|
| Article Access Statistics | | | Viewed | 583 | | | Printed | 12 | | | Emailed | 0 | | | PDF Downloaded | 17 | | | Comments | [Add] | | |
|


Click on image for details.
|
|
| |


 |
| Year : 2016 | Volume
: 10
| Issue : 1 | Page : 48-49 |
|
|
|
|
|
LETTER TO THE EDITOR Snapping shoulder caused by glenoid labral bone apposition: A case report
Tomoya Takasago, Kiminori Yukata, Toshihiko Nishisho, Natsuo Yasui
Department of Orthopedics, Tokushima University Hospital, 3-18-15 Kuramoto, Tokushima - 770-8503, Japan
Correspondence Address:
Kiminori Yukata
Department of Orthopedics, Tokushima University Hospital, 3-18-15 Kuramoto, Tokushima - 770-8503
Japan
 Source of Support: None, Conflict of Interest: None  | Check |
DOI: 10.4103/0973-6042.174522
 |
|
|
|
| Date of Web Publication | 20-Jan-2016 |
How to cite this article:
Takasago T, Yukata K, Nishisho T, Yasui N. Snapping shoulder caused by glenoid labral bone apposition: A case report. Int J Shoulder Surg 2016;10:48-9 |
Sir,
We describe an unusual case of shoulder snapping and pain caused by bone apposition on the glenoid labrum related to osteoarthritis of the shoulder.
An 84-year-old right hand-dominant woman presented with right shoulder pain since 5 years and snapping during shoulder elevation and reduced range of motion. In particular, she complained of the right shoulder pain while getting up from the bed using her hand (push-up motion at the shoulder abduction). There was no history of trauma. The patient had been conservatively treated, but symptoms worsened during few months before the consultation. Physical examination revealed some tenderness over the coracoid process. Snapping occurred frequently during abduction at 45° or 70° or external rotation during abduction.
Plain radiographs confirmed severe osteoarthritis of both glenohumeral joints and calcified tumors under the coracoid process [Figure 1]a]. Computed tomography showed a small bony tumor at the superior-posterior glenoid rim [Figure 1]b-e]. Arthrography revealed a small defect of contrast media at superior-posterior area of the joint space, but no multiple loose bodies or subacromial leakage [Figure 1]f]. Magnetic resonance imaging revealed joint effusion [Figure 1]g].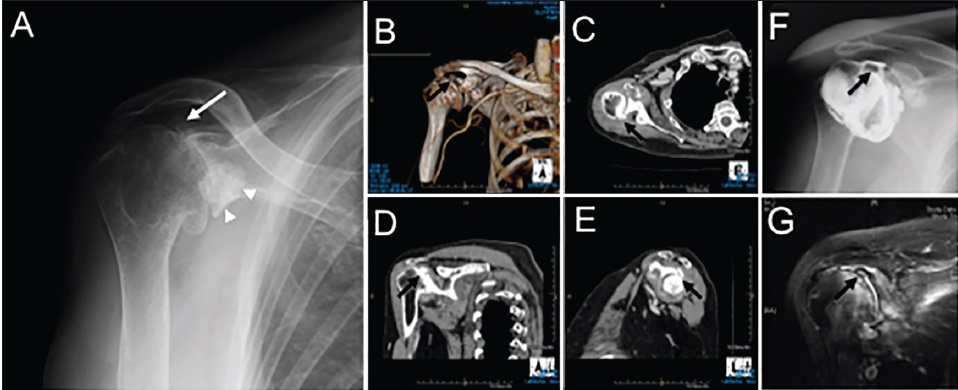 | Figure 1: Antero-posterior radiographs of right shoulder (a). Three-dimension (b), Axial (c), Oblique coronal (d), and oblique sagittal (e) Views of computed tomography of the right shoulder. Antero-posterior view of arthrography (f) and oblique coronal view of enhanced magnetic resonance imaging (g) of the right shoulder. Arrows indicate a small bone fragment at the superior-posterior glenoid rim. Arrowheads showing large bone
fragments under the bilateral coracoid processes
Click here to view |
Arthroscopic findings confirmed intra-articular bone apposition on the glenoid labrum at 11-o'clock position [Figure 2]a-d]. The articular cartilage of both humeral head and glenoid was worn, and further the cancellous bone of the humeral head was partially exposed because it was shaved off by the bone fragment. The patient underwent arthroscopic removal of the bone fragment on the glenoid labrum, partial synovectomy, and resection of the tumor under the coracoid process via an open anterior approach [Figure 2]e]. Histologic examination showed that both intra-and extra-articular tumors were benign osteochondromas.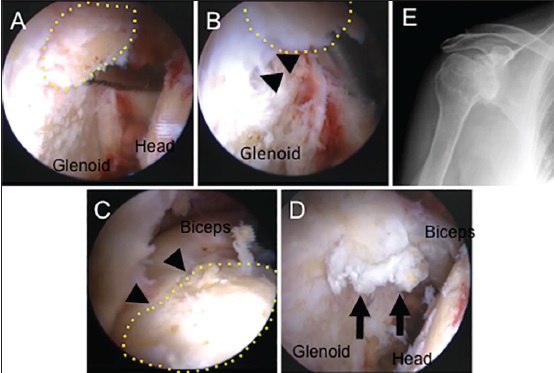 | Figure 2: Arthroscopic views showed the osteochondral fragment was connected with the glenoid labrum at the 11-o'clock position of the right shoulder. Switching rod inserted from the anterior portal was located under the osteochondral fragment (a), and the fragment was moved upward (b) and downward (c) to confi rm the continuity with the labrum (arrowheads). After removal of the osteochondral fragment, an irregular rim of the glenoid labrum was seen (arrows) (d). Postoperative antero-posterior X-ray showed the evidence of removal of the bone fragments (e). A yellow dotted line: osteochondral fragment
Click here to view |
Postoperatively, the patient's shoulder pain during push-up motion and snapping during shoulder elevation were diminished. At the last follow-up, that is, 2 years after the surgery, the patient's shoulder condition had not worsened.
The glenoid labrum is fibrocartilaginous tissue attached around the margin of the glenoid cavity, which provides additional static stability to the glenohumeral joint by increasing socket depth and congruency. [1] Although injuries to the glenoid labrum are frequent pathologic conditions, only a few cases of degenerative abnormalities of the glenoid labrum have been reported. [2],[3] Bone apposition/ossification to fibrocartilaginous tissue, such as the knee meniscus or hip labrum, has been described previously. Corten et al. proposed that repetitive abutment of the femoral neck against the labrum is the underlying pathomechanism for subperiosteal bone apposition at the hip acetabular rim. [4] On the other, intra-articular osteochondral fragment including loose bodies can be produced by various pathologic conditions, such as synovial osteochondromatosis, osteochondritis dissecans, and osteochondral fractures, which might be considered in the differential diagnosis. One possible pathomechanism in the present case is partial ossification of the fibrocartilaginous labrum itself because the osteochondral fragment attached to only the tip of the labrum, but not a loose body.
Thus, labral bone apposition should be considered a possible source of shoulder snapping and pain although its etiology remains unclear.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
 References References | |  |
| 1. | Howell SM, Galinat BJ. The glenoid-labral socket. A constrained articular surface. Clin Orthop Relat Res 1989;243:122-5.  |
| 2. | Yukata K, Imada K, Yoshizumi Y, Tamano K, Hosokawa S, Nakaima N. Intra-articular ganglion cyst (paralabral cyst) of the shoulder associated with recurrent anterior dislocation: A case report. J Shoulder Elbow Surg 2002;11:95-7. |
| 3. | Subhas N, Sundaram M, Bauer TW, Seitz WH Jr, Recht MP. Glenoid labrum ossification and mechanical restriction of joint motion: Extraosseous manifestations of melorheostosis. Skeletal Radiol 2008;37:177-81. |
| 4. | Corten K, Ganz R, Chosa E, Leunig M. Bone apposition of the acetabular rim in deep hips: A distinct finding of global pincer impingement. J Bone Joint Surg Am 2011;93 Suppl 2:10-6. |
[Figure 1], [Figure 2]
|
|











