|
| Article Access Statistics | | | Viewed | 576 | | | Printed | 8 | | | Emailed | 0 | | | PDF Downloaded | 17 | | | Comments | [Add] | | |
|


Click on image for details.
|
|
| |


 |
| Year : 2016 | Volume
: 10
| Issue : 1 | Page : 49-51 |
|
|
|
|
|
LETTER TO THE EDITOR A unique bipolar clavicle fracture sustained with minimal trauma
Rupert James Talboys, Mandytien Mak, Nitin Modi, Sunil Garg, Hersh Deo
Department of Trauma and Orthopaedic Surgery, James Paget University Hospital, Gorleston-on-Sea, Great Yarmouth, Norfolk, NR31 6LA, United Kingdom
Correspondence Address:
Rupert James Talboys
Department of Trauma and Orthopaedic Surgery, James Paget University Hospital, Gorleston-on-Sea, Great Yarmouth, Norfolk, NR31 6LA
United Kingdom
 Source of Support: None, Conflict of Interest: None  | Check |
DOI: 10.4103/0973-6042.174524
 |
|
|
|
| Date of Web Publication | 20-Jan-2016 |
How to cite this article:
Talboys RJ, Mak M, Modi N, Garg S, Deo H. A unique bipolar clavicle fracture sustained with minimal trauma. Int J Shoulder Surg 2016;10:49-51 |
Sir,
Segmental clavicle fractures are unusual injuries. When they occur, they tend to involve the mid-shaft and lateral clavicle. An injury is comprising the medial and lateral clavicle fractures, or a bipolar fracture, is rarely seen. There have only been four cases of bipolar clavicle fracture reported in the literature, all of which were the result of high-impact injuries. [1],[2],[3],[4] Due to their infrequency, there is currently no consensus on treatment modality.
A 79-year-old right-handed female presented to our hospital with a painful left shoulder following a mechanical fall. She had tripped over a discarded slipper while getting out of bed, landing on her left adducted shoulder on a carpeted floor. On examination, there was a palpable deformity, with an apparent inferior displacement of the medial clavicle. The lateral clavicle was tender to palpation, with no obvious deformity. Her range of movement was limited by pain; however, there was no neurovascular or respiratory compromise, and no skin tenting. A plain chest X-ray revealed a bipolar segmental fracture [Figure 1], which was subsequently confirmed by a computed tomography (CT) scan [Figure 2]. There were two fractures, the first an extra-articular Allman Group II (Neer Type I fracture) at the lateral end, [4] and the seconds, an anteriorly displaced fracture of the medial clavicle (Allman Group III). The patient was comfortable in a polysling, and her pain was well controlled with simple analgesia.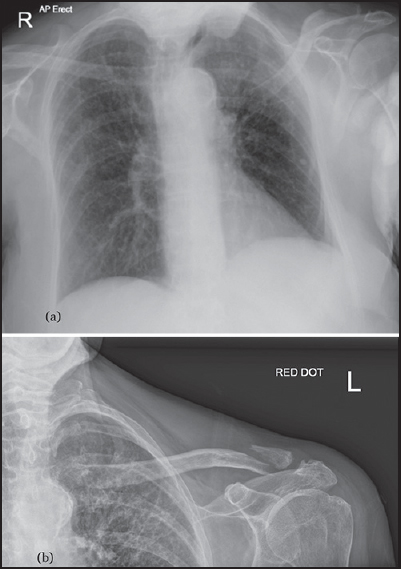 | Figure 1: X-rays are showing a left bipolar clavicle fracture on presentation. (a) Chest X-ray is showing no evidence of pneumothorax. (b) Magnified view of bipolar fracture
Click here to view |
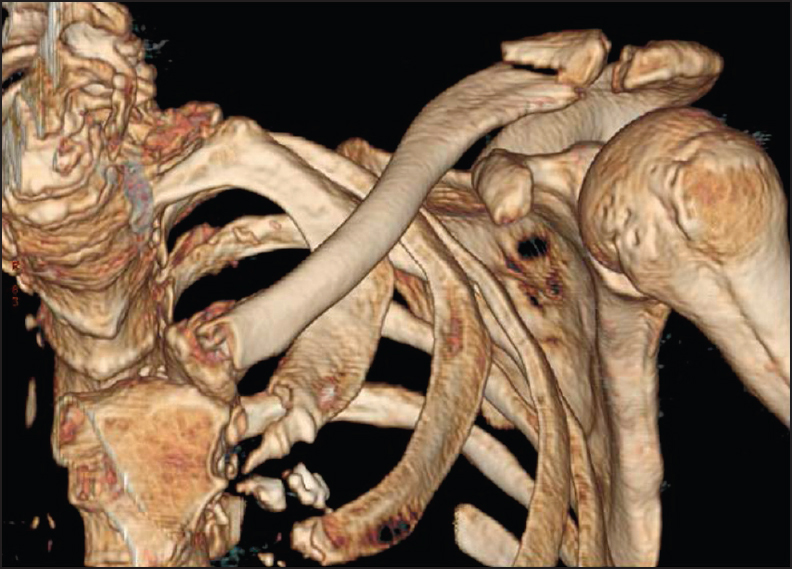 | Figure 2: Computed tomography imaging with three-dimensional reconstruction of the bipolar fracture
Click here to view |
Prior to this admission, she was independent with all daily activities, and did not require any mobility aids. However, she had a body mass index of 18, and she was very frail. She was also an ex-smoker. Her medical background included the chronic obstructive pulmonary disease (COPD) and hypertension. There was no history of previous falls or associated with fragility fractures.
Incidentally, the patient had been admitted for an exacerbation of her COPD 3 months previously; her chest X-ray then revealed no earlier injuries to the clavicle [Figure 3]. The patient gave a clear history, denying traumatic injuries to the shoulder in between these two admissions. This allowed us to ascertain that the bipolar fracture was the result of a single fall as described above, rather than an injury sustained over the separate occasions.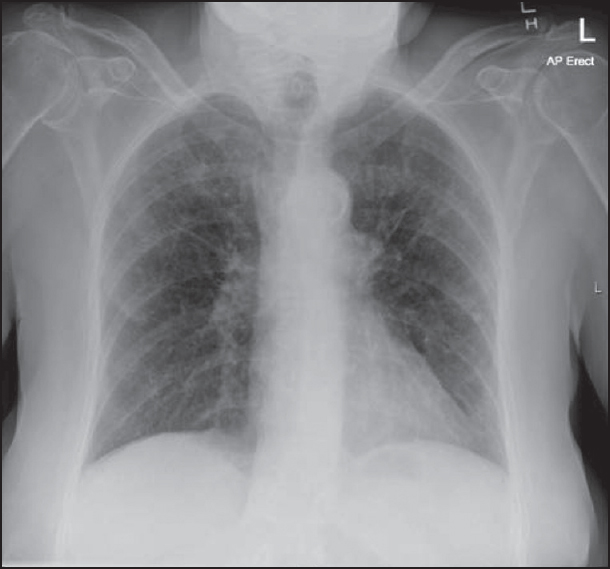 | Figure 3: Chest X-ray 3 months prior to admission, showing no preexisting shoulder injury
Click here to view |
Taking into account, the extent of injury in a frail patient, whose pain was well controlled, a decision was made with the patient's consent to proceed with conservative management. Her shoulder was immobilized in a polysling, with a plan to follow her up with serial X-rays and to review her in the fracture clinic. At 3 weeks postinjury, the patient had a reasonable pain-free range of movement, and her repeat X-ray was satisfactory. The patient then developed other significant medical issues, which required a care at another hospital. She was subsequently followed up with telephone consultations. At 3 months, the patient reported the complete pain relief and no functional deficit from her affected shoulder.
An isolated fracture of the clavicle is common and accounts for up to 4% of all A and E attendances, [5] and 44% of all shoulder girdle injuries. [2] Fractures of the mid-shaft of the clavicle are most common (up to 82%); however, in elderly patients, fractures of the medial or lateral clavicle are more prevalent. [5] Lateral clavicle fractures make up 21% of all clavicle fractures. On the other hand, those at the medial end account for <5%. These can be subtle, and the diagnosis may occasionally be missed. [4] Furthermore, visualization around the medial clavicle on plain radiographs may at times pose a diagnostic challenge due to overlying structures in the chest. [3] Indeed, its incidence may have been under-reported, with many fractures remaining undiagnosed. [4] In our case, it was clear from clinical examination and on plain film that there was the involvement of the medial clavicle. In cases, where the visualization may be obscured on plain radiographs, CT imaging and three-dimensional modeling techniques are invaluable tools for diagnosis, and are perhaps underused in current practice. [2]
The most widely recognized mechanism for clavicle fractures is a direct force to the adducted shoulder following a fall. Medial fractures are usually result from a high-energy impact, and it has been suggested that a segmental fracture is the result of multiple, direct, and high-energy blows to the clavicle. [2],[3] Indeed, all four cases of bipolar clavicle fractures reported to date were all sustained from high-impact injuries. [1],[2],[3],[4]
Most clavicle fractures can be managed nonoperatively in a polysling. Surgery is generally reserved for more complex injuries such as open fractures, significantly displaced fractures, neurovascular compromise, or complications such as delayed or nonunion.
Bipolar fractures were previously associated with high-impact injuries and sequential forces to the clavicle. [2],[3],[4] Our case was the first to demonstrate that it can also present in low-impact mechanical falls in the elderly. Fractures of the medial clavicle may be difficult to identify on plain radiographs. [2] Where doubt remains as to whether or not there has been a bipolar fracture, CT imaging offers superior visualization, and should be considered, [2] especially with the increasing availability of scanners. The diagnosis of a bipolar fracture is important, as it is an unstable injury and may require the operative management. From previously published cases, it appears that patients with higher functional demands and with significantly displaced fractures would benefit from the surgical fixation. Conversely, in those with relatively little functional demands, preexisting co-morbidities and who are asymptomatic, conservative management is a viable option.
In this letter, we have described an unusual injury with an unreported mechanism of injury a low-impact fall. We have summarized the current treatment regimes.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
 References References | |  |
| 1. | Pang KP, Yung SW, Lee TS, Pang CE. Bipolar clavicular injury. Med J Malaysia 2003;58:621-4.  |
| 2. | Sethi K, Newman SD, Bhattacharya R. An unusual case of bipolar segmental clavicle fracture. Orthop Rev (Pavia) 2012;4:e26. |
| 3. | Heywood R, Clasper J. An unusual case of segmental clavicle fracture. J R Army Med Corps 2005;151:93-4. |
| 4. | Miller D, Smith KD, McClelland D. Bipolar segmental clavicle fracture. Eur J Orthop Surg Traumatol 2009;19:337-9. |
| 5. | Nordqvist A, Petersson C. The incidence of fractures of the clavicle. Clin Orthop 1994;300:127-32. |
[Figure 1], [Figure 2], [Figure 3]
|
|











