|
 
 |
| ORIGINAL ARTICLE |
|
| Year : 2015 | Volume
: 1
| Issue : 2 | Page : 56-59 |
|
Tobacco Use among Adults and its Associated Factors in a Rural Area in Karnataka, India
B Bhavya, Catherin Nisha, S Ankit, EN Joseph, BK Anusha, P Omkar, CJ Navya, NS Deepthi, BR Goud
Department of Community Health, St. John's Medical College, Bengaluru, Karnataka, India
| Date of Web Publication | 22-Sep-2015 |
Correspondence Address:
Dr. Catherin Nisha
Department of Community Health, St. John's Medical College, Bengaluru, Karnataka
India
 Source of Support: Nil., Conflict of Interest: There are no confl icts of interest.  | Check |

Background: Tobacco use is a major preventable cause of premature death and disease, currently causing over 5 million deaths per year globally, accounting for 9% of annual deaths. We conducted this research to assess the prevalence of tobacco use and its associated factors, among adults in a rural area in Karnataka, India. Methods: It was a cross-sectional study conducted in a rural area of Bangalore Urban district Karnataka, India using systematic random sampling with a sample size of 295 adults. A door to door survey was conducted during July to August 2012, using a validated questionnaire adapted from Global Adult Tobacco Survey, India. Results: The study population comprised of 157 males (53%) and 138 females (47%). The prevalence of tobacco use was found to be 39.3% of which 17.3% were current tobacco smokers and 22% used smokeless form of tobacco. There was a significant association between smoking and age, literacy, and socioeconomic status. We found that 59% of smokers had attempted to quit in the past 12 months as compared to 44% in smokeless tobacco users. About 61% of current smokers who noticed health warnings on cigarette packs attempted to quit. Conclusion: Smoking form of tobacco use was higher among males and smokeless tobacco use was higher among females. Keywords: Global Adult Tobacco Survey, smoking, smokeless tobacco, tobacco
How to cite this article:
Bhavya B, Nisha C, Ankit S, Joseph E N, Anusha B K, Omkar P, Navya C J, Deepthi N S, Goud B R. Tobacco Use among Adults and its Associated Factors in a Rural Area in Karnataka, India. J Hum Health 2015;1:56-9 |
How to cite this URL:
Bhavya B, Nisha C, Ankit S, Joseph E N, Anusha B K, Omkar P, Navya C J, Deepthi N S, Goud B R. Tobacco Use among Adults and its Associated Factors in a Rural Area in Karnataka, India. J Hum Health [serial online] 2015 [cited 2018 Aug 21];1:56-9. Available from: http://www.jhhjournal.org/text.asp?2015/1/2/56/165910 |
| Introduction | |  |
Tobacco is a preparation of dried nicotine-rich leaves of a Native American plant used for smoking or chewing.[1] In India, tobacco is used two major forms smoking and smokeless which include beedi/biri, cigarette, e-cigarette, hookah, shisha, cigarillo, cigar, pipe, and kretek which are smoking forms and snuff, pan masala, gutkha, mishri, khaini, qiwam, mawa, and toothpaste which are smokeless forms.[2] There is no safe form of tobacco, all forms contain nicotine and can cause addiction or health problems. Tobacco use is a major preventable cause of premature death and disease, currently leading to over 5 million deaths annually worldwide, which is expected to rise to over 8 million by 2030.[3] Tobacco currently accounts for 9% of all deaths annually [4] and 4.1% disability adjusted life years lost every year due to tobacco use.[5] A vast majority of these deaths are projected to occur in developing countries. Nearly 800–900 thousand people die in India due to tobacco-related diseases.[6] The majority of the cardiovascular diseases, cancers, and chronic lung diseases are directly attributable to tobacco consumption. Every year, more than 5.5 trillion cigarettes are produced, enough to provide every person on earth with 1000 cigarettes. Worldwide 1.3 billion people smoked in 2003, a number that is projected to increase to 1.6 billion by 2030. According to the Global Adult Tobacco Survey (GATS) – India 2009–2010, 35% of the Indian population are current tobacco users and 28% in Karnataka state.[7] We conducted this research to assess the prevalence of tobacco use and its associated factors among adults in a rural area in Karnataka.
| Methods | | |
The present study was carried out in a rural area in Karnataka state. The area covered was the Mugalur sub-center in Bangalore Urban District comprising of 8 villages. These villages are situated about 50 km away from Bangalore city. A cross-sectional study was conducted between July and August 2012. The Mugalur sub-center has a total population of 5390 with a total of 1138 households. In order to cover all the villages under the sub-center, systematic random sampling was used. The total population was divided by the number of households, and we thus took every forth household as the sampling unit. One individual from each household was picked out by simple random sampling. The sampling unit was an adult of 15 years and above. Thefirst household to be surveyed was chosen by currency method. In case a household was found to be locked, it was made sure that household was revisited the next day. If it was still locked, the next household, which means the eighth house, was taken as the sampling unit. With regard to the individual interviewed, if it was found that he/she was not present, then that person would be revisited the following day. If still absent, another person chosen by simple random sampling would be interviewed from the same household. However, there were very few instances where the above-mentioned situation arose as the interview was conducted in the evenings when most individuals were present. A pretested and validated questionnaire adapted from GATS was used for the interview. Individuals who agreed to participate in the study were explained the nature and objectives of the study, and informed written consent was obtained. The sample size was calculated to be 292 individuals (P = 0.28 according to GATS – Karnataka 2009 survey,[8] with a relative precision of 5% with 95% confidence) for a finite population. A total of 295 individuals were interviewed. The data were entered in Microsoft Excel, and analyzed using SPSS version 17.0 (IBM Bangalore). Frequencies, mean, standard deviation, and Chi-square were calculated.
| Results | | |
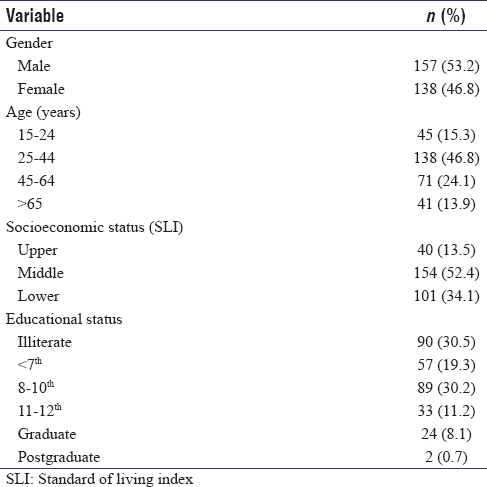
We interviewed 295 adults participants of which 157 (53.2%) were male and 138 (46.2%) female. The response rate was 100%. The sociodemographic characteristics of the study population is depicted in [Table 1], majority were in the age group 25–44 years (46.8%), Hindu by religion (92.5%), were married (80%), living in a nuclear family (48.6%), and belonged to middle class (52.4%) according to standard of living index tool.
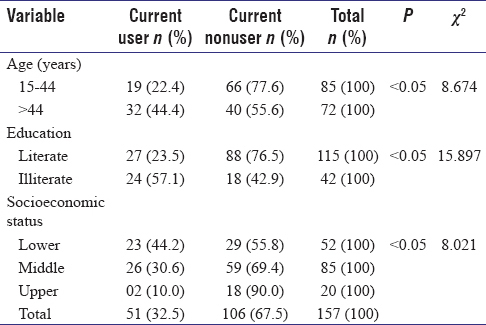
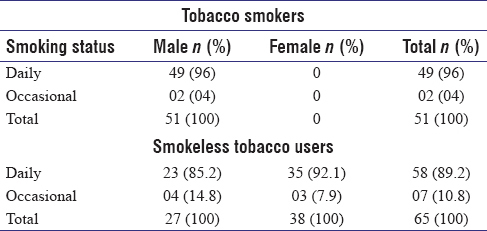
The overall prevalence of tobacco use was found to 39.3% with 17.3% of population using smoking tobacco and 22% being smokeless tobacco users. Among those who smoke tobacco, 96% smoke daily and 4% were occasional smokers [Table 2]. Tobacco smoking was significantly associated with older age group (>44 years, P < 0.05 χ2 = 8.674) and had a male predominance. There was statistically significant association between smoking status and education, more illiterate people were current smokers (P< 0.05 χ2 = 15.897) [Table 3]. Lower the socioeconomic status more is the tobacco smoking (P < 0.05 χ2 = 8.021) [Table 4]. Among smokeless tobacco users, 89.2% were daily users and 11.8% used occasionally. Exposure to secondhand smoke was found to be significantly higher among females (P < 0.05 χ2 = 4.625). Smokeless tobacco use was significantly higher in females (P< 0.05 χ2 = 4.570) and in illiterates (P < 0.05 χ2 = 16.142). Fifty-one percentage of current tobacco users had attempted to quit tobacco use in the past 12 months (59% smokers had tried to quit and 44.6% smokeless tobacco users had tried to quit). Fifty-seven percentage of the study population had noticed anti-cigarette information in newspapers or magazines, 61.7% on cigarette packs, and 82.7% on the television. 19.7% of the study population had noticed cigarette advertisement in stores. Of the 116 current tobacco users, 76 (65.5%) had visited a health care provider, and 72% of them had been advised to quit smoking. Among the tobacco users who had received advice to quit smoking, 55% attempted to quit smoking. 60.5% of current tobacco smokers who had noticed health warning on cigarette packs had attempted to quit in the past 12 months.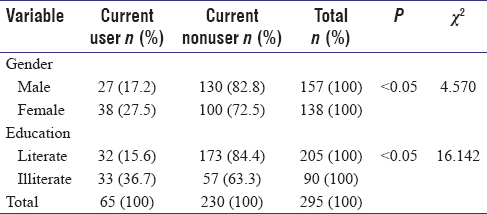 | Table 3: Factors associated with smoking tobacco use in the study population (n=295)
Click here to view |
 | Table 4: Factors associated with smokeless tobacco use in the study population (n=295)
Click here to view |
| Discussion | | |
The overall prevalence of current tobacco use was found to be 39.3% in our study, as compared to 30% in India and 21.9% in Karnataka.[9] The higher prevalence in our study area may be due to lack of education and awareness of ill effects of tobacco. In this study, the prevalence of smokeless form of tobacco use was 22%, which was higher than the smoking form (17.3%). A study conducted in the rural areas of Karnataka [10] in the year 2001, showed that 16.5% used smoking form of tobacco and 14.7% used smokeless form which is contradictory to our findings. The probable reason for this variation is that other study had a larger sample size and was conducted in 2001, there was increased awareness among public about smoking after the legislation was passed in 2004.[11] The higher prevalence of smokeless form of tobacco was probably because it was more socially accepted than smoking form.
We found that tobacco use, both smoking and smokeless form, was significantly associated with illiteracy, lower socioeconomic status, and older age groups. These findings are corroborated by other studies.[9],[12] These studies also showed that tobacco use was more prevalent in scheduled caste and scheduled tribes and also in Muslims. Number of school years also played an important part on tobacco use. A study conducted in Udupi district in Karnataka [13] also showed that tobacco use was more common in older persons, less educated, and lower socioeconomic group. Our study showed that among tobacco users, those who consulted a doctor or health care professional, and was advised to quit, were more likely to attempt quitting tobacco use in the past 12 months.
Noticing health warning on cigarette packs and other media were also instrumental in encouraging people to quit tobacco. We found out that anti-cigarette information was noticed more on the television rather than printed media. The reason could be that television is an audiovisual aid that can be used to convey messages even to the illiterate. 60.5% of current smokers who noticed health warnings on cigarette packs attempted to quit. This shows the effectiveness of health warnings in cigarette packs.
An alarmingly large proportion of the study population had noticed advertisements promoting the use of various tobacco products. This is a serious issue that has to be dealt with.
| Conclusions | | |
This study enumerates the prevalence of tobacco use among adults and its associated factors in a rural area in Karnataka, India. The smoking form of tobacco was exclusively used by males whereas more females used smokeless form as compared to males. A significant association was found between use of both forms of tobacco and education and socioeconomic status. Use of smoking form of tobacco was found to be more among older age group, whereas no such association was found with the use of smokeless form. More number of females was exposed to secondhand smoke at home as compared to males.
| Recommendations | | |
"Tobacco is the only legally available consumer product which kills people when it is used entirely as intended." The study conducted by us made us realize that steps needed to be taken to control the tobacco epidemic. On our part we can start by giving health education to the people about ill effects of tobacco, offer help, and counseling to those who want to quit and also protect those exposed to secondhand smoke at home or their workplace.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
| References | | |
| 1. | Stevenson A. The Little Oxford English Dictionary; 2008.  |
| 2. | |
| 3. | World Health Organization. Report on Global Tobacco Epidemic, The MPOWER Package. Geneva: World Health Organization; 2008. |
| 4. | Thomas AG, Michael G. Epidemiology of Cardiovascular Disease, Harrison's Principle of Internal Medicine. McGraw-Hill Medical: New York; 2012. |
| 5. | |
| 6. | Reddy KS, Gupta PC. Report on Tobacco Control in India. New Delhi: Ministry of Health and Family Welfare, Government of India; 2004. |
| 7. | Global Adult Tobacco Survey, India; 2009-2010. |
| 8. | Global Adult Tobacco Survey, Karnataka; 2009. |
| 9. | Rani M, Bonu S, Jha P, Nguyen SN, Jamjoum L. Tobacco use in India: Prevalence and predictors of smoking and chewing in a national cross sectional household survey. Tob Control 2003;12:e4. |
| 10. | Chaudhry K, Prabhakar AK, Prabhakaran PS, Prasad A, Singh K, Singh A. Prevalence of Tobacco Use in Karnataka and Uttar Pradesh in India – Final Report of the Study by the Indian Council of Medical Research and the WHO South East Asian Regional Office, New Delhi; 2001. |
| 11. | Anti Tobacco Legislation Passed in 2004 and National Tobacco Control Programme Piloted in 2007-08. |
| 12. | Kutty VR, Balakrishnan KG, Jayashree AK, Thomas J. Prevalence of coronary heart disease in the rural population of Thiruvananthapuram district, Kerala, India. Int J Cardiol 1993;39:59–70.. |
| 13. | Daniel AB, Nagaraj K, Kamath R. Prevalence and determinants of tobacco use in a highly literate rural community in southern India. Natl Med J India 2008;21:163-5. |
[Table 1], [Table 2], [Table 3], [Table 4]
|









 Search Pubmed for
Search Pubmed for