|
 
 |
| ORIGINAL ARTICLE |
|
| Year : 2015 | Volume
: 1
| Issue : 2 | Page : 51-55 |
|
Effect of Training with Teaching Methods Designed Based on Health Belief Model on Knowledge and Self-efficacy in Nurses on the Disciplines Standard Precautions in Hospitals
M Khatun Ghanbary1, M Shamsi1, M Khorsandi1, A Farazi2, M Ranjbaran3, B Eshrati3
1 Department of Health Education and Health, Promotion Faculty of Health, Arak University of Medical Sciences, Arak, Iran
2 Department of Infectious Diseases, Faculty of Medicine, Arak University of Medical Sciences, Arak, Iran
3 Department of Epidemiology, Faculty of Health, Arak University of Medical Sciences, Arak, Iran
| Date of Web Publication | 22-Sep-2015 |
Correspondence Address:
Asst Prof. M Shamsi
Department of Health Education, Faculty of Health, Arak University of Medical Sciences, Arak, Markazi
Iran
 Source of Support: None, Conflict of Interest: None  | Check |

Background: Since education is one of the main elements of prevention and control of nosocomial infections, this study aimed to effect of training with teaching methods designed based on health belief model (HBM) on knowledge and self-efficacy in nurses on the disciplines and standard precautions were taken. Methods: This is a quasi-experimental study that was carried out on 100 nurses 50 in experimental and 50 nurses in control group of nurses working hospitals. Data collection tool performed a valid and reliable questionnaire on HBM on preventive behaviours of nosocomial infections. Statistical analysis was performed using t-test, paired t-test and Chi-square. Results: Mean age in the groups of intervention and control was 35.20 ± 7/41 years and 35.02 ± 7/38 , respectively. Before the intervention, mean scores of the knowledge and self-efficacy of nosocomial infection in the two groups do not have a significant statistical difference. However, after the theory-based training intervention, the mean scores for these variables have significant statistical differences between the two groups (P< 0.05). Conclusion: According to these study results, executives of the plan support the efficacy of the model on promoting knowledge and self-efficacy on the disciplines and standard precautions in nurses. Therefore, use of this model is recommended in health centres and hospitals. Keywords: Health belief model, knowledge, nosocomial infections, nurses, standard precautions
How to cite this article:
Ghanbary M K, Shamsi M, Khorsandi M, Farazi A, Ranjbaran M, Eshrati B. Effect of Training with Teaching Methods Designed Based on Health Belief Model on Knowledge and Self-efficacy in Nurses on the Disciplines Standard Precautions in Hospitals. J Hum Health 2015;1:51-5 |
How to cite this URL:
Ghanbary M K, Shamsi M, Khorsandi M, Farazi A, Ranjbaran M, Eshrati B. Effect of Training with Teaching Methods Designed Based on Health Belief Model on Knowledge and Self-efficacy in Nurses on the Disciplines Standard Precautions in Hospitals. J Hum Health [serial online] 2015 [cited 2018 Aug 21];1:51-5. Available from: http://www.jhhjournal.org/text.asp?2015/1/2/51/165913 |
| Introduction | |  |
Hospital infections is one of the risks associated with health care have a large impact on the incidence and duration of hospitalization and increased costs of topics important to public health in the world. This problem is a common cause of illness and death among hospitalized patients and staff.[1],[2] The risk of infection in developing countries is more than in developed countries and rate of patient's infection exceed of 25% in this countries.[3],[4] In developing countries (fore ex Iran), poor awareness one of the basic issues filed to inappropriate management and poor hospital infections in those countries.[5] Standard precautions opposed to reduce occupational infection in health care facilities and a scale designed both known sources of infection the base is in the control of nosocomial infections.[6],[7]
The core standard precautions are: (a) Washing hands after contact with the patient, (b) the use of barrier precautions (e.g., gloves, gowns and face protection) to avoid skin contact of mucous, and (c) at least manipulation of sharp instruments and the disposal of these items is puncture-resistant containers.[6],[8]
The main purpose of standard precautions to reduce the risk of acquisition by patients, hospital staff, other patients and hospital personnel prevent infection accompanying patients during health care.[9]
The health belief model (HBM): Psychological model that focuses on people's attitudes, opinions and try to explain and predict health behaviours.[10] But this behaviour does not lead to behavioural factors. But the possibility of treating sanitation by other factors such as: demographic characteristics, including age, sex, education, health and behaviour as well as information.[11],[12]
The construct of HBM include:
- Perceived susceptibility to understand and believe that they are exposed to the risk
- Perceived severity, understanding and belief that the problem is serious public health problem, and this can lead to serious problems. Collective of these two structures under the perceived threat posed
- Perceived barriers: Barriers to physical, psychological or financial, and so that the person, in order to adopt healthy behaviour occurs
- Perceived benefits belief that a person's behaviour or comply with recommendations in the prevention or reduction of benefits or impact severity and its complications
- Cues to action include health messages, mass communication and acceptance, such as religious and political leaders and the media to trust that the behaviour in the target group is effective
- Perceived self-efficacy include the same amount of confidence a person (or perceived ability).
The finally take action; the health behaviour is affected constructs above.[10],[13]
In educational planning, selection of theoretical model, recognition of the problem and the effectiveness is most important.[14] Studies of the HBM to increase awareness and acceptance of attitudes and practice in the field of nosocomial infections to prevent nosocomial infections in certain aspects of standard precautions have limited the applicability and impact in the planning of education interventions prevention health promotion of health care has been a lot of uses.[12],[14],[15],[16],[17],[18]
The "HBM" one of the models involved in preventive behaviours is also approximately 20–33% of infections in hospital are preventable [19] Educational program for staff is one of the elements in the prevention and control of nosocomial infections and hospital staffer to the procedure policies in various hospital on the principles of the train [20] educational programs can have a positive impact in reducing morbidity and mortality associated with HAIs have.[17] Meanwhile, nurses play an important role in the control and prevention of nosocomial infections (the highest share of treatment patient's care)[7] should be considered major health behaviour theories of the greatest influences on health behaviour included an unprecedented social impact efficacy intention to change the attitude items have been counted.[21]
Since the awareness and self-efficacy are two main prerequisite for changing health behaviours. Therefore, the aim of this study is to determine the effect of teaching and training methods designed based on the HBM on knowledge and self-efficacy on nurses in the context of standard precautions admitted that the results can be a resource for other researchers.
| Materials and Methods | | |
This quasi-experimental study was carried out on 100 nurses (50 in experimental and 50 nurses in control group). Nurses in hospitals affiliated with the Arak University of Medical Sciences in 2014.
Participants in the study were selected by simple random sampling were enrolled after informed consent.
Inclusion criteria was the Bachelor of Nursing, midwifery and higher and at least a diploma nursing. Exclusion criteria were willing to participate in this research was autonomous. This research is part of the hospital environment including emergency nursing services, dialyze in two hospitals selected.
Data were collected by questionnaire, including Part I: Demographic questions, Part II: The second part of the questions (14 questions) Parts III: Questions of self-efficacy (10 questions) based on the principles of prevention of nosocomial infections based on standard precautions can be measured. Scoring questionnaire to this was done: To know the right answer, thefirst part of the question and the answer was zero wrong. Inquiries self-efficacy was based on Likert scale. The range varies between 1 and 5 points each question and answer so that completely agree = 5, agree = 4, no idea = 3, disagree = 2, and strongly disagree = 1 given score.
The total scores ranged between 1 and 20 that scores of people in every part of the 100 score was calculated. In this study, validity was assessed. That questionnaire on-line guide books reputable sources [22],[23] polls advice faculty members experienced teachers. Reliability in a sample of 30 questionnaires and Cronbach's alpha (the value of the knowledge questions 0.75, and self-efficacy was 0.71) was observed.
Normality of the data in each group was measured using the KS test. In the analysis of data in section of knowledge and self efficacy score as low (<50 score), medium (50-75 score) and good (>75 score) were considered.
Educational content and information on the purpose of the pre-test study also was designed based on the HBM. The training is based on the principles of standard precautions based on hand hygiene education as the most important item was the prevention of nosocomial infections.[14]
Before of the intervention, the data from both groups was collected by questionnaire and educational interventions for groups over a month through seminars interactive tutorial written in 4 sessions of 4 h, with qualified teachers pamphlet, poster providing training and a month later was to remind the multimedia preparation as well as studies and data collection after the intervention, after completion of the test, the control group was given 1-month after giving intervention.
Licensed research ethics committee of the Arak University of Medical Sciences with the number 3-138-91 carry out all rules and regulations of the Ethics Committee.
Data collection in 3 months (12 weeks) after the intervention, and analysis with software SPSS (Version 20) for statistical analysis using descriptive statistics such as frequency, mean and standard deviation inferential statistical tests including independent t-test, pair test, Chi-square and taking into account the significant level of <0.05.
| Result | | |
The mean age of the subjects in the case and control group was (35.2 ± 7.41) and (35.02 ± 7.38) years respectively. The mean of service between two groups was 11.06 ± 7.02 and 11.12 ± 6.47 years respectively. Moreover, 41 (0/82%) participants in the case group men and 9 women (0/18%) women in the control group (P = 0.39). The effect of an educational intervention to increase self-efficacy and awareness groups, before and after based on demographic characteristics as visible in [Table 1].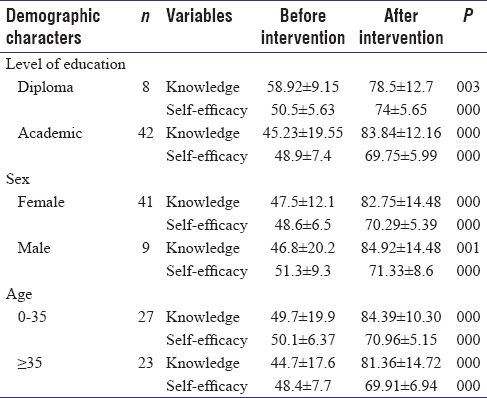 | Table 1: Comparison of effect an educational program on self-effi cacy and knowledge before and after intervention
in case group
Click here to view |
The study aims to determine thefirst hypothesis in the effect of educational based on HBM on knowledge and perceived of self-efficacy in the prevention of nosocomial infection basis of the principles of standard precautions.
The results showed that before the intervention, mean scores of variables (knowledge and perceived self-efficacy) in the prevention of nosocomial infection in the two groups was not statistically significant difference. But three months (12 weeks) after the intervention theory-based training between the average scores of variables in the prevention of nosocomial infection according to independent t-test and handed in the two groups was statistically significant difference.
Also, the paired t-test results showed that in experimental group, a significant difference between perceived self-efficacy in the prevention of nosocomial infections knowledge before and after training there (P < 0/001). While, in the control group in the pre-test and post-test, the differences were not statistically significant [Table 2].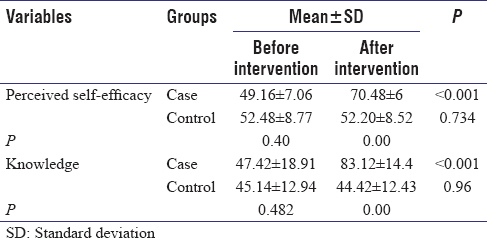 | Table 2: Average knowledge and self-effi cacy of nursing before and 3 months intervention between case and
control groups
Click here to view |
Survey results are used in the training of media is designed based on the HBM in case group in the field of knowledge and self-efficacy showed in [Table 3].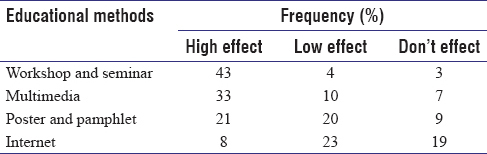 | Table 3: Distribution of the survey of case group about teaching methods
Click here to view |
| Discussion | | |
The findings of this study in order to achieve thefirst objective represent a significant change theory-based training method in trained nurses regarding standard precautions.
Since knowledge is a prerequisite for behaviour change are expected findings in the effect of education on HBM.
As Moujpi et al. in a study as a result of education based on HBM and the health of nursing students stated that knowledge of hand hygiene after the educational intervention based on HBM was significantly increased in comparison with previous findings.[15]
Luo et al. in a study on 1444 nurses and the role of awareness and increase it to the adoption of solar precautions very important respectively.[7] In the study of Wang et al. training on a global alert, the nurses' knowledge increased even after 4 months of this the amount was significant.[24]
In studies conducted in India by Sabane on 108 nursing students, knowledge after training significantly increased.[25] In an another study on the effect of education on knowledge, performance and attitude of health care workers on hospital infections stated that education has a positive effect on knowledge, attitude and practice involved in health care, and need to develop a system of continuing education for all health care workers there.[26]
Low awareness and knowledge of nurses in both the intervention and control groups of health care workers in Janjue studies based on HBM designed consistent in terms of the development and use of global warning level increases.[18] The results showed that educational methods designed to increase self-efficacy in nurses could be based on the HBM. Glodmans recommended that the use of self-efficacy in clinical learning environments can be used as a stimulant on the professional development of nursing students [27] and the efficacy of nursing research, nursing education dummies are also expected about the academic achievement of nursing.[20]
But research on the impact of the weak educational theory based on standard percussion. Perceived self-efficacy as a strong source of motivation and judgment on the ability of people to organize in order to achieve a certain objective.[28]
Research shows that people with high self-efficacy are more committed to the activity at the time of challenges and problems have to spend more effort and time to do their activities. Such people are more likely to maintain healthy behaviour, even after losing the participation of its retrieval plans stronger incentives that not only individuals but also to set a goal to improve the stability in pursuing the objectives.[29],[30]
The results demonstrate the success and efficiency of teaching methods designed (based on HBM) was the nurses' awareness and perceived self-efficacy. Other research has pointed to the effectiveness of the training. Wang et al. to the importance of structured training in enhancing knowledge and behaviour compared with untrained nurses noted.[24]
Training methods like interactive educational workshop sessions alone or in combination with other interventions, can improve professional practice of healthcare workers, but is likely to change the behaviour of complex meetings alone are not effective.[29] Therefore, teaching through lectures or seminars not only improves performance but also help students to use new sources for expanding professional profiles will be.[29],[30]
In the present study given that educational posters to be reminded of educational materials can improve hand hygiene.[30]
Ward also themed study evaluating the use of web-based training in the control of blood-borne infections show that this type of behaviour prevention program increased knowledge has been perceived threats.[28]
According to the study, online resources about infection control nurses was at least, perhaps because they have less access to it because nurses prefer easily accessible training methods. Considering that the study of history, age, education, gender, and employment status differs in both correlation was statistically significant difference was observed in this respect in the group seem to be what the role of the major is the type and quality of education. Demographic characteristics of very slight intervention in the research significant relationship between knowledge and work experience and age was negative.[29]
However, conflicting results of studies on the role of demographic characteristics in terms of their impact on the awareness of the importance of training before and after training.
The limits of this study can be pointed to little of sample size and some of information gathering with self-report.
| Conclusion | | |
The results showed that the impact of teaching practices on knowledge and perceived of self-efficacy of nurses. The execution of this study the efficiency of this model in the design of educational methods based model on promoting knowledge and self-efficacy of nurses in the prevention of nosocomial infections and support the use of this type of practice and other nursing staff recommend.
Acknowledgment
This study is taken from the thesis in master in health education with code number 3-138-91 approval in Arak University of Medical Sciences. Authors of all nurses in this study is appreciated.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
| References | | |
| 1. | Burke JP. Infection control – A problem for patient safety. N Engl J Med 2003;348:651-6.  |
| 2. | Pittet D, Allegranzi B, Storr J, Nejad SB, Dziekan G, Leotsakos A, et al. Infection control as a major World Health Organization priority for developing countries. J Hosp Infect 2008;68:285-92. |
| 3. | Mayon-White RT, Ducel G, Kereselidze T, Tikomirov E. An international survey of the prevalence of hospital-acquired infection. J Hosp Infect 1988;11 Suppl A: 43-8. |
| 4. | Western KA, St John RK, Shearer LA. Hospital infection control – an international perspective. Infect Control 1982;3:453-5. |
| 5. | Allegranzi B, Pittet D. Healthcare-associated infection in developing countries: Simple solutions to meet complex challenges. Infect Control Hosp Epidemiol 2007;28:1323-7. |
| 6. | Siegel JD, Rhinehart E, Jackson M, Chiarello L; Health Care Infection Control Practices Advisory Committee. 2007 Guideline for Isolation Precautions: Preventing transmission of infectious agents in health care settings. Am J Infect Control 2007;35 10 Suppl 2:S65-164. |
| 7. | Luo Y, He GP, Zhou JW, Luo Y. Factors impacting compliance with standard precautions in nursing, China. Int J Infect Dis 2010;14:e1106-14. |
| 8. | World Health Organization. WHO Guidelines on Hand Hygiene in Health Care. First Global Patient Safety Challenge Clean Care is Safer Care, 2009. Geneva, Switzerland: WHO Press; 2011. |
| 9. | Khokhar S. Non-compliance with standard precautions: System theory approach. Int J Nurs Care 2013;1:115-9. |
| 10. | Karen Glanz, Francis Markvz, Barbara Lewis. Shafie Forough. The translation of health behavior and health education. ed.1, Tehran, Ladan 1997. p. 41. |
| 11. | Ghanbari MK, Farazi AA, Shamsi M, Khorsandi M, Esharti B. Measurement of the health belief model (HBM) in nurses hand hygiene among the hospitals. World Applied Sciences Journal 2014;31:811-18. |
| 12. | Efstathiou G, Papastavrou E, Raftopoulos V, Merkouris A. Factors influencing nurses' compliance with standard precautions in order to avoid occupational exposure to microorganisms: A focus group study. BMC Nurs 2011;10:1. |
| 13. | Hazavehei S, Sharifirad G, Mohabi S. The effect of educational program based on health belief model on diabetic foot care. Int J Diabetes Dev Ctries 2007;27:18. |
| 14. | Fuller C, Besser S, Cookson BD, Fragaszy E, Gardiner J, McAteer J, et al. Technical note: Assessment of blinding of hand hygiene observers in randomized controlled trials of hand hygiene interventions. Am J Infect Control 2010;38:332-4. |
| 15. | Mujipi Z. Influence of education of health belief model on hand hygiene condition of nursing students. Chin J Nosocomiol 2011;12:084. |
| 16. | Shamsi M, Tajik R, Mohammadbegee A. Effect of education based on Health Belief Model on self-medication in mothers referring to health centers of Arak. Arak Univ Med Sci J 2009;12:57-66. |
| 17. | Gupta A, Kapil A, Kabra SK, Lodha R, Sood S, Dhawan B, et al. Assessing the impact of an educational intervention on ventilator-associated pneumonia in a pediatric critical care unit. Am J Infect Control 2014;42:111-5. |
| 18. | Shamsi M, Bayati A. A survey of the prevalence of self-medication and the factors affecting it in pregnant mothers referring to health centers in Arak city. J Jahrom Univ Med Sci 2010;7:34-42. |
| 19. | Harbarth S, Sax H, Gastmeier P. The preventable proportion of nosocomial infections: an overview of published reports. J Hosp Infect 2003;54:258-66. |
| 20. | Peterson VM. Predictors of academic success infirst semester baccalaureate nursing students. Soc Behav Pers Int J 2009;37:411-7. |
| 21. | Noar SM, Chabot M, Zimmerman RS. Applying health behavior theory to multiple behavior change: considerations and approaches. Prev Med 2008;46:275-80. |
| 22. | GhanbaryM, Shamsi M, Farazi A, Khorsandy M, Eshrati B. The survey of knowledge, self-efficacy and practice of nurses in standard precautions to prevent nosocomial infections in hospitals of Arak University of Medical Sciences, 2013. Arak Medical University Journal 2013;16:45-54. |
| 23. | World Health Organization. WHO Guidelines on Hand Hygiene in Health Care:First Global Patient Safety Challenge. Clean Care is Safer Care. Geneva, Switzerland. WHO Press: World Health Organization; 2009. |
| 24. | Wang H, Fennie K, He G, Burgess J, Williams AB. A training programme for prevention of occupational exposure to bloodborne pathogens: impact on knowledge, behaviour and incidence of needle stick injuries among student nurses in Changsha, People's Republic of China. J Adv Nurs 2003;41:187-94. |
| 25. | Sabane HH, Dixit RR, Durge P. Impact of knowledge about Post exposure prophylaxis among nursing students-A cross sectional study. Nursing 2011;1:4.68. |
| 26. | Suchitra JB, Lakshmi Devi N. Impact of education on knowledge, attitudes and practices among various categories of health care workers on nosocomial infections. Indian J Med Microbiol 2007;25:181-7. [ PUBMED]  |
| 27. | Gloudemans H, Schalk R, Reynaert W, Braeken J. The development and validation of a five-factor model of Sources of Self-Efficacy in clinical nursing education. J Nurs Educ Pract 2012;3:80. |
| 28. | Pisanti R, Lombardo C, Lucidi F, Lazzari D, Bertini M. Development and validation of a brief Occupational Coping Self-Efficacy Questionnaire for Nurses. J Adv Nurs 2008;62:238-47. |
| 29. | Karami Matin B, Sepahi S, Khoshay A, Sepahi V, Shahabadi S, Laghaei Z, et al. The effect of training based on health belief model on the awareness and attitude of nursing and midwifery students in preventing cardiovascular diseases. Educ Res Med Sci J 2013;1:28-33. |
| 30. | Javaheri Tehrani F, Nikpour S, Haji Kazemi EA, Sanaie N, Shariat Panahi SA. The effect of education based on health belief model on health beliefs of women with urinary tract infection. Int J Community Based Nurs Midwifery 2014;2:2-11. |
[Table 1], [Table 2], [Table 3]
|









 Search Pubmed for
Search Pubmed for