|
 
 |
| ORIGINAL ARTICLE |
|
| Year : 2015 | Volume
: 1
| Issue : 1 | Page : 7-12 |
|
Evaluating Dietary Perceptions Education Program among Rural Hypertensive Patients on Commitment and Adherence to Healthy Diet
Aziz Kamran1, Aliakbar Shekarchi1, Gholamreza Sharifirad2, Elham Sharifian3, Leila Shekarchi1
1 Department of Public Health, Khalkhal Faculty of Medical Sciences, Ardabil University of Medical Sciences, Ardabil, Iran
2 Department of Health Education and Promotion, School of Health, Qom University of Medical Sciences, Qom, Iran
3 Department of Health Education and Promotion, Khalkhal Faculty of Medical Sciences, Ardabil University of Medical Sciences, Ardabil, Iran
| Date of Web Publication | 10-Aug-2015 |
Correspondence Address:
Prof. Gholamreza Sharifirad
Department Health Education and Promotion, School of Health, Qom University of Medical Sciences, Qom
Iran
 Source of Support: None, Conflict of Interest: None  | Check |

Background: A healthy diet has beneficial effects on reducing risk factors for cardiovascular diseases. This study was aimed to determine the effect of theoretical educational program on commitment and adherence to healthy diet in rural hypertensive patients. Methods: This quasi-experimental study was conducted on 138 hypertensive patients (68 in the intervention group and 70 in the control group) those referred to Ardabil rural health centers during 2013. The data were collected by a validated and reliable questionnaire. The pretest and posttest had an interval of 2 and 6 months. Health promotion model was used as a theoretical framework to explain the motivation of a behavior. Descriptive analysis, repeated measure, t-test, and T-paired with SPSS-18 were used to analyze data. Results: After intervention, knowledge scores, health promotion model constructs, and follow-up score increased significantly in the intervention group compared to the control group (P < 0.001). In contrast, perceived barriers reduced in the intervention group compared to the control group (P < 0.001). Conclusions: Educational intervention provided based on Pender's health promotion model had a beneficial effect on commitment and adherence to healthy diet. Keywords: Adherence, behavior, blood pressure, dietary, education, health promotion model, perception
How to cite this article:
Kamran A, Shekarchi A, Sharifirad G, Sharifian E, Shekarchi L. Evaluating Dietary Perceptions Education Program among Rural Hypertensive Patients on Commitment and Adherence to Healthy Diet. J Hum Health 2015;1:7-12 |
How to cite this URL:
Kamran A, Shekarchi A, Sharifirad G, Sharifian E, Shekarchi L. Evaluating Dietary Perceptions Education Program among Rural Hypertensive Patients on Commitment and Adherence to Healthy Diet. J Hum Health [serial online] 2015 [cited 2018 Aug 21];1:7-12. Available from: http://www.jhhjournal.org/text.asp?2015/1/1/7/162520 |
| Introduction | |  |
High blood pressure is the major cause of cardiovascular disease worldwide and there is a linear correlation between high blood pressure and cardiovascular diseases. [1] High systolic blood pressure (SBP) has been recognized responsible for most deaths in all regions of Iran [2] and according to Chaman et al. [3] and Faramarzi et al. [4] studies, the prevalence of hypertension in rural area is higher than urban in Iran. Several meta-analyses, interventional and epidemiological studies suggest that some dietary patterns and nutrition elements play a critical role in developing hypertension. In contrast, a healthy diet has positive effects on reducing risk factors for cardiovascular diseases. [5] Nutrition strategies are reduced sodium intake, limited alcohol intake, increased potassium intake, and following patterns like Dietary Approach to Stop Hypertension (DASH). [6] The DASH approach is a clear evidence of the effectiveness of short-term interventions. Recent studies show that the risk of cardiovascular disease in people with low-sodium intake treatment dropped as much as 25% [7] and the study carried out by Nowson on DASH approach showed that its effect on lowering blood pressure is stronger than the low-fat diet. [8] In another study, the SBP and diastolic blood pressures significantly lowered through the approach. [9]
A better adherence to the approach leads to reduced blood pressure, [10] but evidences showed that adherence to DASH recommendations is in low rates. [11] The adherence rate of the DASH diet among the study sample was 6 out of 10 [10] and in the study by Racine et al. [12] and Troyer et al. [13] the adherence rate was 2 out of 9.
Evidences showed that increasing the patient's motivation to adhere to dietary recommendations can lead to greater adherence to them. [10] In similar studies, self-efficiency (the perceived ability to adhere to recommendations), self-monitoring, emotions, and attending training sessions have been cited as predictors of adherence to the DASH approach. [14],[15] Another factor affecting adherence to the DASH approach include perceived barriers to dietary adherence, perceived benefits, perceived low social support, anxiety, depression, social conditions, low efficacy, [10] and negative previous experience. [16] Cultural influences are cited as another factor affecting adherence to the DASH approach. [16],[17] Hence, to achieve successful intervention in patients, nutritional factors affecting adherence shall be considered. In this study, Pender's health promotion model was used to study its effect on psychosocial factors and increased adherence which is similar to the majority of the cases in previous studies. Pender et al. (2011) explains this model as a framework and a guide for discovering complex psychological processes, which motivates individuals to change their behavior, and leads them to the promotion of health and hygiene. In addition to internal cognitive processes, this pattern investigates other effective factors on the behavior of individual including interpersonal relation and situational effects and individuals' previous experiences concerning the behavior which seems to be recommended for diet behavior of patients suffering from high blood pressure with various experiences of preserving the recommended diet. The structures of this model include self-efficacy, perceived benefits and barriers, affects related to behavior, interpersonal influences, situational influences, commitment toward the behavior, preferences, and immediate competitors. [18]
Many studies have used the DASH approach for nutrition education, but to our knowledge, this is the first interventional study on education about perceptions of hypertensive patients based on Pender's health promotion model. Another reason to perform this research was that very little educational intervention was reported on rural hypertensive patients. Considering the importance of nutrition and to increase the motivation of hypertensive patients to adhere to the recommendations for lowering their blood pressure, this study was carried out aiming to determine the effectiveness of education on the degree of commitment and adherence to the healthy diet.
| Methods | | |
This research was a controlled quasi-experimental pretest/posttest study. The study was supported, funded, and approved by Isfahan University of Medical Sciences Institutional Review Board No: 392132. The statistical population included hypertensive patients in rural health centers in Ardabil in 2013 with a multi-stage random sampling method, and 140 people were selected (70 as case, and 70 as control) based on repeated measure sampling formula (v = 1, w = 2, ρ =0.6, α =0.05). During the study, two patients were excluded from the case group because of immigration. To select samples, the 4 rural health centers were randomly selected in the first stage. Then 2 centers were randomly assigned to the treatment group and 2 centers were used as control group. In the third stage in each center, the samples were randomly selected among patients with systolic blood pressure (SBP) ≥140 mm Hg or diastolic blood pressure ≥90 mm Hg. Other inclusion criteria were age range of 30-65, tendency for conscious participation and the ability to read and write and exclusion criteria include suffering from complications of hypertension, need for another special diet for any reason, other medical conditions. The data were collected using interviews before treatment and in follow-up periods 2 and 6 months after the intervention by trained personnel who were trusted by the patients. The designed education included motivational advices based on HPM in 6 group teaching sessions (2 sessions/week). For the convenience of the patients and to increase their participation, the sessions were held in selected rural health centers.
At the first and in the end of the last session, behavioral commitment of the patients to adhere to dietary recommendations was emphasized. All patients were verbally committed to adhere to dietary instructions and in this regard and for strengthening of commitment, monthly educational pamphlet, and booklets were distributed among the patients. The entire educational program provided by AK (PhD in Health Promotion). For ethical considerations, after completing the study, the instruction booklets were also distributed among the control group.
A questionnaire with nine sections was used for data collection: (1) Demographic specification questions, (2) perceived benefits (nine questions in the form of two ranges based on Likert attitude scale (completely agree, agree, disagree, and completely disagree) which were given 1-4 scores), (3) Perceived barriers (ten questions in the form of two ranges based on Likert attitude questionnaire (completely agree, agree, disagree, completely disagree) which were given 1-4 scores), (4) Self-efficacy (10 questions based on a 10 item scale which were given 1-10 scores), (5) Affects related to behavior (eight questions based on 5-point Likert attitude scale (always, usually, often, rarely, never) which were given 1-5 scores), (6) Interpersonal influences (nine questions based on 5-rank scale investigating social support of spouse, which were given 1-5 scores), (7) Situational influences (seven 5-scale questions including always, usually, often, rarely, and never) which were given 1-5 scores 8. Commitment to the plan (nine questions based on 5-point scale (always, usually, often, rarely, and never) which were given 1-5 scores). The face validity of the questionnaire was confirmed by content validity ration and content validity index. The reliability of the questionnaire was calculated through internal homogeneity and Cronbach's alpha and the values of these coefficients for every structure were calculated. The highest alpha was related to perceived self-efficacy (0.96), while the lowest was related to perceived benefits (0.85). Other values were 0.92, 0.86, 0.85, and 0.89 for perceived barriers, affects related to behavior, commitment to plan, interpersonal, and situational influences, respectively.
Data were analyzed using SPSS software version 18.0 (SPSS Inc., Chicago, IL, USA). Student's t-test was used to compare the values between the two groups before and after the intervention. The mean differences of variables were compared by paired t-test and repeated measures analysis of variance was used to test the group for the effects of time. P < 0.05 was considered significant.
| Results | | |
The mean age of patients participating in the case group was 49.6 years and in the control group was 50.9 years. There was no significant difference in the mean age, mean duration of disease, education level, and gender of the patients in both groups [Table 1]. The mean knowledge score before intervention was 11.9 ± 3.7 in the case group and it was 12.3 ± 3.5 in the control group, and there was no significant difference between the two groups. However, 2 and 6 months after the intervention, a significant difference was found in the mean changes of knowledge among the two groups. Repeated measuring tests showed that the intervention had a significant effect on knowledge changes in the case group over time (P < 0.001) and the knowledge significantly increased. The mean scores of perceived benefits before intervention were 28.8 ± 4.4 in the case group and it was 28.4 ± 4.3 for the control group, which shows that there is no significant difference between the two groups. However, 2 and 6 months after intervention, the two groups had statistically significant differences. Repeated measure test showed that the intervention had a significant effect (P < 0.001) and it increased, but the changes in the perceived benefits before the intervention were not significant in the control group over time (P = 0.053). The mean score of the perceived benefits in the case group was 26.6 ± 3.9 and it was 28.4 ± 5.4 in the control group. However, 2 and 6 months after the intervention, the difference between the two groups was significantly different. Repeated measure test showed that the intervention had a significant effect (P < 0.001).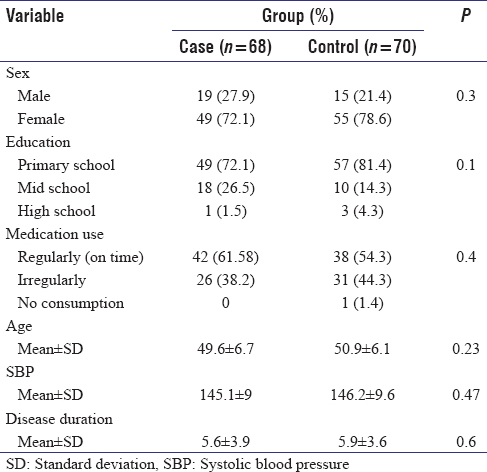 | Table 1: Demographic Characteristics of Hypertensive Patients in the Case and Control Groups
Click here to view |
There was no significant difference between the mean scores of the two groups' efficacy before the intervention. However, the mean difference of perceived self-efficiency score between the two groups 2 and 6 months after the intervention was significantly different and the intervention had a significant effect on the perceived self-efficiency changes in the case group over time (P < 0.001) and it increased, but changes in the perceived self-efficiency in the control group was not significant over time (P = 0.93) [Table 2].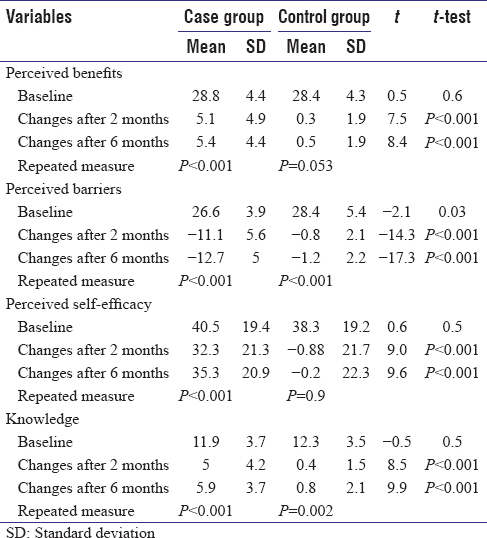 | Table 2: Mean of Perceived Benefits and Barriers, Self-efficacy and Knowledge in Case and Control Group before and after Intervention
Click here to view |
Before the instruction intervention, no significant difference was observed between the mean scores of interpersonal and situational influences in the control and case groups. However, 2 and 6 months after the intervention, there was a significant difference between the mean score changes of the two groups and the intervention had a significant effect on the perceived self-efficiency changes in the case group (P < 0.001) and it increased over time, but these changes were not significant in the control group over time. There was also no significant difference in mean scores related to the feelings about the previous behavior and commitment of the two groups before the intervention. However, 2 and 6 months after the intervention, there was a significant difference between the changes in the mean scores of the two groups at these points. The repeated measure test showed that education intervention had a significant effect on the feeling changes related to behavior and commitment to diet in the case group over time (P = 0.001) and it increased, but the changes in the control group was not significant over time.
The mean follow-up score before the intervention was 15.4 ± 5.5 in the case group and it was 15.0 ± 6.1 in the control group with no significant difference between the two groups. However, 2 and 6 months after the intervention, there was a significant difference between the mean changes of the two groups, and repeated measure test showed that education intervention had a significant effect (P < 0.001) [Table 3].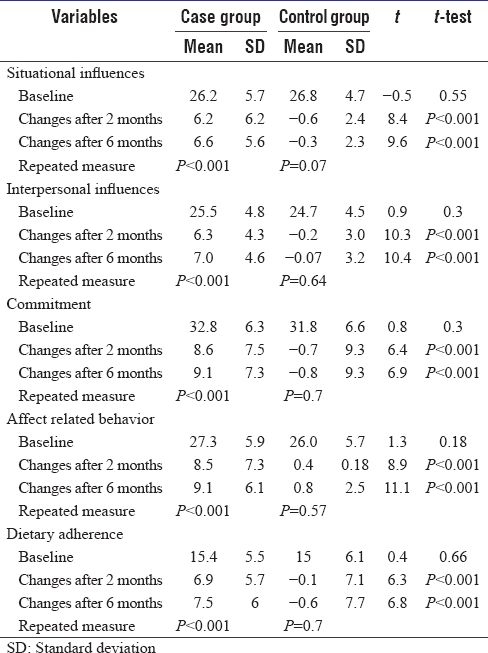 | Table 3: Mean of Situational and Interpersonal Influences, Commitment and Adherence in Case and Control Group before and after Intervention
Click here to view |
| Discussion | | |
According to the findings during this research, this is the first study on nutrition education using the DASH approach in the form of Pender's health promotion model constructs in patients with hypertension, especially rural patients and it offers useful information particularly for researchers and health care providers in Iran. In this study, regarding the maximum score, it can be said that patients had a moderate level of knowledge and this is in line with the studies by Kamran et al. [19] and Sabouhi et al. [20] concluding that patients' knowledge was moderate, but in the another study patients had poor nutritional knowledge [21] so that based on reports, one of the factors resulting to the lack of control of this disease was low level of knowledge. [20] Low nutrition knowledge was an obstacle for observing recommended diet in DASH approach in the study by Spencer. [22] The lack of accurate information in the rural areas is concerning. [23]
Knowledge plays an important role in the nutrition of hypertension patients. [24] In the study by Kamran et al., there is a significant inverse relationship between knowledge and sodium intake, and this association is stronger in the controlled hypertensive group. The knowledge and understanding of the disease could predict 17% and 46.2% of the variation in sodium intake of the treatment group and the control group, respectively. [19] After the education intervention, the treatment patients' knowledge significantly increased (5.9 scores), while these changes were not observed in the control group (0.8 score). This result is consistent with the results of the study by Magadza et al. [25] and the study by Pandey et al., which indicated a significant increase in nutritional knowledge of the patients after the intervention. [26]
The mean score of the perceived benefits regarding the maximum score, is higher than average. The mean score of the perceived barriers regarding the maximum score can also be convincing to say that the score of perceived barriers is higher than average. High mean score of the perceived benefits is perhaps a positive sign of willingness to respect and adhere to the diet. In the study by Pires et al., overcoming beliefs in the identified benefits is an indication of positive predictions about adherence to a diet introduced healthy. [27] In the study by Pawlak et al., people received low scores on all items related to barriers of healthy eating. These scores were lower than the scores for benefits of a healthy diet. [28] Perceived benefits were suggested as important factors affecting the intake of fruits and vegetables. [28]
Perceived benefits and barriers are two structures explaining behavior in certain patterns of behavior change, in fact explaining the action of the people by the balance or imbalance between the perceived positive and negative behaviors regarding health. As a result, people perform a behavior or refuse it based on the review and analysis of the benefits subtracted from barriers. [29] In the study by Kamran et al., sodium intake had a reverse relationship with perceived benefits and had a significant direct relationship with perceived barriers. This means that by increasing perceived benefits, the sodium intake decreased, and by increasing perceived barriers, the sodium intake decreased. According to the perceived barriers by the study samples, the most important perceived barriers included: Difficulty of separate preparation of low-salt meals, the exclusion of certain foods tastes, boring diet and being limited in parties, and the high cost of diet food. [30]
The mean score of the perceived benefits increased significantly after the education intervention; however, the perceived benefits changes in the control group were not significant over time. In the study by Park et al., after the instruction of nutritional intervention on hypertension, the perceived benefits increased significantly. [31] Changes in the perceived barriers were significantly lower in the treatment group after the intervention. In the study by Park et al., after the intervention, the perceived barriers to hypertension significantly decreased. [31] Given the importance of perceived barriers to health-promoting behaviors, it is expected that adopting the behavior through the reduction of perceived barriers, and the increase of perceived benefits is increased.
In this study, the mean score on perceived self-efficacy was below from average. These finding is inconsistent with the studies by Paryad et al. [32] and the study by Warren-Findlow et al. indicating that the efficacy of hypertension self-care was desirable. However, these studies suggest the need for education intervention to increase self-efficacy. [33] Self-efficacy is affected by factors such as age, gender, education, region of residence and access to care and services. [32] This inconsistency may be justifiable for the rural samples in this study and greater number of women compared to men as well as a low level of the education of the samples.
In the present study, intervention in perceived self-efficacy had a significant effect on changes in the intervention group and self-efficacy significantly increased over time. Increased self-efficacy will increase the likelihood of behavior and success in it. [34] In intervention studies, with increased efficacy, the onset and maintenance of the behavior becomes stronger and more stable and there is generally a strong relationship between self-efficacy and achievement in changing a behavior. [35]
Social influences and influencing people who influence others including family members have been identified among facilitating and inhibiting factors in blood pressure control. [36],[37] Family members play a critical role on the self-care of hypertensive patients suffering. These roles can include assisting in the selection and preparation of food, [38] assisting in understanding and adherence to recommendations, [37] support in adherence to the diet, [39] as well as encouraging behavior change. [37] In the study by Wilson et al., people who had received more psychological support from family members, had greater adherence to the diet and limited salt in their diet. [38]
In this study, the effects of patients showed significant improvements with respect to eating behavior. Emotions play an important role in patients' adherence to nutritional recommendations. The study by Keshani and Farvid, fatigue resulted by long-term adherence to diet, laziness and impatience, incorrect beliefs, ignorance, and stubbornness were among the obstacles mentioned for the intake of the food containing enough fiber. [40] From among perceived barriers to diet control, frustration in controlling the disease could be mentioned. Patients routinely do not adhere to dietary recommendations and they are disappointed by failure in controlling the disease. [40]
In this study, patients' adherence to the diet was moderate. Various studies have used different criteria to assess adherence to nutrition. In this study, in addition to the mean score of nutrition adherence, the blood pressure of the patients was also used to evaluate patients' adherence. A significant increase in the nutritional follow-up of the patients and a significant decrease in SBP and diastolic blood pressures were observed. In a review study, the results of 123 instructions on nutritional intervention were examined for the prevention and control of chronic diseases, and of these, only 32 studies reported favorable changes in adherence to the diet. Using various teaching techniques and providing feedback on training sessions, creating commitment, and contract with the patient were mentioned as the reasons for the success of these studies. [41] Evaluating the nutritional status of the patients with hypertension on the basis of compliance with the DASH score in a 16-year follow-up period on over 4386 patients showed that the compliance rate is declining and it showed that few patients observe consuming total fat, saturated fat, and magnesium. [42]
Limitations
The intervention effects obtained in the study might not be applicable to the general population especially for residents in urban areas. Second, this was only a 6-month follow-up study. This study subjects will need to be followed up in the future to examine the long-term effect of the nutrition health education program on blood pressure. Another limitation is that in this study, patients were not separated in a prior hypertension group and a group with no pharmacologic treatment. Finally, biochemical parameters were not measured in this study that could help to explain differences between controls and cases.
In contrast, the optimal sample size and the standard tools are the strengths of this study. The other strength, according to our knowledge, this is the first study have been done on the rural hypertensive patients in Iran.
| Conclusion | | |
Educational intervention provided based on Pender's health promotion model had a beneficial effect on patients' perception, commitment and adherence to the recommended dietary behavior in rural patients of this study. Further study should be emphasized on the degree or the type of physical activity and the specific items of vegetables and fruits to evaluate their effects on reducing blood pressure. Due to the lack of information available on the nutritional status and self-care in hypertensive patients especially in rural patients in Iran and other developing countries, additional researches into the determinants of eating behavior in this population will play an important role in helping to control hypertension.
Financial support and sponsorship
This is extracted from PhD thesis.
Conflicts of interest
There are no conflicts of interest.
| References | | |
| 1. | Lee DS, Massaro JM, Wang TJ, Kannel WB, Benjamin EJ, Kenchaiah S, et al. Antecedent blood pressure, body mass index, and the risk of incident heart failure in later life. Hypertension 2007;50:869-76.  |
| 2. | Fallah Z, Qorbani M, Motlagh ME, Heshmat R, Ardalan G, Kelishadi R. Prevalence of prehypertension and hypertension in a nationally representative sample of iranian children and adolescents: The CASPIAN-IV Study. Int J Prev Med 2014;5 Suppl 1:S57-64. |
| 3. | Chaman R, Yunesian M, Hajimohamadi A, Gholami Taramsari M. Investigating hypertension prevalence and some of its influential factors in an ethnically variant rural sample. Knowl Health 2008;3:39-42. |
| 4. | Faramarzi H, Bagheri P, Bahrampour A, Halimi L, Rahimi N, Ebrahimi M. The comparison of prevalence of diabete and hypertension between rural areas of fars and rural area of EMRO region. Iran J Endocrinol Metab 2011;13:157-64. |
| 5. | Azadbakht L, Fard NR, Karimi M, Baghaei MH, Surkan PJ, Rahimi M, et al. Effects of the Dietary Approaches to Stop Hypertension (DASH) eating plan on cardiovascular risks among type 2 diabetic patients: A randomized crossover clinical trial. Diabetes Care 2011;34:55-7. |
| 6. | Bazzano LA, Green T, Harrison TN, Reynolds K. Dietary approaches to prevent hypertension. Curr Hypertens Rep 2013;15:694-702. |
| 7. | Cook NR. Salt intake, blood pressure and clinical outcomes. Curr Opin Nephrol Hypertens 2008;17:310-4. |
| 8. | Nowson CA, Worsley A, Margerison C, Jorna MK, Godfrey SJ, Booth A. Blood pressure change with weight loss is affected by diet type in men. Am J Clin Nutr 2005;81:983-9. |
| 9. | Nowson CA, Wattanapenpaiboon N, Pachett A. Low-sodium Dietary Approaches to Stop Hypertension-type diet including lean red meat lowers blood pressure in postmenopausal women. Nutr Res 2009;29:8-18. |
| 10. | Epstein DE, Sherwood A, Smith PJ, Craighead L, Caccia C, Lin PH, et al. Determinants and consequences of adherence to the dietary approaches to stop hypertension diet in African-American and white adults with high blood pressure: Results from the ENCORE trial. J Acad Nutr Diet 2012;112:1763-73. |
| 11. | Kwan MW, Wong MC, Wang HH, Liu KQ, Lee CL, Yan BP, et al. Compliance with the Dietary Approaches to Stop Hypertension (DASH) diet: A systematic review. PLoS One 2013;8:e78412. |
| 12. | Racine E, Troyer JL, Warren-Findlow J, McAuley WJ. The effect of medical nutrition therapy on changes in dietary knowledge and DASH diet adherence in older adults with cardiovascular disease. J Nutr Health Aging 2011;15:868-76. |
| 13. | Troyer JL, Racine EF, Ngugi GW, McAuley WJ. The effect of home-delivered Dietary Approach to Stop Hypertension (DASH) meals on the diets of older adults with cardiovascular disease. Am J Clin Nutr 2010;91:1204-12. |
| 14. | Tinker LF, Rosal MC, Young AF, Perri MG, Patterson RE, Van Horn L, et al. Predictors of dietary change and maintenance in the Women′s health initiative dietary modification trial. J Am Diet Assoc 2007;107:1155-66. |
| 15. | Burke LE, Wang J, Sevick MA. Self-monitoring in weight loss: A systematic review of the literature. J Am Diet Assoc 2011;111:92-102. |
| 16. | Airhihenbuwa CO, Kumanyika S, Agurs TD, Lowe A, Saunders D, Morssink CB. Cultural aspects of African American eating patterns. Ethn Health 1996;1:245-60. |
| 17. | Williams JH, Auslander WF, de Groot M, Robinson AD, Houston C, Haire-Joshu D. Cultural relevancy of a diabetes prevention nutrition program for African American women. Health Promot Pract 2006;7:56-67. |
| 18. | Pender NJ, Murdaugh CL, Parsons MA. Health Promotion in Nursing Practice. 6 th ed. Boston, MA: Pearson; 2011. |
| 19. | Kamran A, Azadbakht L, Sharifirad G, Mahaki B, Sharghi A. Sodium intake, dietary knowledge, and illness perceptions of controlled and uncontrolled rural hypertensive patients. Int J Hypertens 2014;2014:245480. |
| 20. | Sabouhi F, Babaee S, Naji H, Zade AH. Knowledge, Awareness, Attitudes and practice about hypertension in hypertensive patients referring to public health care centers in khoor and biabanak 2009. Iran J Nurs Midwifery Res 2011;16:35-41. |
| 21. | Nkosi NG, Wright SC. Knowledge related to nutrition and hypertension management practices of adults in Ga-Rankuwa day clinics. Curationis 2010;33:33-40. |
| 22. | Spencer A, Jablonski R, Loeb SJ. Hypertensive African American women and the DASH diet. Nurse Pract 2012;37:41-6. |
| 23. | Li X, Ning N, Hao Y, Sun H, Gao L, Jiao M, et al. Health literacy in rural areas of China: Hypertension knowledge survey. Int J Environ Res Public Health 2013;10:1125-38. |
| 24. | Ford CD, Kim MJ, Dancy BL. Perceptions of hypertension and contributing personal and environmental factors among rural Southern African American women. Ethn Dis 2009;19:407-13. |
| 25. | Magadza C, Radloff SE, Srinivas SC. The effect of an educational intervention on patients′ knowledge about hypertension, beliefs about medicines, and adherence. Res Social Adm Pharm 2009;5:363-75. |
| 26. | Pandey RM, Agrawal A, Misra A, Vikram NK, Misra P, Dey S, et al. Population-based intervention for cardiovascular diseases related knowledge and behaviours in Asian Indian women. Indian Heart J 2013;65:40-7. |
| 27. | Pires CG, Mussi FC. Health beliefs regarding diet: A perspective of hypertensive black individuals. Rev Esc Enferm USP 2012;46:580-9. |
| 28. | Pawlak R, Colby S. Benefits, barriers, self-efficacy and knowledge regarding healthy foods; perception of African Americans living in eastern North Carolina. Nutr Res Pract 2009;3:56-63. |
| 29. | Mohebi S, Sharifirad G, Feizi A, Botlani S, Hozori M, Azadbakht L. Can health promotion model constructs predict nutritional behavior among diabetic patients? J Res Med Sci 2013;18:346-59. [ PUBMED]  |
| 30. | Kamran A, Sharifirad G, Azadbakht L. Assessing Nutritional Behaviors and Attitudes of Rural Hypertensive Patients Based on Pender Health Promotion Model. Ardabil: Ardabil University of Medical Sciences; 2013. |
| 31. | Park S, Kwon J, Kim C, Lee Y, Kim H. Development of nutrition education program for hypertension based on health belief model, applying focus group interview. Korean J Community Nutr 2012;17:623-36. |
| 32. | Paryad E, Hosseinzade T, Kazemnejad E, Asiri S. A study of self-efficacy in patients with coronary artery disease and its predictors. Qom Univ Med Sci J 2013;7:41-8. |
| 33. | Warren-Findlow J, Seymour RB, Brunner Huber LR. The association between self-efficacy and hypertension self-care activities among African American adults. J Community Health 2012;37:15-24. |
| 34. | Mularcik K. Self-Efficacy Toward Health Behaviors to Improve Blood Pressure in Patients who Receive Care in a Primary Care Network: The Ohio State University; 2010. |
| 35. | Strecher VJ, DeVellis BM, Becker MH, Rosenstock IM. The role of self-efficacy in achieving health behavior change. Health Educ Q 1986;13:73-92. [ PUBMED] |
| 36. | Khatib R, Schwalm JD, Yusuf S, Haynes RB, McKee M, Khan M, et al. Patient and healthcare provider barriers to hypertension awareness, treatment and follow up: A systematic review and meta-analysis of qualitative and quantitative studies. PLoS One 2014;9:e84238. |
| 37. | Flynn SJ, Ameling JM, Hill-Briggs F, Wolff JL, Bone LR, Levine DM, et al. Facilitators and barriers to hypertension self-management in urban African Americans: Perspectives of patients and family members. Patient Prefer Adherence 2013;7:741-9. |
| 38. | Wilson DK, Ampey-Thornhill G. The role of gender and family support on dietary compliance in an African American adolescent hypertension prevention study. Ann Behav Med 2001;23:59-67. |
| 39. | Trivedi RB, Ayotte B, Edelman D, Bosworth HB. The association of emotional well-being and marital status with treatment adherence among patients with hypertension. J Behav Med 2008;31:489-97. |
| 40. | Keshani P, Farvid M. Perceived benefits and barriers regarding high fiber food intake in type 2 diabetes patients - A qualitative study. Iran J Nutr Sci Food Technol 2012;7:11-22. |
| 41. | Desroches S, Lapointe A, Ratté S, Gravel K, Légaré F, Turcotte S. Interventions to enhance adherence to dietary advice for preventing and managing chronic diseases in adults. Cochrane Database Syst Rev 2013;2:CD008722. |
| 42. | Mellen PB, Gao SK, Vitolins MZ, Goff DC Jr. Deteriorating dietary habits among adults with hypertension: DASH dietary accordance, NHANES 1988-1994 and 1999-2004. Arch Intern Med 2008;168:308-14. |
[Table 1], [Table 2], [Table 3]
|









 Search Pubmed for
Search Pubmed for