|
 
 |
| ORIGINAL ARTICLE |
|
| Year : 2015 | Volume
: 10
| Issue : 1 | Page : 8-12 |
|
Hand washing practices and techniques among health professionals in a tertiary hospital in Kano
Mohammed Abdulsalam1, Aliyu Ibrahim1, Godpower Michael2, Abubakar Mijinyawa3
1 Department of Paediatrics, Aminu Kano Teaching Hospital/Bayero University, Kano, Nigeria
2 Department of Family Medicine, Aminu Kano Teaching Hospital, Kano, Nigeria
3 Department of Nursing and Continuing Education, Aminu Kano Teaching Hospital, Kano, Nigeria
| Date of Web Publication | 4-Nov-2015 |
Correspondence Address:
Dr. Mohammed Abdulsalam
Department of Paediatrics, Aminu Kano Teaching Hospital/Bayero University, Kano
Nigeria
 Source of Support: None, Conflict of Interest: None  | Check |
DOI: 10.4103/9783-1230.169058

Background: The simple act of hand washing has been proven to reduce the risk of acquiring hospital infection, especially with the current concern of Ebola viral disease. Hospital acquired infections have contributed significantly to overall mortality and morbidity and health care cost. They report that hand washing remains at an unacceptable low level in most medical environments, with large numbers of doctors and nurses routinely forgetting to wash their hands before touching patients. Transmission of health-care-associated infections often occurs via the contaminated hands of health care workers. Materials and Methods: It was a descriptive cross-sectional study carried out among randomly selected doctors and nurses in Aminu Kano Teaching Hospital, Kano. The questionnaires were administered to the respondents during their ward rounds or clinic sessions.
Results: One hundred and forty health professionals comprising 98 nurses and 42 doctors were studied. About 64.4% of them were aware of the World Health Organization (WHO) global hand washing day but only 15% stated the date correctly. About 99.3% of them believed that if hand washing is done correctly it can reduce the risk of infection. All (100%) of the health professionals use water and soap or hand rubs as agents of hand washing. About 93.6% were taught hand washing technique and 47% were aware of the five moments in hand washing but only 17% of them could list the five moments in hand washing. Only 25.7% health professionals knew the correct steps of hand washing (χ2 = 2.444, df = 2, P = 0.295). Ninety-one percent of the health professionals had seen posters on hand washing. Majority (72.1%) adhered to principles of hand washing (χ2 = 0.015, df = 1, P = 0.902) while 82.1% wash their hands before touching patients (χ2 = 2.841, df = 1, P = 0.092). However, most of them (95%) washed their hands after touching patients and 97% washed their hands after handling body fluids or secretions from patients. On the other hand, only 39% health professionals washed hands before wearing hand gloves (χ2 = 0.321, df = 1, P = 0.571) but 95% washed hands after removing the hand gloves. Ninety-nine percent washed their hands after visiting or using the restroom. Conclusion: This study underscores the need for continuous information and education of health professionals on the importance WHO global hand washing day. As doctors and nurses are important in the health care team, it is important to provide the appropriate knowledge and training regarding preventive practices of infectious diseases. Training and retraining of health professionals on correct steps of hand washing will encourage and remind them on the importance of washing hands before wearing gloves and before touching patients to reduce the risk of infection and cross infection. Keywords: Doctors, hand washing, health professionals, hygiene, nurses
How to cite this article:
Abdulsalam M, Ibrahim A, Michael G, Mijinyawa A. Hand washing practices and techniques among health professionals in a tertiary hospital in Kano. J Med Investig Pract 2015;10:8-12 |
How to cite this URL:
Abdulsalam M, Ibrahim A, Michael G, Mijinyawa A. Hand washing practices and techniques among health professionals in a tertiary hospital in Kano. J Med Investig Pract [serial online] 2015 [cited 2018 Aug 17];10:8-12. Available from: http://www.jomip.org/text.asp?2015/10/1/8/169058 |
| Introduction | |  |
Health-care associated infections are important causes of morbidity and mortality among inpatients worldwide.[1] Such infections affect nearly 2 million individuals annually in the United States and are responsible for approximately 80,000 deaths each year.[2] Transmission of health-care-associated infections usually occurs via the contaminated hands of health care workers. Interestingly, hand hygiene, which is handwashing with soap and water or use of a waterless, alcohol-based hand rub has long been considered one of the most important measures for preventing health-care-associated infections.[3] However, compliance by health care workers with recommended hand hygiene procedures has remained unacceptable low, with compliance rates generally below 50%.[2]
Hand hygiene promotion has been challenging for a 150 years.[4] Health care professionals must be aware of the significance of sanitation through hand washing in their working area.[5] Healthcare professionals must take responsibility on their hand hygiene, and it is imperative for hospitals to take necessary actions to control the spread of diseases within the hospital environments. Various factors are responsible for poor handwashing compliance among health care workers. These include lack of knowledge among health personnel about the importance of hand hygiene in reducing the spread of infection and how hands become contaminated, lack of knowledge of correct hand hygiene technique, understaffing and overcrowding, lack of handwashing facilities, irritant contact dermatitis associated with frequent exposure to soap and water, and lack of institutional commitment to good hand hygiene.[6]
Hand hygiene adherence and promotion involve factors at both the individual and institutional level. Enhancing individual and institutional attitude regarding the feasibility of making changes (self-efficacy), obtaining active participation of personnel at both levels, and promoting an institutional safety climate represent challenges that exceed the current perception of the role of infection control professionals.[4] To address this problem of lack of compliance with hand hygiene, continuous efforts are being made to identify effective and sustainable strategies. One of such efforts is the introduction of an evidence based concept of "My five moments for hand hygiene" by World Health Organization (WHO). These five moments that call for the use of hand hygiene include the moment before touching a patient, before performing aseptic and clean procedures, after being at risk of exposure to body fluids, after touching a patient, and after touching patient surroundings.[7] Lack of hand washing remains at an unacceptable low level in most medical environments, with large numbers of doctors and nurses routinely forgetting to wash their hands before touching patients.[8],[9] In view of the worldwide needs to improve hand hygiene in health care facilities, the WHO launched its guidelines on hand hygiene in health care (advanced draft) in October 2005. These consensus guidelines reinforce the need for multi-dimensional measures as the most effective approach to promote hand hygiene.[10] Important components of these guidelines include staff education and motivation, adoption of an alcohol-based hand rub as the primary method for hand hygiene, use of performance feedback indicators, and strong commitment by all stakeholders, such as front-line staff, managers and health care leaders, to improve hand hygiene.
The Centers for Disease Control and Prevention (CDC) recommends hand washing over hand sanitizer rubs, particularly when hands are visibly dirty.[4],[11] Wearing gloves during patient care is an additional measure that helps reduce transmission of pathogens in high-risk situations.[12],[13],[14] Also, when gloves are worn in accordance with CDC's standard precaution, gloves protect health care workers from exposure to blood-borne infections such as HIV and hepatitis B and C.[12],[15],[16] Health care workers should demonstrate accurate knowledge of hand hygiene.[17],[18],[19]
The current study was carried out to determine the hand washing practices and techniques among health professionals of Aminu Kano Teaching Hospital (AKTH), Kano.
| Materials and Methods | | |
This was a descriptive cross-sectional study carried out among doctors and nurses of AKTH. The study was conducted between August 2014 and February 2015. The study was carried out after obtaining permission from the Ethics Committee of AKTH, Kano, and getting consent from the doctors and the nurses. The questionnaires were administered to the respondents during their daily ward rounds and clinic sessions. The contents of the questionnaires included age, sex, profession, years of working experience, awareness of global hand washing day, whether or not taught on hand washing technique, agents used in hand washing, five moments in hand washing and ability to list them, having seen poster on hand washing technique, steps in hand washing, adherence to principle of hand washing, washing hands before and after touching patients or after handling secretions or body fluids of patients, washing hands before wearing and after removing hand gloves and after using toilets.
Data analysis
The information obtained from the subjects was entered and subsequently analyzed using Statistical Package for Social Sciences version 16 by Microsoft Corporation 2007. Quantitative variables were summarized using means and medians while qualitative variables were summarized using frequencies and percentages and categorical variables were compared using Chi-square test of significance while P < 0.05 was considered as being statistically significant.
| Results | | |
A total of 140 health professionals were recruited for the study. They comprised of 98 (70%) nurses and 42 (30%) doctors. There were 71 (50.7%) females and 69 (49.3%) males with male to female ratio of 1:1.03. Their ages ranged from 20 to 60 years with a mean age of 36.95 ± 6.59 years. Ninety (64.3%) health professionals are aware of the WHO global hand washing day and only 21 (15%) were able to correctly state the exact date while 50 (37.7%) health professionals were not aware of the WHO global hand washing day, and none of them could state the exact date. χ2 = 21.21, df = 2, P = 0.000. This is statistically significant. However, 139 (99.3%) health professionals believed that hand washing if correctly done can reduce the risk of infections but 25 (17.9%) of them did not wash their hands before touching patients. One hundred and thirty one (93.6%) health professionals were taught hand washing and 66 (47.1%) were aware of the five moments in hand washing while 65 (46.4%) were not aware of the five moments. Nine (6.4%) were not taught hand washing but 4 (2.9%) are aware of the five moments of hand washing. Chi-square = 0.119, df = 1, P = 0.73. This is not statistically significant.
[Table 1] shows that 131 (93.6%) health professionals were taught hand washing and of these 92 (65.7%) were nurses while 39 (27.9%) were doctors. This is not statistically significant. (χ2 = 0.051, df = 1, P = 0.822).
[Table 2] below compares profession and ability to list correct steps of hand washing. Only 36 (25.7%) health professionals were able to list the correct steps of hand washing and of these, 12 (8.6%) were doctors while 24 (17.1%) were nurses (χ2 = 2.444, df = 2, P = 0.295).
From [Table 3], only 6 (4.3%) doctors could list the five moments of hand washing correctly, the majority of them did not know the five moments. This was similar to the nurses group where only 18 (12.9%) knew the five moments while the rest 58 (41.4%) did not know. This was however, not statistically significant (χ2 = 1.967, df = 2, P = 0.347).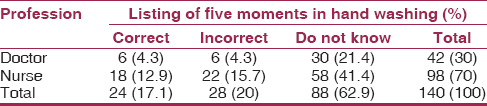 | Table 3: Profession versus ability to list the five moments of hand washing
Click here to view |
From [Table 4] showed some adherence to principles of hand washing by various health professionals. Thirty (21.4%) doctors and 71 (50.7%) nurses adhered to principles of hand washing. The overall adherence rate was 72.1%. This is not statistically significant (χ2 = 0.015, df = 1, P = 0.902).
[Table 5] showed that majority of 115 (82.1%) of the health professionals wash their hands before touching patients and of this number doctors constitute 22.1% while nurses made up to 60%. It is not statistically significant (χ2 = 2.841. df = 1, P = 0.092).
However, 133 (95%) of the health professionals did wash their hands after touching patients while 138 (98.6%) of them washed their hands after handling body fluids or secretions from patients.
[Table 6] showed that most health professionals (60.7%) did not wash their hands before wearing hand gloves. However, this was not statistically significant (χ2 = 0.321, df = 1, P = 0.571).
[Table 7] showed that 133 (95%) of the health professional washed their hands after removing their hand gloves and from these, 40 (28.6%) were doctors while 93 (66.4%) were nurses. However, there was not statistically significant (χ2 = 0.007, df = 1, P = 0.933).
It was also observed that almost all 138 (98.6%) health professionals washed their hands after visiting or using restroom and all 140 (100%) health professionals agreed that they use water and soap or hand rubs as agent of hand washing.
| Discussion | | |
From this study, it is clear that the health professionals had moderate knowledge on the WHO global hand washing day. They, however, had a significantly higher knowledge on the benefits of hand washing in reducing infection. This is probably due to the recent Ebola awareness and personal protection seminar that was organized for hospital staffs due to the outbreak of Ebola viral disease in some West African countries. They were also well informed on the use of water and soap or hand rubs as agents of hand washing. There was also a high rate of adherence to principles of hand washing among all the categories of health professionals studied. This contrasted with the findings in Sri Lankan study where compliance of healthcare workers to hand hygiene guideline was reported to be poor;[11] similar observation was noted in other countries [20] Allegranzi et al. also recorded a low compliance rate of 51% in their study.[21] This low compliance rate was attributed to nonimplementation of the WHO strategies on hand hygiene.[21] Despite evidence of benefit, adherence to hand hygiene among health care professionals remains low. Several behavioral and organizational theories have been proposed to explain this.[22] As a whole, the success of interventions to improve adherence to hand hygiene among health care professionals has been limited. Recent data suggest that a multifaceted intervention, including the use of feedback, education, the introduction of alcohol-based hand wash, and visual reminders, may increase adherence to hand hygiene recommendations.[21] However, very few health professionals knew and listed the five moments on hand washing in this study. This may be due institutional failures in commemorating this day as recognized by WHO, therefore, health workers may have limited knowledge of WHO global hand washing day.[10] They also had very poor knowledge of the correct steps of hand washing, and this may be due to infrequent training and retraining of health workers on hand washing technique; which make them easily forgettable.[20] Furthermore lack of staff evaluation and motivation on hand washing practices may result in poor performance.[23] A higher rate of hand washing among the health professionals was found in; after touching patients, after handling body fluids or secretions from patients, after removing hand gloves and after using the restroom. This finding could be attributed to their knowledge of disease transmission and a personal need for self-protection, in a similar survey of hand washing in Ghana, the strongest motivators for hand washing were related to nurturance, social acceptance, and disgust of feces.[24] Protection from disease was mentioned as a driving force but was not a key motivator of hand washing.[25] This further buttresses the point that knowledge of disease transmission is an important motivating factor for hand washing amongst health personnel. The health belief model has some key components of perceived susceptibility, perceived severity, perceived benefits, and perceived barriers.[23] The attitude of hand washing before wearing gloves and before touching patients is also not poor in both groups of health professionals. Studies have shown that self-reported adherence to hand hygiene is higher than the actual adherence during the working shift. However, having regular hand hygiene campaigns, displaying posters and encouraging peers to remind colleagues of hand hygiene have been shown to improve the compliance of health professional significantly.[26]
It is important to improve the current training programs targeting hand hygiene practices among health professionals. Hand washing training sessions may need to be conducted more frequently for health professionals with continuous monitoring and evaluation to encourage them to follow correct hand washing practices.[27],[28] Doctors and nurses are important in the health care team; it is important to provide the best knowledge and training regarding preventive measures of infectious diseases.[23] It has been shown that doctors' adherence to proper hand hygiene practices can be improved by personal encounters, direct meetings with the infectious disease physician and video presentations and adherence to WHO strategies on hand hygiene.[21] It is important that the infection prevention unit of the hospitals get more involved with health care providers training and the updating of infection prevention notices.[29] It is recommended that hospitals should develop and implement innovative educational and motivational programs adapted to specific groups of health personnel to improve hand hygiene practice and compliance.[30]
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflict of interest.
| References | | |
| 1. | Jarvis WR. Selected aspects of the socioeconomic impact of nosocomial infections: Morbidity, mortality, cost, and prevention. Infect Control Hosp Epidemiol 1996;17:552-7.  |
| 2. | Pittet D, Mourouga P, Perneger TV. Compliance with handwashing in a teaching hospital. Infection Control Program. Ann Intern Med 1999;130:126-30. |
| 3. | Lankford MG, Zembower TR, Trick WE, Hacek DM, Noskin GA, Peterson LR. Influence of role models and hospital design on hand hygiene of healthcare workers. Emerg Infect Dis 2003;9:217-23. |
| 4. | CDC. Antimicrobial spectrum and characteristics of hand-hygiene antiseptic agents. MMWR Morb Mortal Wkly Rep 2002;51:45. |
| 5. | |
| 6. | Pittet D, Boyce JM. Hand hygiene and patient care: Pursuing the Semmelweis legacy. Lancet Infect Dis 2001;1:9-20. |
| 7. | Sax H, Allegranzi B, Uçkay I, Larson E, Boyce J, Pittet D. 'My five moments for hand hygiene': A user-centred design approach to understand, train, monitor and report hand hygiene. J Hosp Infect 2007;67:9-21. |
| 8. | Goldmann D. System failure versus personal accountability – The case for clean hands. N Engl J Med 2006;355:121-3. |
| 9. | Pittet D. Improving compliance with hand hygiene in hospitals. Infect Control Hosp Epidemiol 2000;21:381-6. |
| 10. | |
| 11. | Ariyaratne MJ, Gunasekara TD, Weerasekara MM, Kottahachchi J, Kudavidanage BP, Fernando SS. Knowledge, attitudes and practices of hand hygiene among final year medical and nursing students at the University of Srilanka Jayewardenepura. Sri Lankan J Infect Dis 2013;3:15-25. |
| 12. | Pittet D, Dharan S, Touveneau S, Sauvan V, Perneger TV. Bacterial contamination of the hands of hospital staff during routine patient care. Arch Intern Med 1999;159:821-6. |
| 13. | Pessoa-Silva CL, Dharan S, Hugonnet S, Touveneau S, Posfay-Barbe K, Pfister R, et al. Dynamics of bacterial hand contamination during routine neonatal care. Infect Control Hosp Epidemiol 2004;25:192-7. |
| 14. | Tenorio AR, Badri SM, Sahgal NB, Hota B, Matushek M, Hayden MK, et al. Effectiveness of gloves in the prevention of hand carriage of vancomycin-resistant enterococcus species by health care workers after patient care. Clin Infect Dis 2001;32:826-9. |
| 15. | Johnson S, Gerding DN, Olson MM, Weiler MD, Hughes RA, Clabots CR, et al. Prospective, controlled study of vinyl glove use to interrupt Clostridium difficile nosocomial transmission. Am J Med 1990;88:137-40. |
| 16. | Garner JS. Guideline for isolation precautions in hospitals. The Hospital Infection Control Practices Advisory Committee. Infect Control Hosp Epidemiol 1996;17:53-80. |
| 17. | Duckro AN, Blom DW, Lyle EA, Weinstein RA, Hayden MK. Transfer of vancomycin-resistant enterococci via health care worker hands. Arch Intern Med 2005;165:302-7. |
| 18. | Larson EL, Eke PI, Wilder MP, Laughon BE. Quantity of soap as a variable in handwashing. Infect Control 1987;8:371-5. |
| 19. | Widmer AE, Dangel M. Alcohol-based handrub: Evaluation of technique and microbiological efficacy with international infection control professionals. Infect Control Hosp Epidemiol 2004;25:207-9. |
| 20. | How-to Guide. Improving Hand Hygiene: A Guide for Improving Practices among Health Care Workers. Institute for Health Care Improvement. Available from: http://www.IHI.org. [Last accessed on 2015 Apr 04]. |
| 21. | Allegranzi B, Gayet-Ageron A, Damani N, Bengaly L, McLaws ML, Moro ML, et al. Global implementation of WHO's multimodal strategy for improvement of hand hygiene: A quasi-experimental study. Lancet Infect Dis 2013;13:843-51. |
| 22. | Maskerine C, Loeb M. Improving adherence to hand hygiene among health care workers. J Contin Educ Health Prof 2006;26:244-51. |
| 23. | Min JS. Hand hygiene compliance: A multidisciplinary and protective Approach. J Contin Educ Health Prof 2006;26:244-51. |
| 24. | Scott B, Curtis V, Rabie T, Garbrah-Aidoo N. Health in our hands, but not in our heads: Understanding hygiene motivation in Ghana. Health Policy Plan 2007;22:225-33. |
| 25. | Pronovost P, Needham D, Berenholtz S, Sinopoli D, Chu H, Cosgrove S, et al. An intervention to decrease catheter-related bloodstream infections in the ICU. N Engl J Med 2006;355:2725-32. |
| 26. | Beggs CB, Shepherd SJ, Kerr KG. Increasing the frequency of hand washing by healthcare workers does not lead to commensurate reductions in staphylococcal infection in a hospital ward. BMC Infect Dis 2008;8:114. |
| 27. | Fischler GE, Fuls JL, Dail EW, Duran MH, Rodgers ND, Waggoner AL. Effect of hand wash agents on controlling the transmission of pathogenic bacteria from hands to food. J Food Prot 2007;70:2873-7. |
| 28. | Edmonds SL, Mann J, McCormack RR, Macinga DR, Fricker CM, Arbogast JW, et al. SaniTwice: A novel approach to hand hygiene for reducing bacterial contamination on hands when soap and water are unavailable. J Food Prot 2010;73:2296-300. |
| 29. | Opara PI, Alex-Hart BA. Hand washing practices amongst medical students. Niger Health J 2009;9:1-4. |
| 30. | Bukhari SZ, Hussain WM, Banjar A, Almaimani WH, Karima TM, Fatani MI. Hand hygiene compliance rate among healthcare professionals. Saudi Med J 2011;32:515-9. |
[Table 1], [Table 2], [Table 3], [Table 4], [Table 5], [Table 6], [Table 7]
|









 Search Pubmed for
Search Pubmed for