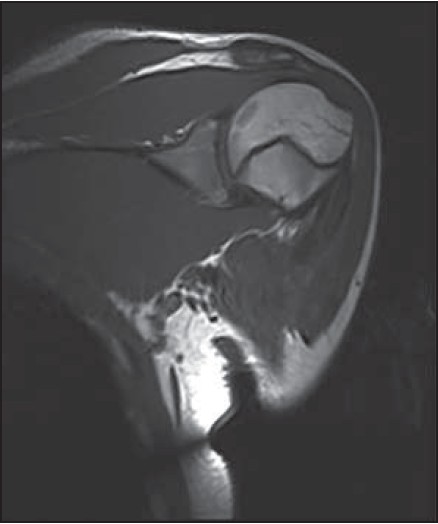 | Figure 2: Coronal section MRI T1 at 3.5 months showing the zoning phenomenon
Click here to view |
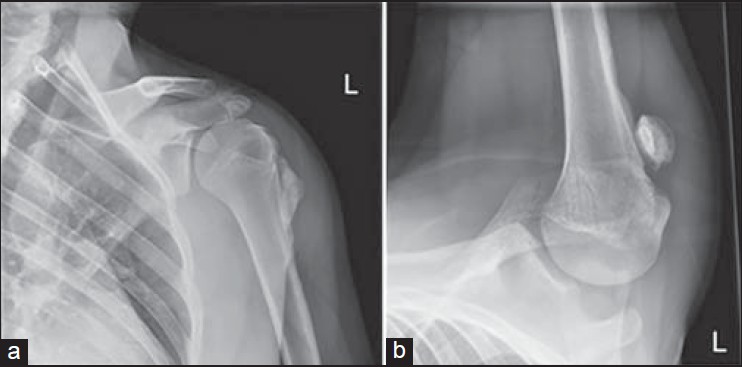 | Figure 3: (A and B) AP and axial X-ray of shoulder at 5 months showing maturation of the ossifying mass
Click here to view |
 | Figure 4: 3D CT scan of shoulder at 5 months demonstrating a fully mature myositis ossificans
Click here to view |
A diagnosis of myositis ossificans was made. A decision was made to manage the patient conservatively.
| Discussion | | |
Myositis ossificans is an inflammatory pseudotumor of the skeletal muscle and can easily be mistaken clinically and even histologically for a malignant soft tissue tumor. The exact etiology of the condition remains unclear. Myositis ossificans can develop secondary to muscular trauma. However, in most cases no causative factor can be identified. [13]
There is a gender predilection albeit circumstantial, as males are generally more prone to trauma than females. [4] However, cases of one of the variants of the lesion, myositis ossificans progressiva though rare, have been reported more among females than males but the reasons for this are yet unknown. [3] Perhaps genetics has a role to play in the etiology as is seen in cases of 'stone man disease', a rare hereditary connective tissue disorder in which certain individuals are prone to undergoing spontaneous heterotropic ossification in skeletal muscle, tendons, and ligaments. [14]
After a significant traumatic injury to a muscle, bleeding occurs into or around it. The resulting hematoma undergoes organization and mineralization from the outside in. This reflects the 'zoning phenomenon' characteristically seen with myositis ossificans in which three distinct zones have been classified. [1] The central zone is made up of fibroblasts and necrotic muscle; the middle zone has osteoblasts and immature bone and the most peripheral zone is formed of mature trabeculoid distinct from the surrounding tissue. This shows on films as a well-circumscribed mass with an outer layer of ossification and a lucent centre. Depending on the level of maturation of the lesion, all three zones might not always be clearly demonstrated radiographically. Calcification of the lesion is seen as early as 11 days up to 4 weeks. Ossification and formation of a sharp circumscribed mass occur at 4-8 weeks, and the lesion reaches full maturity after 5 months. [1]
It is interesting that not all cases of soft tissue trauma with hematoma development progress into myositis ossificans, and conversely that there are non traumatic forms of the same. A pertinent question to ask is what then triggers the formation of bone in non ossifying tissue in some individuals and not others?
Several theories have been explored to try and explain why myositis ossificans occurs, one of which states after an injury to a muscle, the disruption of small capillaries, shearing of muscle fibers, and the detachment of periosteal cells is what is thought to eventually stimulate the formation of extra-osseous bone within the skeletal muscle. [3] This is likely to be the reason for the occurrence of myositis ossificans in this case report. Another proposed mechanism by which myositis ossificans develops is thought to be as a consequence of the healing process after a single or repeated episodes of trauma that tends to develop more readily after intramuscular bleeds than intermuscular ones. [7] The cardinal features of inflammation, rubor, tumor, color, dolor are considered a prerequisite to developing myositis ossificans [6] though some authors argue that this is not strictly the case. [4] The evidence is controversial and inconclusive making it difficult to ascertain the exact cause. It might probably be due to a combination of some, if not all the above factors.
A detailed history and thorough clinical examination when treating all patients cannot be emphasized enough. What is of particular interest here, however, is the radiological appearance of myositis ossificans which is typically characteristic of the lesion. We therefore take into significant consideration the importance of good roentgenographic studies with timely follow-up when making a diagnosis of myositis ossificans. The literature on the subject matter is limited, nonetheless, the exact cause has yet to be elucidated and further in depth analysis of myositis ossificans cases might shed light on this confounding phenomenon.
Standard radiographs often appear normal during the early stages of myositis ossificans but can show de novo pathognomonic ossification surrounding a clear central area at a later stage. [2] Some reports suggest ultrasound to be the most sensitive imaging modality to detect early zone phenomenon in myositis ossificans. [15] MRI may show the so-called zone phenomenon even before the ossification appears. CT scans are more sensitive than radiography for detecting ossification and may also show a central fatty metaplastic area. [16]
Histological section of a mature lesion shows a central myxoid matrix with fibroblasts (pseudo-fibrosarcomatous zone) surrounded by mature bone at the periphery of the lesion. In the acute phase of myositis ossificans which lasts for about one week, histology of the lesion shows proliferation composed of mesenchymal cells secreting a myxoid matrix as well as fibroblasts exhibiting numerous mitoses, which gives it a pseudo-fibrosarcomatous appearance. In the subacute phase, which lasts for about 10 days, the fibroblasts differentiate into osteoblasts and secrete an osteoid matrix at the periphery of the initial myxoid zone, giving it a pseudo-osteosarcomatous appearance. During the late phase, also called the maturation phase, which usually starts between the second and fifth week, bone production can be observed at the periphery of the lesion. Biopsy at this stage will reveal three characteristic zones of myositis ossificans. Hence, early biopsy of the myositis ossificans lesion can lead to misdiagnosis of sarcoma. [17]
Previously due to the uncertainty of malignancy, mutilating surgeries were carried out. [4] However, substantial research and case studies on myositis ossificans over the decades have enabled clinicians to make a diagnosis without undertaking such radical measures. Treatments such as nonsteroidal anti - inflammatory drugs (indomethacin), hydrochloride injections, laser treatment, and acetic acid iontophoresis have been used with some success although the evidence on these is limited. [18]
The prognosis of such lesions is generally good. Of seven documented cases of myositis ossificans occurring at the humerus (three brachialis, two deltoid, and one triceps brachii), four resolved completely, two did not, and one was lost to follow up. [6] For this reason, the management of myositis ossificans is largely conservative. To summarise, we report a rare case of myositis ossificans of the humeral insertion of pectoralis major following a single episode of trauma, which to our knowledge, has not been previously documented. Recognition or knowledge of the imaging appearances and natural history are important factors supporting the decision to conservatively treat myositis ossificans.
| References | | |
| 1. | Kransdorf MJ, Meis JM, Jelinek JS. Myositis ossificans: MR appearance with radiologic - pathologic correlation. AJR Am J Roentgenol 1991;157:1243-8. 
|
| 2. | Goldman AB. Myositis ossificans circumscripta: A benign lesion with a malignant differential diagnosis. AJR Am J Roentgenol 1976;126:32-40.
|
| 3. | Geschickter CF, Maseritz IH. Myositis ossificans. J Bone Joint Surg 1938;20:661-74.
|
| 4. | Ogilvie-Harris DJ, Fornasier VL. Pseudomalignant myositis ossificans: Heterotopic new-bone formation without a history of trauma. J Bone Joint Surg Am 1980;62:1274-83.
|
| 5. | Gunn DR, Young WB. Myositis ossificans as a complication of tetanus. J Bone Joint Surg Br 1959;41-B:535-40.
|
| 6. | Thorndike A Jr. Myositis ossificans traumatica. J Bone Joint Surg 1940;22:315-23.
|
| 7. | King JB. Post-traumatic ectopic calcification in the muscles of athletes: A review. Br J Sports Med 1998;32:287-90.
|
| 8. | Ackerman LV. Extra-osseous localized non-neoplastic bone and cartilage formation (so-called myositis ossificans): Clinical and pathological confusion with malignant neoplasms. J Bone Joint Surg Am 1958;40-A:279-98.
|
| 9. | Rockwood CA, Masten FA II, editors. The Shoulder. 2 nd ed. Philadelphia: Saunders;1998. p. 63.
|
| 10. | Provencher MT, Handfield K, Boniquit NT, Reiff SN , Sekiya JK, Romeo AA. Injuries to the pectoralis major muscle: Diagnosis and management. Am J Sports Med 2010;38:1693-705.
|
| 11. | Connell DA, Potter HG, Sherman MF, Wickiewicz TL. Injuries of the pectoralis major muscle: Evaluation with MR Imaging. Radiology 1999;210:785-91.
|
| 12. | Schepsis AA, Grafe MW, Jones HP, Lemos MJ. Rupture of the pectoralis major muscle. Outcome after repair of acute and chronic injuries. Am J Sports Med 2000;28:9-15.
|
| 13. | Nuovo MA, Norman A, Chumas J, Ackerman LV. Myositis ossificans with atypical clinical, radiographic, or pathologic findings: A review of 23 cases. Skeletal Radiol 1992;21: 87-101.
|
| 14. | Mortazavi H, Eshghpour M, Niknami M, Saeedi M. Stone man: A case report. Iran J Radiol 2012;10:37-40.
|
| 15. | Thomas EA, Cassar-Pullicino VN, McCall IW. The role of ultrasound in the early diagnosis and management of heterotopic bone formation. Clin Radiol 1991;43:190-6.
|
| 16. | Amendola MA, Glazer GM, Agha FP, Francis IR, Weatherbee L, Martel W. Myositis ossificans circumscripta: Computed tomographic diagnosis. Radiology 1983;149:775-9.
|
| 17. | Mirra JM. Osseous soft tumors. In: Mirra JM, Picci P, Gold RH, editors. Bone Tumors: Clinical, Radiologic and Pathologic Correlations. London: Lea & Febiger; 1989. p. 1549-86.
|
| 18. | Wieder DL. Treatment of traumatic myositis ossificans with acetic acid iontophoresis. Phys Ther 1992;72:133-7.
|
[Figure 1], [Figure 2], [Figure 3], [Figure 4]
|














