|
 
 |
| EDITORIAL |
|
| Year : 2013 | Volume
: 1
| Issue : 1 | Page : 1-7 |
|
Nigerian prevention of mother to child transmission of human immunodeficiency virus program: The journey so far
Chris O Agboghoroma1, Solomon A Sagay2, Joseph Ifeanyichukwu Ikechebelu3
1 Department of Obstetrics and Gynaecology, National Hospital, Abuja, Nigeria
2 Department of Obstetrics and Gynaecology, University of Jos, Jos, Nigeria
3 Department of Obstetrics and Gynaecology, Nnamdi Azikiwe University, Nnewi, Nigeria
| Date of Acceptance | 17-Jun-2013 |
| Date of Web Publication | 16-Aug-2013 |
Correspondence Address:
Joseph Ifeanyichukwu Ikechebelu
Editor in Chief. JHHR. c/o Department of Obstetrics and Gynaecology, Nnamdi Azikiwe University, Nnewi Campus
Nigeria
 Source of Support: None, Conflict of Interest: None  | Check |

How to cite this article:
Agboghoroma CO, Sagay SA, Ikechebelu JI. Nigerian prevention of mother to child transmission of human immunodeficiency virus program: The journey so far. J HIV Hum Reprod 2013;1:1-7 |
How to cite this URL:
Agboghoroma CO, Sagay SA, Ikechebelu JI. Nigerian prevention of mother to child transmission of human immunodeficiency virus program: The journey so far. J HIV Hum Reprod [serial online] 2013 [cited 2017 Apr 2];1:1-7. Available from: http://www.j-hhr.org/text.asp?2013/1/1/1/116527 |
| Introduction | |  |
Nigeria is the most populous country in Africa. Estimates based on the 2006 national census and an annual growth rate of 3.2% puts the 2012 population at about 171 million. [1] The high population may be attributed to the high total fertility rate of 5.7%, a large percentage of women in the reproductive age group and a low contraceptive prevalence rate of 15%. [2] The 2008 National Demographic and Health Survey (NDHS) estimates the maternal mortality ratio at 545/100,000 live birth and infant mortality rate at 75 deaths/1,000 live births. [2] The life expectancy at birth for women and men in Nigeria is estimated at 47.1 years and 46 years respectively. [2] This NDHS also revealed that; 36% of pregnant women do not receive any form of antenatal care (ANC), only 35% of deliveries occur in health facilities and 56% of mothers did not receive any post natal care, breastfeeding was nearly universal, with 97% of children being breastfed, although, only 13% of children under 6 months were exclusively breastfed. Health-care provision in Nigeria is a concurrent responsibility of the three tiers of government; the federal, state and local governments, which have broad responsibilities for tertiary, secondary and primary care respectively. The federal government through the Federal Ministry of Health (FMOH) provides policy guidance and technical assistance to the 36 states and Federal Capital Territory, Abuja. The FMOH also implement and/or monitor and evaluate National Health Programs and Policies. In 2011, a census of available Health Facilities in Nigeria showed a total of 34,173, of which 30,098 (88.1%) are Primary Health-Care Facilities, 3,992 (11.7%) secondary and 83 (0.2%) tertiary. [3] Nearly, 38% of these facilities belong to the private sector.
Human immunodeficiency virus (HIV)/acquired immune deficiency syndrome (AIDS) is a major public health problem in Nigeria. Since the report of the first AIDS case in Nigeria in a 13-year-old girl in 1986, serial HIV sentinel surveys of pregnant women in the country recorded persistent high HIV prevalence. Though, with variations across the country, the national median seroprevalence was 1.8% in 1991, 3.8% in 1994, 4.5% in 1996, 5.4% in 1998, 5.8% in 2001, 5.0% in 2003, 4.4% in 2005, 4.6% in 2008 and 4.1% in 2010. [4] With the current estimate of about 3 million persons living with HIV (PLHIV) in Nigeria, it harbors the second largest burden in the world. The morbidity, mortality and socio-economic loss associated with HIV infection is a major treat to future survival of the country. Efforts of the Nigerian Government to control HIV/AIDS in the country led to the establishment of National Agency for the Control of AIDS - formerly National Action Committee on AIDS in 2000 with the responsibility to lead a multi-sectoral response. [5] The HIV/AIDS division in the Department of Public Health of the FMOH, formerly National AIDS and Sexually Transmitted Diseases Control Program is charged with the health sector response.
| Justification | | |
The Nigerian prevention of mother-to-child transmission (PMTCT) of HIV program is one of the health sector responses to the HIV/AIDS epidemic in the country. Mother-to-child transmission (MTCT) is the main route of pediatrics HIV infection. It accounts for over 90% of all pediatrics (children less than 15 years) infection. Without interventions, the rate of MTCT ranges from 25% to 40%, however with effective interventions, MTCT rates have been reduced below 2%. [6] While pediatrics HIV has been virtually eliminated in most developed countries with structured interventions, many developing countries still record high transmission rates. [6],[7],[8] The high prevalence of HIV among pregnant women, high total fertility rate, culture of prolonged breast feeding/missed feeding, non-use of modern health facilities for antenatal and delivery purposes have contributed to the high rate of MTCT in the country. It is estimated that without effective interventions, between 67,500 and 125,000 infants will be infected in a year in the country. [9] The morbidity and mortality associated with pediatrics HIV infection has virtually eroded most of the previous gains of child survival strategies in the country. Some reports suggest that at least one-third of HIV infected children in Africa and other developing countries die within their 1 st year of life. [10],[11]
| Evolution of PMTCT Program in Nigeria | | |
The initiative for the establishment of PMTCT program in Nigeria started with the inauguration of the PMTCT National Task Team (NTT) in December 2000. The PMTCT NTT was saddled with the responsibility of developing the proposal, framework, guidelines, monitoring and evaluating (M and E) the PMTCT program. Actual PMTCT services in Nigeria commenced as a pilot project in July 2002. The goal, objectives and targets of the PMTCT program have undergone some review over time in line with national realities and international demands such as the global initiative for the elimination of MTCT by the year 2015. [12] The current overall goal as documented in the 2010-2015 scale-up plan is to contribute to improved maternal health and child survival through accelerated provision of comprehensive and integrated PMTCT services. [13]
| The Main Elements of the PMTCT Program | | |
One of the main outputs of the PMTCT NTT was the development of National Guidelines on implementation of PMTCT. The national guidelines took into consideration the World Health Organization (WHO) four-prong strategy on PMTCT. [14] The first guideline was produced in 2001 and was reviewed in 2005, 2007 and 2010 in line with scientific development and international best practices based on WHO recommendations. [15],[16],[17],[18] National PMTCT standard operating procedure was also developed to assist with the implementation of the guidelines. [19] The main elements of the National PMTCT program are:
- HIV Information and counseling provided to pregnant women and their spouses. HIV positive clients receive on-going counseling and support.
- Routine rapid HIV testing (with an option to decline) for all women, during the period of pregnancy and/or labor.
- Antiretroviral (ARV) treatment or prophylaxis to HIV infected women. While single-dose nevirapine (sdNVP) in labor was the ARV drug intervention in the first 2-3 years of the program, a more effect combination ARV regimen in form of highly active antiretroviral therapy or zidovudine (AZT) monotherapy are now the recommended drugs.
- ANC and delivery supervised by a skilled health worker to ensure safe delivery and prevent MTCT. Though the importance of cesarean section is acknowledged, its use as a public health measure was restricted with the availability of ARV and lack of access to the service in most health facilities.
- Infant feeding counseling on exclusive breastfeeding and breast milk substitute were the initial practice. Current guidelines emphasize only exclusive breast feeding while the mother and/or infant are on extended use of ARV drugs.
- ARV prophylaxis (NVP or AZT) for the infant for 6 weeks.
- Infant follow-up and HIV testing at 18 months at the early stage of the program. The National PMTCT program has recently introduced polymerase chain reaction services for early infant diagnosis (EID) at 6 weeks.
- Referral of mother, baby and other members of the family for life-long antiretroviral therapy (ART), other reproductive health services and care and support.
- Communication activities including community dialog to improve service up-take and male involvement.
- PMTCT logistics and supplies.
- How to establish new PMTCT site.
- Monitoring and Evaluation (M and E).
| PMTCT Program Management | | |
The secretariat of the PMTCT program is based in the PMTCT unit of the HIV/AIDS Division in the Public Health Department of FMOH with a desk officer responsible for documentation and coordination of the activities.
The PMTCT NTT constitutes the technical working committee on PMTCT and meets quarterly to review PMTCT activities in the country and provide pathways for the PMTCT program. The chairman and members are appointed by the Honorable Minister of Health. Membership include Obstetricians and Gynecologists who are also site coordinators, Pediatricians, Public Health Physicians, representatives from relevant departments/units in the FMOH - (HIV/AIDS, Reproductive Health, Nutrition, Food and Drugs), National Primary Health-Care Development Agency, PLHIV and Development partners active in PMTCT in the country.
The Core Partners Forum is another medium created for core partners, donor organizations and major stakeholders to harmonize their contributions and plans in line with the national strategic plan.
Site PMTCT committee also exist in health facilities rendering PMTCT services. The membership of the site committee includes medical doctors and midwives and nurses working in maternity and child health units, pharmacists, laboratory staff, medical record staff, counselors and social workers. The site committee meet regularly to ensure the PMTCT services are rendered as provided for in the guidelines.
| Research | | |
Two national research initiatives have been undertaken as part of the National PMTCT program. The PMTCT formative research was carried out in the six geopolitical zones in 2001 and 2002 at the commencement of PMTCT services in the country. The second was an operations research within 3 years of the PMTCT program. The findings from both studies were useful in subsequent management of the program.
| Training Curriculum and Capacity Development | | |
Most of the PMTCT program activities are health facility based. The development of capacity to implement the activities was a major agenda of the PMTCT NTT. In order to ensure a uniform, standard and high quality PMTCT services across the country, a comprehensive training curriculum was developed. [20],[21] The course content of the curriculum is divided into the following ten modules:
Module 1: Introduction to HIV/AIDS.
Module 2: Overview of PMTCT of HIV.
Module 3: HIV testing and Counseling of pregnant women.
Module 4: Specific PMTCT interventions.
Module 5: Infant feeding in the context of HIV infection.
Module 6: Linkages to treatment, care and support for mothers and families with HIV infection.
Module 7: Safety and supportive care in the work environment.
Module 8: Communication issues in stigma and discrimination.
Module 9: PMTCT program monitoring.
Module 10: Establishing a PMTCT site.
The 6 days PMTCT training was designed to provide health-care workers with the basic information and skills necessary to deliver core PMTCT services in an integrated manner. The program also provided advanced training for health workers in some aspects of the curriculum including counseling, HIV testing and other laboratory services, ARV drug use in pregnancy, drug management, M and E and EID. With increased emphasis on decentralization of services to Primary Health Centers (PHCs) where service providers are mainly Community Health Extension Workers, the simpler integrated management of adolescent and adult illnesses/integrated management of pregnancy and child birth WHO training curriculum is often used.
| Monitoring and Evaluation | | |
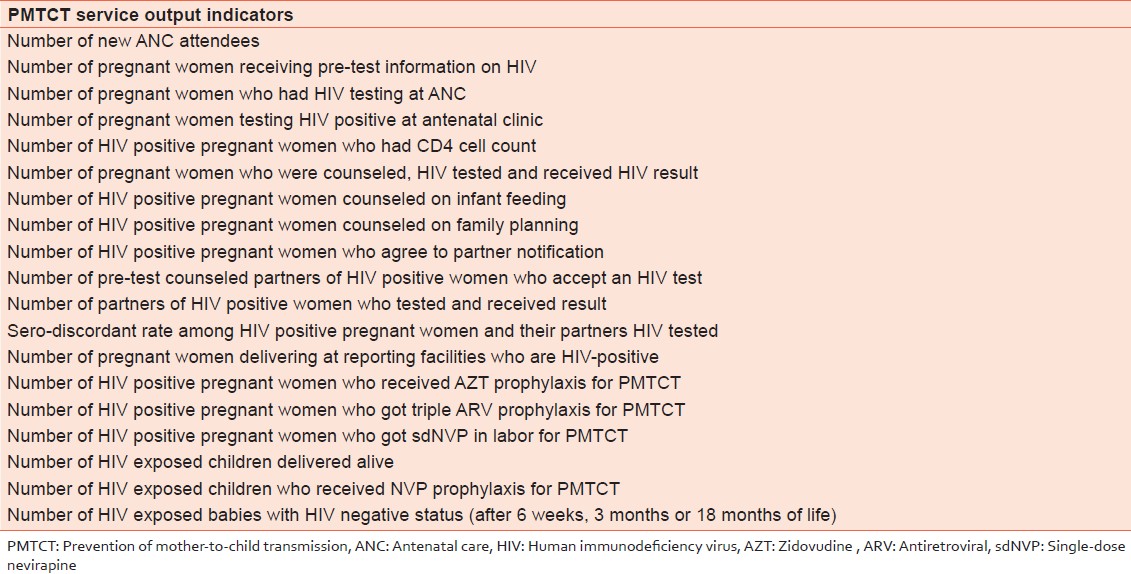
A PMTCT management information system (MIS) was developed early in the program. Specific indicators were identified for programmatic activity and for measurement of program success. [Table 1] shows the National PMTCT service indicators.
A set of registers were developed to capture PMTCT indicator information from service delivery points in the health facilities.
These include:
- The general antenatal clinic register;
- HIV counseling and testing register;
- PMTCT ARV register;
- Partner register;
- Labor and delivery register;
- Maternal follow-up register and
- Child follow-up register.
Two summary forms - monthly counseling and testing summary form and monthly delivery summary form were also developed to capture monthly summary of relevant data.
To ensure quality data collection, entry and reporting, an MIS training curriculum was developed and key service providers and designated M and E officers were trained on accurate use of the MIS tools. Computers and necessary accessories were also provided in the various centers at the start of the PMTCT program. The completed summary forms are transmitted regularly to the central PMTCT MIS database located at the PMTCT unit of the HIV/AIDS department of FMOH Abuja through the state ministry of health and/or the donor/supporting partner.
| PMTCT Program Financing | | |
Though the National PMTCT program is owned by the Federal Government of Nigeria (GON), it is substantially donor driven. The program depends on manpower and infrastructure provided by government in the health facilities. UNICEF sponsored the take-off of PMTCT program including pilot activities in the first six sites in 2001 and 2002 while Gates Foundation funded AIDS Prevention Initiatives in Nigeria (APIN) that supported 2 additional sites from Ibadan and Jos during the same period. Subsequently technical, logistic and financial support for the program came from global fund for the control of HIV/AIDS, malaria and tuberculosis, UN agencies including WHO, United Nations Population Fund and United Nations Program on HIV/AIDS, the United States government through the Centre for Disease Control and Prevention and United States Agency for International Development and their implementing agencies (Institute of Human Virology Nigeria, APIN, Family Health International, ENHANCE, Centre for Development and Population Activities, Global HIV/AIDS Initiative Nigeria and Columbia University) and Clinton foundation. Most of the PMTCT NTT meetings and activities are sponsored by these donors and partners.
| National PMTCT Sites and Targets | | |
Since the commencement of PMTCT program, the first scale-up plan - 2005-2009 was developed to direct the initial expansion of the program in the country. [9] The program started in 2002 in six pilot sites, one in each of the six geopolitical zones in the country - National Hospital, Abuja; Ahmadu Bello University Teaching Hospital, Zaria; University of Nigeria Teaching Hospital, Enugu; University of Port Harcourt Teaching Hospital, Port Harcourt; Lagos University Teaching Hospital, Lagos; and University of Maiduguri Teaching Hospital, Maiduguri. Two additional APIN-Supported sites Jos University Teaching Hospital, Jos and University College Hospital, Ibadan joined in 2002 while Nnamdi Azikiwe University Teaching Hospital, Nnewi and Aminu Kano Teaching Hospital, Kano were established in 2003. There have been progressive increases in PMTCT sites to 250 in 2006, 640 in 2009 and 1,320 by the end of 2012. [22] This has however not translated to effective coverage of the large population of the Nigerian society. It is estimated that in 2009 and 2012 respectively, only 12% and 18% of HIV positive pregnant women received ARVs for PMTCT. With an estimated pool of about 228,800 infected pregnant women and 57,000 children infected principally through MTCT in 2012, Nigeria accounts for over 30% of the global PMTCT gap. [22],[23],[24]
The persistently high burden of HIV and MTCT are indications that the national PMTCT program has only made modest impact. This may be attributed to the low-level of coverage across the country. To address this problem, an accelerated scale-up plan 2010-2015 to rapidly decentralize PMTCT services in the country was developed and is being implemented. [13],[25]
The targets of the 2010-2015 National PMTCT scale-up plan include:
- To ensure at least 50% reduction in HIV incidence among 15-49 year old women by 2015;
- To ensure at least 90% reduction in unmet need for family planning among women with HIV by 2015;
- To ensure at least 90% of all pregnant women have access to quality HIV counseling and testing by 2015;
- To ensure at least 90% of all HIV positive pregnant women and breastfeeding infant - mother pairs receive ARV prophylaxis by 2015;
- To ensure at least 90% of all HIV exposed infants have access to EID services by 2015;
- To ensure at least 90% of pregnant women requiring ART for their own health receive life-long ART.
Nigeria signed up to the global plan for the elimination of new HIV infections among children and keeping their mothers alive. [12] This plan was launched in 2011 and it provides the foundation for country-led movement toward achieving two global targets by 2015; reduce new HIV infections among children by 90% and reduce number of AIDS related maternal deaths by 50%. Since the GON committed to this plan, significant strides have been made, in partnership with development partners, to decentralize PMTCT services to PHCs and rural settings in order to increase coverage. [Table 2] demonstrates the significant achievements in 2012 in comparison to 2011 and previous years with regards to new service points, number of women tested with results and number of HIV positive pregnant women who receive ARV prophylaxis. This momentum is driven by increased funding by GON and partners, better coordination and accountability and look set to continue. | Table 2: Trend of key PMTCT indicators by year in the Nigerian PMTCT program
Click here to view |
| Challenges and Opportunities | | |
The PMTCT program in Nigeria is confronted with series of challenges that have affected its success. The Nigerian PMTCT program started in tertiary institutions as a pilot program, which would be decentralized to secondary hospitals and then to PHCs. This decentralization has been slow for a variety of reasons which include:
- Poor buy-in at the state and local government levels;
- Weak health systems;
- Human resource limitations particularly in rural areas;
- Low utilization of maternal and child health-care services.
Several other challenges such as high fertility rate, low contraceptive prevalence rate and a strong culture of breastfeeding with very low rates of exclusive breast feeding before 6 months have also plagued the program resulting in poor population coverage. Non-involvement of the private sector, which is a big player in the provision of health service in Nigeria is another reason for the poor program impact.
Overcoming these challenges will require much political will and strategic commitment of national, state and local government resources and international support to addressing these problems. The cost of indecision, inaction and delay in program acceleration is high, as every pediatric HIV infection that is not averted increases the ultimate economic and social cost to each family, community and country. The current international focus on Nigeria and the readiness to assist the county in scaling up PMTCT services is an opportunity that Nigeria must leverage on in order to meet its target of eliminating MTCT by 2015.
| Birth of Journal of HIV and Human Reproduction | | |
To facilitate the dissemination of research work in HIV medicine from Nigeria and other developing countries, the PMTCT NTT after several months of planning, enthusiastically presents the maiden issue of Journal of HIV and Human Reproduction. It is an international peer reviewed journal published by one of the world's renowned open access publishers - Medknow (part of Wolters Kluwer Health).
The Journal publishes contributions in English from all fields of HIV Medicine (Counseling, testing, treatment and care, prevention, support, behavior change, impact, stigma, discrimination, adherence, faith-based approaches, evidence-based interventions, structural and environmental interventions, funding and policy issues, etc.) and the impact of HIV on Human Reproduction including elimination of MTCT strategies, method of conception, fertility issues, pregnancy outcomes and infant feeding practices.
This maiden issue is global on contributors, reviewers and indeed contents.
| Conclusions | | |
The persisting high burden of HIV infected pregnant women and MTCT in the country is an indication of the need to urgently scale-up the PMTCT program and make the services accessible to all women especially those in the rural areas. Pre-service training curricula for all relevant cadres of health-care workers should be revised to include the knowledge and competences required for the provision of PMTCT services. Strategies that improve utilization of health services by rural dwellers should be promoted.
| References | | |
| 1. | United Nations Population Fund (UNFPA). State of World Population 2010. New York: UNFPA; 2010. 
|
| 2. | National Population Commission (Nigeria) and ICF Macro. Nigeria Demographic and Health Survey 2009. Abuja, Nigeria: National Population Commission and ICF Macro; 2009.
|
| 3. | Federal Ministry of Health. A Directory of Health Facilities in Nigeria 2011. Abuja, Nigeria: Federal Ministry of Health; 2011.
|
| 4. | Federal Ministry of Health (FMOH). National HIV sero-prevalence sentinel survey among pregnant women attending antenatal clinics in Nigeria. Technical Report 2010. Abuja: FMOH; 2010.
|
| 5. | National Agency for the Control of AIDS (NACA). Update on National Response to the HIV/AIDS Epidemic. Abuja: National Agency for the Control of AIDS; 2007.
|
| 6. | Burr CK, Lampe MA, Corle S, Margolin FS, Abresh C, Clark J, et al. An end to perinatal HIV: Success in the US requires ongoing and innovative efforts that should expand globally. J Public Health Policy 2007;28:249-60.
|
| 7. | Royal College of Obstetricians and Gynaecologists. Management of HIV in pregnancy. Guideline No. 39. London: RCOG; 2004.
|
| 8. | Mofenson LM. Prevention in neglected subpopulations: Prevention of mother-to-child transmission of HIV infection. Clin Infect Dis 2010;50 Suppl 3:S130-48.
[PUBMED] |
| 9. | Federal Ministry of Health, Nigeria. Scale - Up plan on prevention of mother to child transmission (PMTCT) of HIV in Nigeria. Abuja: Federal Ministry of Health; 2005.
|
| 10. | Dabis F, Leroy V, Castetbon K, Spira R, Newell ML, Salamon R. Preventing mother-to-child transmission of HIV-1 in Africa in the year 2000. AIDS 2000;14:1017-26.
|
| 11. | Dabis F, Ekpini ER. HIV-1/AIDS and maternal and child health in Africa. Lancet 2002;359:2097-104.
[PUBMED] |
| 12. | UNAIDS. Global plan towards the elimination of new HIV infections among children by 2015 and keeping their mothers alive. Countdown to Zero. Geneva, Switzerland: UNAIDS; 2011.
|
| 13. | Federal Ministry of Health. National scale up plan towards elimination of mother-to-child transmission of HIV in Nigeria 2010-2015. Abuja, Nigeria: Federal Ministry of Health; 2010.
|
| 14. | World Health Organization. Strategic approaches to the prevention of HIV infection in infants: Report of a WHO meeting. Morges, Switzerland: WHO; 2002, 2003.
|
| 15. | Federal Ministry of Health, Nigeria. National Guidelines on Prevention of Mother to Child Transmission (PMTCT) of HIV in Nigeria. Abuja: Federal Ministry of Health; 2001.
|
| 16. | Federal Ministry of Health, Nigeria. National Guidelines on Prevention of Mother to Child Transmission (PMTCT) of HIV in Nigeria. Abuja: Federal Ministry of Health; 2005.
|
| 17. | Federal Ministry of Health, Nigeria. National Guidelines on Prevention of Mother to Child Transmission (PMTCT) of HIV in Nigeria. Abuja: Federal Ministry of Health; 2007.
|
| 18. | Federal Ministry of Health, Nigeria. National Guidelines for Prevention of Mother-to-Child Transmission of HIV. 4 th ed. Abuja: Federal Ministry of Health; 2010.
|
| 19. | Federal Ministry of Health, Nigeria. National standard operating procedures for prevention of mother to child transmission (PMTCT) of HIV. Abuja: Federal Ministry of Health; 2007.
|
| 20. | Federal Ministry of Health, Nigeria. Prevention of Mother to Child Transmission (PMTCT) of HIV-Nigeria Curriculum, Participants's Manual. Abuja: Federal Ministry of Health; 2006.
|
| 21. | Federal Ministry of Health, Nigeria. Prevention of Mother to Child Transmission (PMTCT) of HIV-Nigeria Curriculum, Trainer's Manual. Abuja: Federal Ministry of Health; 2006.
|
| 22. | Federal Ministry of Health, Nigeria. Update of the PMTCT MIS for 2012. Presentation at the March 2013 PMTCT task team meeting. Abuja: Federal Ministry of Health; 2013.
|
| 23. | UNAIDS. Global Report: UNAIDS Report on the Global AIDS Epidemic. Geneva: UNAIDS; 2012.
|
| 24. | Inter-agency Task Team on the Prevention of HIV Infection in pregnant women, Mothers and Children. IATT dashboard for monitoring progress towards elimination of mother-to-child transmission goals. New York: IATT; 2012.
|
| 25. | Federal Ministry of Health. National health sector strategic plan and implementation plan for HIV/AIDS 2010-2015. HIV/AIDS Division. Abuja, Nigeria: Department of Public Health, Federal Ministry of Health; 2010.
|
[Table 1], [Table 2]
|








 Search Pubmed for
Search Pubmed for