| |


 |
| Year : 2014 | Volume
: 8
| Issue : 2 | Page : 58-60 |
|
|
|
|
|
CASE REPORT An unusual cause of mass in the shoulder: A primary hydatid cyst
Serdar Yilmaz, Murat Gulcek, Yunus Demirtas, Sualp Turan
Department of Orthopaedics and Traumatology, Ankara Numune Training and Research Hospital, Ankara, Turkey
Correspondence Address:
Serdar Yilmaz
Department of Orthopaedics and Traumatology, Ankara Numune Training and Research Hospital, Ankara
Turkey
 Source of Support: None, Conflict of Interest: None
DOI: 10.4103/0973-6042.137530
 |
|
|
|
| Date of Web Publication | 24-Jul-2014 |
 Abstract Abstract | | |
A hydatid cyst is a zoonotic infection which may affect any organ and tissue, particularly the liver and the lung. Primary muscular hydatid cysts comprise less than 0.7-3% of the cases. The hydatid cysts must be kept in mind to avoid a diagnostic puncture in cystic lesions to avoid the spreading of the disease. In this case report, we present an exceptionally rare case with an unusual localization of a primary hydatid cyst in the left deltoid muscle.
Keywords: Daughter cyst, deltoid muscle, germinative membrane, hydatid cyst, scolices
How to cite this article:
Yilmaz S, Gulcek M, Demirtas Y, Turan S. An unusual cause of mass in the shoulder: A primary hydatid cyst. Int J Shoulder Surg 2014;8:58-60 |
| Introduction | |  |
A hydatid cyst is a zoonotic infection caused by the larval forms of mostly the Echinococcus granulosus. [1],[2],[3] It is endemic in Middle East and Mediterranean countries and the main host is predominantly dogs. [4] The location and the size of the cyst and the complications such as rupture and immunological reactions are the main source of patient's symptoms. [5] A hydatid cysts may affect any organ and tissue but the most common affected organs are the liver (60-70%) and the lungs (25-30%). [3] Primary muscular hydatid cysts comprise less than 0.7-3% of the cases. [6],[7] The hydatid cysts must be kept in mind to avoid a diagnostic puncture in cystic lesions.
In this case report, we present an exceptionally rare case with an unusual localization of a primary hydatid cyst in the left deltoid muscle.
| Case report | | |
A 64-year-old man working as a farmer in a rural area was admitted to our hospital with a painless growing mass in his left shoulder. He noted the mass on the shoulder about 6 months ago and it grows slowly. As a farmer he has contact with sheep, dogs and cows. There was no history of abdominal pain, chest pain, hemoptysis, cough, fever, weight loss, urticaria or trauma [Figure 1]. Physical examination revealed a firm, nontender, semimobile mass of 10 × 8 cm in diameter on the posterolateral aspect of the left shoulder. There was no fluctuation, restriction of motion, erythema, ecchymosis or lymphadenopathy. The constant score of the patient was 88. An X-ray of the left shoulder revealed a mass without bone involvement. Ultrasonographic examination of the mass showed a big anechoic cyst in the left shoulder with a slightly thick wall which was involving small cystic areas measuring 10 × 7 cm in diameter. Magnetic resonance imaging (MRI) demonstrated a 10 × 7 × 5 cm diameter well-defined, encapsulated, soft tissue cystic lesion in the deltoid muscle. In the posterior part of the deltoid, there were multiple small cystic lesions inside the main cyst [Figure 2]a-c. Abdomen and chest CT showed no evidence of hepatic or pulmonary involvement, and the diagnosis of a primary muscular hydatid disease was made. Laboratory results showed a normal erythrocyte sedimentation rate, C-reactive protein and the echinococcal indirect hemaglutination (IHA). | Figure 1: There was a firm, non-tender mass of 10 × 8 cm in diameter on the posterolateral aspect of the shoulder
Click here to view |
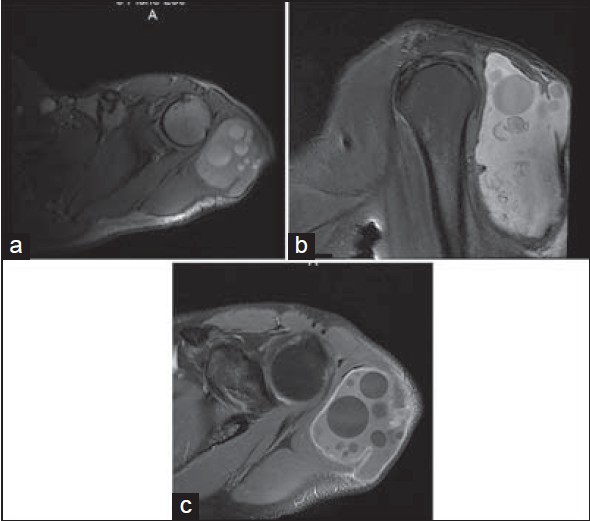 | Figure 2: MRI aspects of T1 weighted axial image (a) and sagittal image (b) with fat suppression of the cyst, also T2-weighted coronal image shows the daughter cysts well (c)
Click here to view |
Surgically, the mass was excised under general anesthesia with wide surgical margin with a posterolateral approach. The deltoid muscle in the margin of the mass was excised. The rotator cuff muscles were not affected. The mass was consisted with cysts and excised completely followed by irrigation with 3% hypertonic saline. The cysts were defined as mother and daughter cysts macroscopically [Figure 3]. Histological examination of the specimen also revealed mother and daughter cysts and fragments of the lamellar membrane of the hydatid cyst. Adjunctive albendazole treatment (400 mg/day) was prescribed for 3 months. The patient was symptom free after 2 years [Figure 4] and the shoulder function remained undisturbed (constant score was 88). There was no inferior subluxation due to deltoid insufficiency. | Figure 3: The mother and daughter cysts of the hydatid cyst were seen extracted in the surgery
Click here to view |
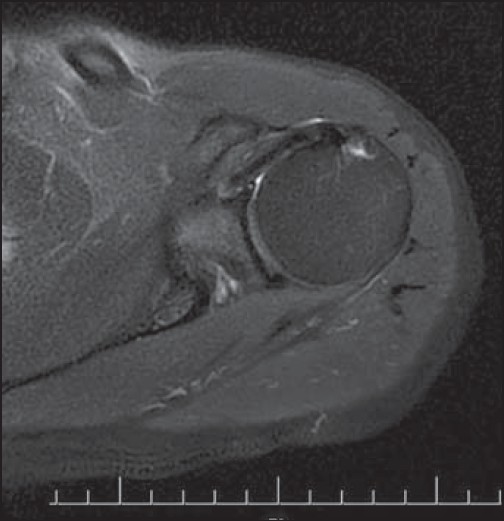 | Figure 4: The cyst was completely disappeared after 2 years on an axial T1-weighted scan
Click here to view |
| Discussion | | |
Hydatid disease is a parasitic infection caused by mainly Echinococcus granulosus. Dogs are the main hosts and the disease was transmitted to humans by the expelled eggs in the feces of the dogs. [1],[2],[3] A hydatid cyst is most frequently found in the liver and lungs, but can also be seen anywhere. [6],[7] Primary muscular hydatid cysts were uncommon and usually located in the peripheral muscles such as supraspinatus, biceps brachii, pectoralis major, gracilis, psoas, sartorius and quadriceps have been reported in the literature. [6],[7],[8],[9],[10],[11],[12],[13] A hydatid cyst in the deltoid muscle was reported in two cases in the literature. [14],[15]
The main symptom is palpable swelling in muscular hydatid disease. [9] Contact with animals must be questioned in the history. Ultrasonography can be used in the diagnosis, but magnetic resonance imaging (MRI) is very useful and gave more information in the diagnosis. [14],[16] The multicystic appearance with homogenous intensity and the daughter vesicles are typical signs of a hydatid cyst in MRI. If the appearance of the 'scolices' was seen in the surgery, the diagnosis was confirmed. [3] If there was any suspicion of a hydatid cyst in the muscle, a diagnostic biopsy or aspiration must be avoided to prevent the spreading of the daughter vesicles. [3],[17] Serologic tests can be used in the diagnosis and are valuable when they are positive, but half of the primary muscular hydatid cases gave a false-negative result as in our case. The indirect hemagglutination test (IHA) sensitivity rate has been reported as 67%. [18],[19]
The proposed treatment method in case of a muscular hydatid cyst is total surgical excision. [3],[9] If the cyst is very large or the surgical procedure is difficult to completely excise, the main purpose is to prevent the spreading of the daughter vesicles to the surrounding tissues. Percutaneous cyst drainage, total excision of the germinative membrane, irrigation of the cyst pouch with scolicidal solution can be applied in this situation. [3],[9],[18] 3% hypertonic sodium chloride can be used as scolicidal solution. [20],[21] We excised the hydatid cyst completely in our case and also irrigated with 3% hypertonic solution.
Medical treatment of a hydatid cyst is not recommended alone, but can be used to prevent recurrence and spread of the disease after surgery. [22] We used albendazol for 3 months after surgery and no recurrence was seen.
As a conclusion, the hydatid cyst must be kept in mind in the differential diagnosis of soft tissue mass in the extremities, especially in regions where this zoonosis is endemic. The diagnosis can be made with the imaging techniques easily without performing a biopsy because of the risk of the contamination of the daughter cysts.
| References | | |
| 1. | Kazakos CJ, Galanis VG, Verettas DA, Polychronidis A, Simopoulos C. Primary hydatic disease in femoral muscles. J Int Med Res 2005;33:703-6. 
|
| 2. | Casero RD, Costas MG, Menso E. An unusual case of hydatid disease: Localization to the gluteus muscle. Clin Infect Dis 1996;23:395-6.
|
| 3. | Kammerer WS, Schantz PM. Echinococcal disease. Infect Dis Clin North Am 1993;7:605-18.
|
| 4. | Aytac A, Yurdakul Y, Ikizler C, Olga R, Saylam A. Pulmonary hydatid disease: Report of 100 patients. Ann Thorac Surg 1977;23:145-51.
|
| 5. | Ahmad S, Jalil S, Saleem Y, Suleman BA, Chughtai N. Hydatid cysts at unusual sites: Reports of two cases in the neck and breast. J Pak Med Assoc 2010;60:232-4.
|
| 6. | Tatari H, Baran O, Sanlidað T, Göre O, Ak D, Manisali M, et al. Primary intramuscular hydatidosis of supraspinatus muscle. Arch Orthop Trauma Surg 2001;121:93-4.
|
| 7. | Singh CM. Hydatid cyst of adductor longus. J Indian Med Assoc 1990;88:288.
|
| 8. | Duygulu F, Karaoðlu S, Erdoðan N, Yildiz O. Primary hydatid cyst of the thigh: A case report of an unusual localization. Turk J Pediatr 2006;48:256-9.
|
| 9. | Di Gesù G, Picone A, La Bianca A, Massaro M, Vetri G. Muscular and subcutaneus hydatidosis. Minerva Med 1987;78:835-40.
|
| 10. | Prousalidis J, Tzardinoglou K, Sgouradis L, Katsohis C, Aletras H. Uncommon sites of hydatid dissase. World J Surg 1998;22:17-22.
|
| 11. | Melis M, Marongiu L, Scintu F, Pisano M, Capra F, Zorcolo L, et al. Primary hydatid cysts of psoas muscle. ANZ J Surg 2002;72:443-5.
|
| 12. | Rask MR, Lattig GJ. Primary intramuscular hydatidosis of the sartorius. Report of a case. J Bone Joint Surg Am 1970;52:582-4.
|
| 13. | Abdel-Khaliq RA, Othman Y. Hydatid cyst of pectoralis major muscle. Case report and note on surgical management of muscle echinococcosis. Acta Chir Scand 1986;152:469-71.
|
| 14. | Vasilevska V, Zafirovski G, Kirjas N, Janevska V, Samardziski M, Kostadinova-Kunovska S, et al. Imaging diagnosis of musculoskeletal hydatid disease. Prilozi 2007;28:199-209.
|
| 15. | Ozdemir G, Zehir S, Ozdemir BA, Sipahioðlu S, Severge U. Hydatid cyst involvement of shoulder and deltoid muscle: A case report. Joint Diseases & Related Surgery 2012;23:173-6.
|
| 16. | Martin J, Marco V, Zidan A, Marco C. Hydatid disease of the soft tissues of the lower limb: Findings in three cases. Skeletal Radiol 1993;22:511-4.
|
| 17. | Mseddi M, Mtaoumi M, Dahmene J, Ben Hamida R, Siala A, Moula T, et al. Hydatid cysts in muscles: Eleven cases. Rev Chir Orthop Reparatrice Appar Mot 2005;91:267-71.
|
| 18. | Durakbasa CU, Tireli GA, Sehiralti V, Sander S, Tosyali AN, Mutus M. An audit on pediatric hydatid disease of uncommon localization: Incidence, diagnosis, surgical approach, and outcome. J Pediatr Surg 2006;41:1457-63.
|
| 19. | Biava MF, Dao A, Fortier B. Laboratory diagnosis of cystic hydatic disease. Word J Surg 2001;25:10-4.
|
| 20. | Cannon CP, Nelson SD, Panosian CB, Seeger LL, Eilber FR, Eckardt JJ. Soft tissue echinococcosis: A report of two cases and review of the literature. Clin Orthop Relat Res 2001; 186-91.
|
| 21. | Tokmak M, Bekler H, Alioðlu Y, Ertav A. Primary muscular hydatid cyst disease. Acta Orthop Traumatol Turc 1995; 29:167-9.
|
| 22. | Bonifacino R, Dogliani E, Craig PS. Albendazole treatment and serological follow-up in hydatid disease of bone. Int Orthop 1997;21:127-32.
|
[Figure 1], [Figure 2], [Figure 3], [Figure 4]
|













