| |


 |
| Year : 2014 | Volume
: 8
| Issue : 3 | Page : 90-93 |
|
|
|
|
|
CASE REPORT Scapular spine stress fractures: To fix or not to fix, our experience in a patient with bilateral fractures and review of the literature
Karuppaiah Karthik, Jason Lau, Joydeep Sinha, Adel Tavakkolizadeh
Department of Orthopaedic Surgery, King's College Hospital, Denmark Hill, London, United Kingdom
Correspondence Address:
Karuppaiah Karthik
King's College Hospital, Denmark Hill, London - SE5 9RS
United Kingdom
 Source of Support: None, Conflict of Interest: None  | 1 |
DOI: 10.4103/0973-6042.140117
 |
|
|
|
| Date of Web Publication | 4-Sep-2014 |
 Abstract Abstract | | |
We report a case of bilateral scapular spine stress fracture, treated conservatively on one side and operatively on the other side. Besides, we performed a literature review to establish management options. A 61-year-old right-handed gentleman came to our clinic with acute on chronic deterioration of shoulder pain and loss of arm function. Clinical assessment and investigations revealed long-standing bilateral rotator cuff tear and scapular spine stress fractures. The fracture on the right side united with conservative management for 2 months. However, his left side remained symptomatic with pain, abnormal mobility and no radiological evidence of union. The fracture progressed to union after fixation and bone grafting. At the final follow-up at 2 years, the patient was asymptomatic with regards to the fractures with Oxford Shoulder Score (OSS)-30 and Disabilities of the Arm, Shoulder and Hand (DASH)-30.8. Fracture union either by conservative or operative treatment is associated with good functional outcome and is supported by our review.
Keywords: Cuff tear arthropathy, scapula fracture, scapula spine stress fracture, stress fracture
How to cite this article:
Karthik K, Lau J, Sinha J, Tavakkolizadeh A. Scapular spine stress fractures: To fix or not to fix, our experience in a patient with bilateral fractures and review of the literature. Int J Shoulder Surg 2014;8:90-3 |
How to cite this URL:
Karthik K, Lau J, Sinha J, Tavakkolizadeh A. Scapular spine stress fractures: To fix or not to fix, our experience in a patient with bilateral fractures and review of the literature. Int J Shoulder Surg [serial online] 2014 [cited 2016 Aug 23];8:90-3. Available from: http://www.internationalshoulderjournal.org/text.asp?2014/8/3/90/140117 |
| Introduction | |  |
Scapular spine stress fractures are uncommon following cuff tear arthropathy, there are only six reported cases in the English literature. [1],[2],[3],[4] Management of these fractures remains a challenge because of poor bone quality and persistent deforming force at the fracture site. [4] Management of these fractures can be conservative or surgical, with good functional outcome being associated with fracture union. Conservative management can lead to asymptomatic nonunion, [3],[4] and there is a risk of recurrence of symptoms leading to a painful stiff shoulder. [1] We present a case of bilateral scapular spine stress fractures that was treated operatively on one side and conservatively on the other with satisfactory functional outcome, besides we reviewed the literature to find the optimal treatment option.
| Case report | | |
A 61-year-old right-hand dominant gentleman was referred to our clinic with sudden deterioration bilateral shoulder pain and loss of function. He was a retired ambulance driver with long-standing and established bilateral massive rotator cuff tear and arthropathy (worse on the left). Clinically, he had very limited and painful, active movements bilaterally (30° of abduction and forward flexion, no external rotation and internal rotation to sacrum). He had minimal supraspinatus and infraspinatus power and markedly weakened subscapularis. He was tender over both scapular spines, with significant site mobility and pain on the left side.
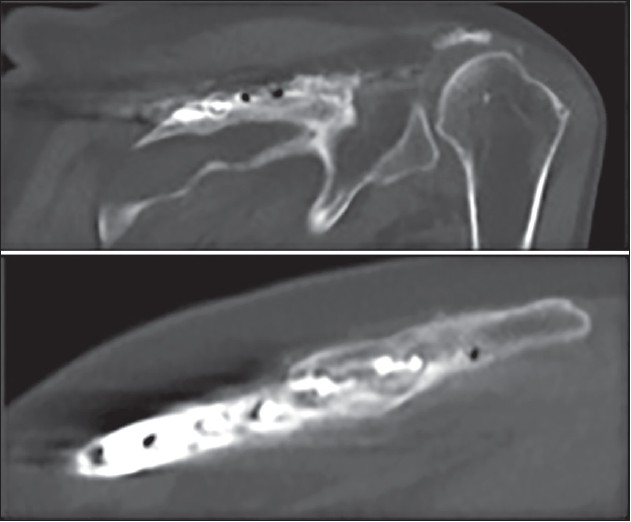
Shoulder radiographs, computed tomography (CT) and magnetic resonance imaging (MRI) revealed chronic bilateral massive rotator cuff tears with significant retraction of the supraspinatus and infraspinatus associated with fatty infiltration. There was associated superior migration of the humeral head on both sides with the loss of acromio-humeral space. Bilateral stress fractures of the spine of scapula were noted with the left side being significantly displaced with no evidence of healing [Figure 1]. Dual energy X-ray absorptiometry scan revealed early osteopenia without osteoporosis. The patient had a history of chronic obstructive pulmonary disease (COPD) and suffered from noninsulin-dependent diabetic mellitus.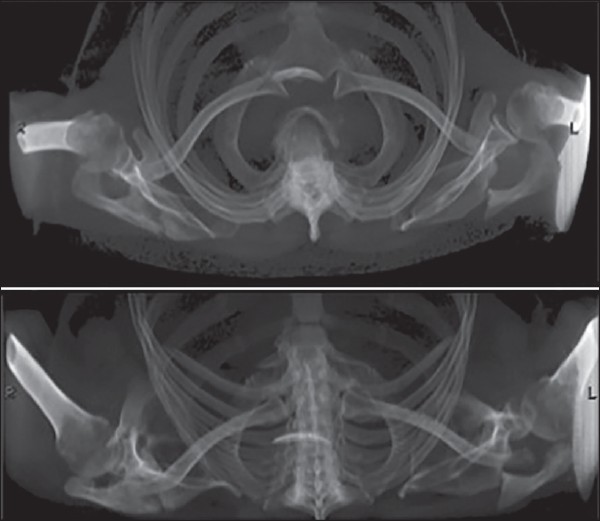 | Figure 1: Computed tomography reconstruction on initial presentation showing bilateral scapula spine fractures. Note the left side is grossly displaced compared to the right
Click here to view |
Although, he initially had severe pain in both shoulders, symptoms in his right shoulder reduced with conservative treatment after 2 months, with diminishing pain and functional improvement. This was further confirmed with X-rays and CT scans showing callus formation and progression to union [Figure 2]. However, his left side remained symptomatic with pain, abnormal mobility at the fracture site, and no radiological evidence of healing [Figure 3]. The patient underwent a successful open reduction and internal fixation of the left scapular spine with 3.5 mm limited contact dynamic compression plate (Synthes) and iliac crest bone grafting. Postoperatively the arm was immobilized in a polysling allowing rotational movements and pendulum exercises for 4 weeks. This was followed by active assisted forward flexion and abduction to 90° for further 2 weeks and a full range of movement exercises as tolerated by the patient after 6 weeks. The fracture progressed to union uneventfully with significant improvement in symptoms and function in his left shoulder [Figure 4]. As the patient's symptoms improved, he refused further treatment and arthroplasty for his cuff tear arthropathy as his level of symptoms were manageable.
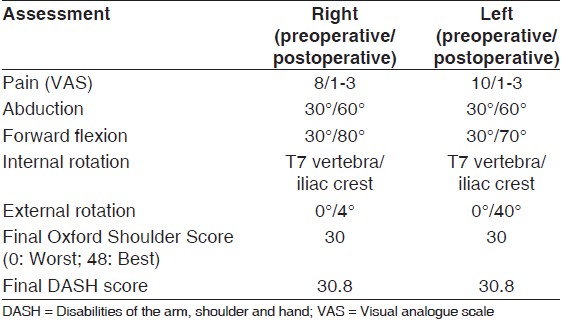
At the final follow-up at 2 years, the patient was asymptomatic with regards to the scapular spine fractures with reasonably good function [Table 1]. He was able to drive and managed his activities of daily living well. His Oxford Shoulder Score (OSS) [5] was 30 for both shoulders and disabilities of the arm, shoulder and hand (DASH) [6] score was 30.8 at the final follow-up.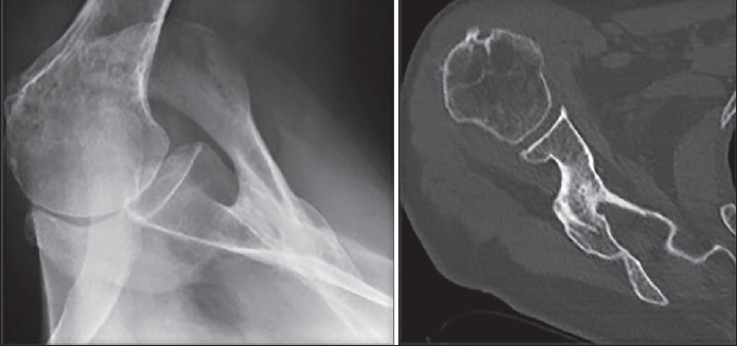 | Figure 2: Radiograph (left) and computed tomography scan (right) of the right shoulder after conservative treatment showing evidence of callus formation and healing. This correlated well with clinical symptoms of reducing pain and improving function
Click here to view |
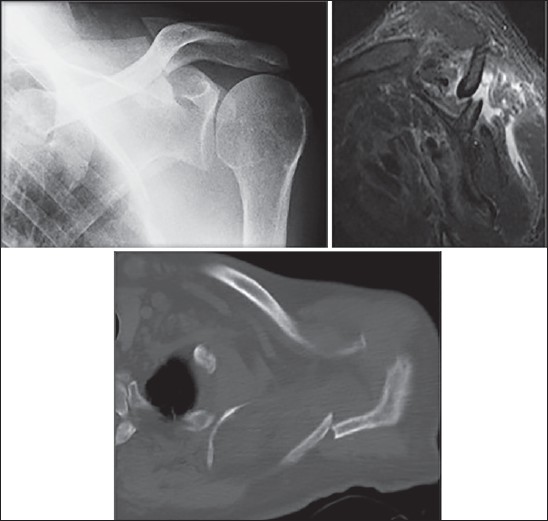 | Figure 3: Radiograph (top left), magnetic resonance imaging (top right) and computed tomography (bottom) of the left shoulder showing evidence of nonunion of the scapula spine fracture, this correlated with persistent symptoms of pain and increased mobility at the fracture site
Click here to view |
 | Figure 4: Follow-up computed tomography scan of the left shoulder at 2 years after open reduction and internal fixation with plates and screws showing bony union
Click here to view |
| Discussion | | |
Massive rotator cuff tears alter the kinematics of the gleno-humeral articulation. [7] In patients with massive cuff tears, the humeral head comes into contact with the overlying acromion during movements in the arm. [4] This may lead to antero-superior migration of the humeral head and altered bio-mechanics. During shoulder movements, the elevated humeral head transfers increased loads across the acromion, and the spine of scapula. Over time, these abnormal forces on the acromion could lead to remodeling of the acromion and spine of scapula according to Wolfe's Law [8] with acetabularization of the acromion. [4] However, in patients with other predisposing factors such as osteopenia in our patient and other patients reported in the literature, the risk of stress fractures increases because of the reduced remodeling potential. Other reported factors in the literature include radiotheraphy, [4] chronic steroid use [1],[4] and osteoporosis. [3] COPD can be a mechanical factor, where chronic cough produces repetitive micro-trauma to an already weakened bone. [1],[9] In our case, steroid use, chronic cough, and osteopenia secondary to long-standing COPD in addition to long-standing cuff tear arthropathy likely led to the stress fractures.
A Medline search was conducted to find all articles on scapular spine stress fractures from 1966 to March 2013 [Table 2]. Groot et al., [1] treated two such patients with physiotherapy, analgesics and ultrasound bone growth stimulation, however, the fractures did not unite, and the patients ended up with painful stiff shoulders [Table 2]. Interestingly, one of their patients whose symptoms settled initially presented after 10 months with recurrence of severe pain. This raises doubts about leaving the asymptomatic nonunion without treatment, as it can lead to further disability in an already compromised shoulder. Shindle et al., [4] in his study tried conservative treatment in two patients and eventually ended up operating on both. In one patient where the fracture was fixed with plates and screws, the fracture united and the patient regained painless shoulder elevation despite cuff deficiency at 3 months. In the second patient, the scapula fracture failed to progress to union with conservative management but was minimally displaced. Her pain was not thought to be due to a fracture, so a reverse total shoulder arthroplasty was performed, however, the patient developed postoperative infection and died. Biomechanically, reverse total shoulder arthroplasty reverses the forces responsible for stress fractures of acromion and scapular spine in cuff tear arthropathy, however increased tension, and elongated deltoid can potentially worsen the situation by increasing the stress in acromion and scapular spine in the opposite direction. [10],[11] In patients with scapular spine stress fracture following reverse total shoulder arthroplasty, operative fixation is the treatment of choice, [10] as poor functional results were associated with conservative treatment. [11] Roy et al, [3] treated a patient with minimal symptoms from a scapular spine stress fracture conservatively. The patient was wheelchair-bound and was admitted in a medical ward for heart failure and chronic varicose ulcers. At 6 months follow-up the patient had a pain-free nonunion.
Our patient had both operative and conservative management of the fractures. Both the fractures united and patient recovered well. The outcome scores measured at the final follow-up did not accurately reflect his recovery from the scapular spine stress fractures. Some components of the score, such as household chores and shopping and recreational activities, were limited because of his severe COPD rather than his shoulder problems. In addition, the preexisting cuff tear arthropathy limited his function in overhead activities. However, the OSS and DASH scores were equal at final follow-up for both shoulders highlighting the fact that the fracture union is essential to regain prefracture levels of function.
Based on present literature review, union following symptomatic scapular spine stress fracture is associated with good functional outcome. However, even in patients with painless nonunion, there is a risk of recurrence of symptoms that may result in a painful stiff shoulder. If conservative treatment fails, operative treatment can be considered if the shoulder remains symptomatic.
| Conclusion | | |
Scapular spine stress fractures are rare, but can occur in patients with a combination of massive rotator cuff tear with arthropathy and poor bone quality. Fracture union either by conservative or operative route is associated with a good functional outcome and is supported by our literature review.
| References | | |
| 1. | Groot D, Giesberts AM, van Mourik JB. Spontaneous scapular spine fracture related to rotator cuff pathology: A report of two cases. Strategies Trauma Limb Reconstr 2012;7:105-7. 
|
| 2. | Ho KM, Schranz P, Wallace WA. ′Stress′ fracture of the scapula. Injury 1993;24:498.
|
| 3. | Roy N, Smith MG, Jacobs LG. Stress fracture of base of the acromion. Ann Rheum Dis 2002;61:944-5.
|
| 4. | Shindle MK, Wanich T, Pearle AD, Warren RF. Atraumatic scapular fractures in the setting of chronic rotator cuff tear arthropathy: A report of two cases. J Shoulder Elbow Surg 2008;17:e4-8.
|
| 5. | Dawson J, Rogers K, Fitzpatrick R, Carr A. The Oxford shoulder score revisited. Arch Orthop Trauma Surg 2009;129:119-23.
|
| 6. | Hudak PL, Amadio PC, Bombardier C. Development of an upper extremity outcome measure: The DASH (disabilities of the arm, shoulder and hand) [corrected]. The Upper Extremity Collaborative Group (UECG) Am J Ind Med 1996;29:602-8.
|
| 7. | Yamaguchi K, Sher JS, Andersen WK, Garretson R, Uribe JW, Hechtman K, et al. Glenohumeral motion in patients with rotator cuff tears: A comparison of asymptomatic and symptomatic shoulders. J Shoulder Elbow Surg 2000;9:6-11.
|
| 8. | Frost HM. Wolff′s Law and bone′s structural adaptations to mechanical usage: An overview for clinicians. Angle Orthod 1994;64:175-88.
|
| 9. | Franco M, Albano L, Blaimont A, Barrillon D, Bracco J. Spontaneous fracture of the lower angle of scapula. Possible role of cough. Joint Bone Spine 2004;71:580-2.
|
| 10. | Crosby LA, Hamilton A, Twiss T. Scapula fractures after reverse total shoulder arthroplasty: Classification and treatment. Clin Orthop Relat Res 2011;469:2544-9.
|
| 11. | Walch G, Mottier F, Wall B, Boileau P, Molé D, Favard L. Acromial insufficiency in reverse shoulder arthroplasties. J Shoulder Elbow Surg 2009;18:495-502.
|
[Figure 1], [Figure 2], [Figure 3], [Figure 4]
[Table 1], [Table 2]
|