|
 
 |
| CASE REPORT |
|
| Year : 2013 | Volume
: 1
| Issue : 2 | Page : 70-76 |
|
Piezocision-assisted canine distalization
Ozlem Aylikci1, Caglar Sakin2
1 Department of Orthodontics, Research Assistant in Orthodontics, DDS, Erciyes University, College of Dentistry, Kayseri, Turkey
2 Private Practice in Orthodontics, Ankara, Turkey
| Date of Web Publication | 7-Aug-2013 |
Correspondence Address:
Caglar Sakin
Private Practice ?n Orthodontics, Phd, Ankara
Turkey
 Source of Support: None, Conflict of Interest: None  | Check |
DOI: 10.4103/2321-3825.116288

An increasing number of adult patients are seeking orthodontic treatment to improve their smile or their masticatory function. One of the biggest challenges an adult orthodontic patient faces is the time spent wearing brackets because time and esthetics have become increasingly important in this time. Over the years, several surgical techniques have been developed to address this issue and reduce overall treatment time. Although very effective, these techniques have proven to be quite invasive. A new, minimally invasive surgical procedure [piezocision] is presented in this case report that combines microincisions and localized piezoelectric surgery to achieve similar results rapidly and with minimal trauma. Keywords: Microincisions, canine distalization, piezocision
How to cite this article:
Aylikci O, Sakin C. Piezocision-assisted canine distalization. J Orthod Res 2013;1:70-6 |
| Introduction | |  |
An increasing number of adult patients have been seeking orthodontic treatment in recent years because orthodontic treatment efficiency is especially important when treating adults. These patients have specific demands and usually want to achieve their treatment goals as soon as possible to reduce the negative effects of orthodontic appliances in their social and professional lives. According to the American Association of Orthodontists (AAO) the length of comprehensive orthodontic treatment can range from approximately 12 to 36 months, depending on treatment options and individual characteristics. [1] That is why many patients refuse orthodontic treatment.
To shorten the time necessary for orthodontic tooth movement, various attempts have been made. These attempts mainly fall into three categories. The first is local or systemic administration of medicines such as prostaglandins, [2],[3],[4],[5],[6] interleukins, [7] leukotrienes, [8] cyclic adenosine monophosphate, [9] and vitamin D. [10],[11] The second category is mechanical or physical stimulation. Direct electrical current, [12] pulsed electromagnetic field, [13] samarium cobalt magnet, [14] and low-energy laser [15] were studied. These two methods increase movement speed 0.3 to 1 times according to the literature. However, they are not without problems. The effects of medicines are not specific, and side effects in the long term are unknown. [3],[11],[16] Physical stimulation also has unwanted effects. [13],[17]
The last category is oral surgery, including dental distraction, alveolar surgeries to undermine interseptal bone, and alveolar corticotomies, which have been used to correct malocclusions for over 100 years. [18],[19] Although very effective, these techniques have proven to be quite invasive so, in 2009 Dibart et al. [20] have described a new minimally invasive, periodontally accelerated orthodontic tooth movement procedure [Piezocision]. This procedure combines micro incisions and localized piezoelectric surgery to achieve similar results rapidly and with minimal trauma.
| Case Report | | |
Clinical Evaluation
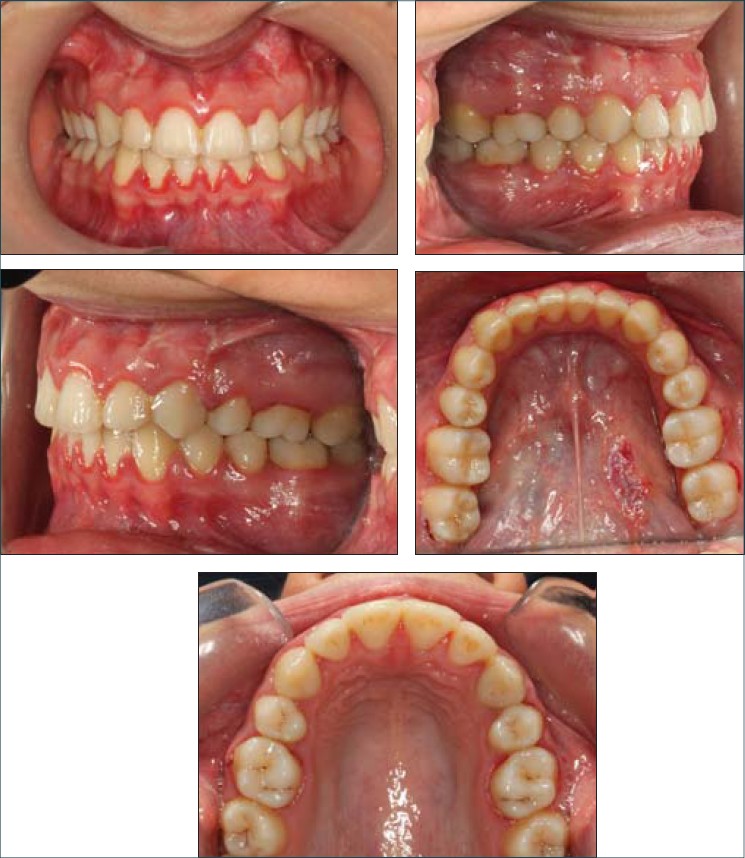
A 19-year-old female patient with a chief complaint of upper anterior crowding and excessive overbite showed a retrusive facial profile. Usual diagnostic examinations: impressions, intraoral and facial photos, panoramic and lateral cephalometric radiographs, and cephalometric tracing and model analysis are performed. The clinical examination revealed skeletal and dental Class II malocclusion, retroclination of upper incisors, deep bite, and deficient anterior facial height. Clinically, she had showed the features of Class II Division 2 malocclusion [Figure 1] and [Figure 2]. The oral hygiene was adequate. Excessive upper incisor and gum display was remarkable during smile, indicating severe gummy smile.
Hayes-Nance analysis revealed upper and lower arch crowding 5 and 2 mm, respectively. There was 0.3 mm Bolton discrepancy in the lower anterior region. A 2 mm lower dental midline deviation to right side was noted. The overbite was 7 mm [Figure 3].
Radiographic Examination
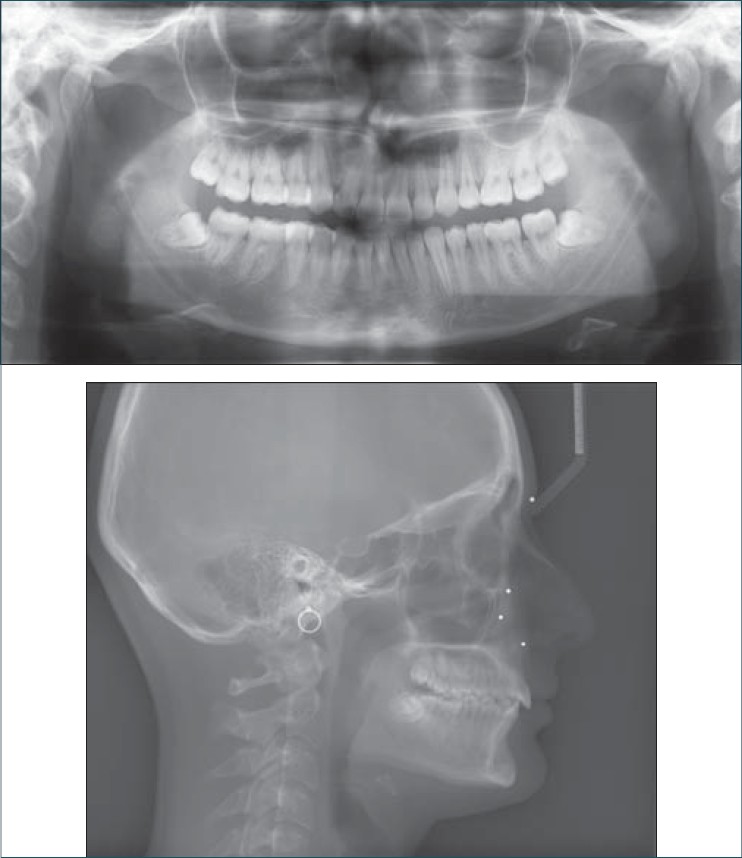
The panoramic film showed impacted third molars. The root form and root length appeared adequate, with good bone support. No fillings, carious lesions, or periodontal defects were observed [Figure 3].
Cephalometric measurements showed an average maxilla with 79.6° SNA angle. 75.8° SNB angle value revealed that mandible was retrognathic. Although mandibular advancement is necessary to improve facial profile, she didn't accept a surgical procedure. Witts value was 3, 8 mm that supports Class II jaw disharmony. Mandible was retrognathic according to McNamara measurements too. All vertical measurements showed low angle vertical pattern. U1-SN and U1-PP were measured 86.5° and 96.2° respectively showing severe retroclination of upper incisors. -1, 1 mm of U1-NA [mm] value also indicates retrusion of upper incisors. Lower incisors are also retroclined according to L1-NB with 12.2° but they are normally inclined according to IMPA with 93.4°. Therefore, interincisal angle was increased to 158.2°. Lastly, soft tissue measurements showed an increased nasolabial angle and retrusive upper and lower lips [Figure 3], [Table 1].
Treatment Objectives
Because she did not approve orthognathic surgery, the treatment objectives was intended for dental correction including elimination of maxillary and mandibular dental crowding and correction of deep bite by intrusion of upper and especially lower incisors. To achieve these goals, extraction of upper first premolars was planned with maximum anchorage mechanics on the left side. A Class II final molar relationship was targeted.
Treatment Progress
After extraction of two upper first premolars, upper and lower arches were bonded. Upper incisors were not bonded at the beginning of treatment for avoiding jiggling effect during retraction of incisors. Leveling was achieved by using 0.016 Ni-Ti and 0.016 x 0.022 Ni-Ti wires, respectively. After leveling phase finished, 0.016 stainless steel wire placed and canine retraction phase was started. Miniscrews were placed bilaterally, to the mesial of first molars, for anchorage control. Before surgery the interdental bone and the proximity of the roots of the teeth were evaluated on the panoramic radiograph. The patient was fully informed of the proposed surgical procedure and signed an informed consent. She accepted this minimally invasive surgical intervention.
Surgical Technique
Surgical procedure was performed with local infiltrative anesthesia to mesial and distal sides of upper canines. After local anesthesia, vertical interproximal incisions were made, 5 mm apical to the mesial and distal interdental papilla of related canines, on the buccal aspect of each jaw using surgical blade No. 15. Incisions were extending 10 mm length apically. The general rule for the incisions was it has to go through the periosteum, which allows the blade to reach the alveolar bone. A Piezo surgical knife [Piezotome, tip BS 1™ UK] was used to create the cortical bone incision through the gingival opening to a depth of approximately 4 mm. When the corticotomies are finished, vertical incisions are closed using a resorbable 5-0 suture. The patient was comfortable and she was discharged under antibiotic and analgesic cover. Whole operation and extractions took only 15 minutes. The patient reported no discomfort and pain. Surgical area was fully healed after 1 week from operation. There was no symptom of edema and inflammation.
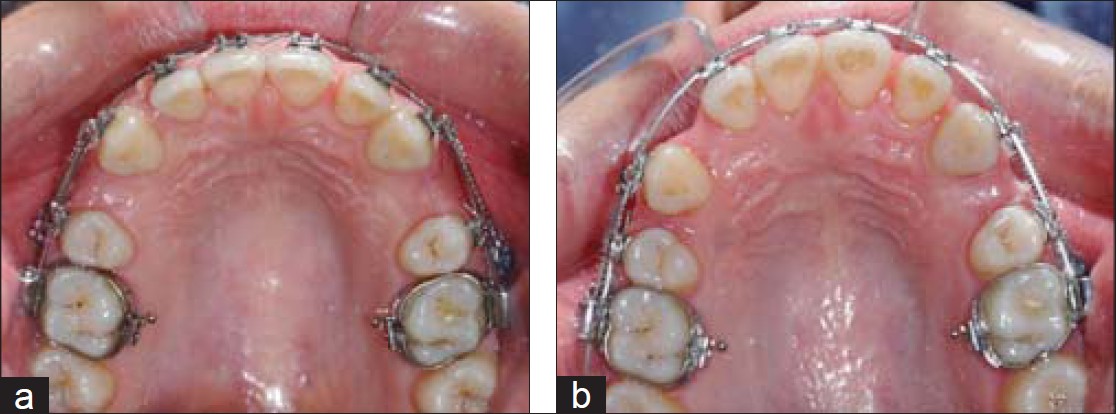
After the operation, canine distalization was performed immediately because the time span between surgical procedure and tooth movement was very critical, using santalloy closed coil springs which conduct 180 gr continuous forces to maxillary canines. Closed coil springs were extending from the hook of canine bracket to ipsilateral miniscrew. Upper right canine was fully distalized after 4 months but left canine distalization took 5 months. After both canines fully distalized, before incisor retraction stage, upper and lower incisor intrusions were achieved using Burstone's intrusion arch. Then 0.016x0.022 inch stainless steel retraction arches with reverse closing loops were inserted.
Treatment Results
At the end of the treatment inclination of upper incisors and gummy smile was improved [Figure 4] and [Figure 5]. The crowding was eliminated, upper and lower incisors were intruded and retraction of upper incisors was achieved. Class II molar and Class I canine relationships were established. Although rapid canine distalization and application of palatinal root torque to upper incisors, there was no remarkable root resorption observed on the panoramic radiograph. Minimal blunting of canine and premolar roots is observed. Marginal alveolar ridges also blunted minimally due to poor oral hygiene [Figure 6].
Upper right canine showed 3.95° and upper left canine showed 8.2° distal tipping. The final positions of canines were normal and there was no need for uprighting [Table 1].
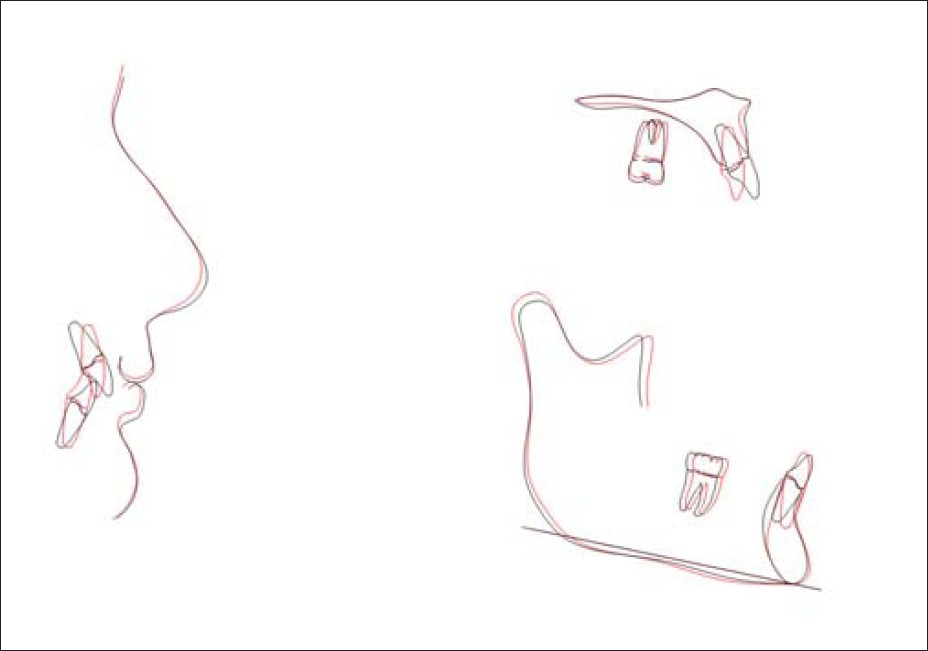
The final lateral cephalometric measurements and the superimpositions of the initial and final lateral cephalometric radiographs revealed that the lower facial height was increased minimally. Overbite correction is achieved mostly by incisor intrusion which is preferred also for retention of deep bite correction. Somewhat overcorrection of incisors was obtained at the end of treatment [Figure 6] and [Figure 7], [Table 1]. A cuspid protected occlusion is achieved after 28 months of active orthodontic treatment.
| Discussion | | |
Length of treatment time is an important factor for adult patients. In recent decades major attempts have been made to shorten the length of treatment. These techniques include rapid distraction of the canines [1] and corticotomy-facilitated orthodontics. [2] In the late 1990s, Wilcko brothers added the alveolar augmentation to the corticotomies and developed the Accelerated Osteogenic Orthodontics (AOO) procedure and claimed that the orthodontic treatment time could be reduced by 75% in the majority of orthodontic cases. [3] By classical methods 1-2 mm canine distalization per month is achieved. In extraction cases canine distalization takes an average of 4-8 months. [21] In the present case, canine distalization phase took 5 months. Fischer reported that the movement rate of canines was significantly higher in the corticotomy group when compared to control. [22] Aboul-Ela et al found that the accumulative moved distance was significantly larger in the corticotomy group for 1, 2, 3, and 4 months. [23] Two of these studies used a corticotomy that was performed by making small perforations on the alveolar bones along the way by which the tooth would be moved, different from piezocision. In this case, piezocision did not provide a dramatic reduction of time during canine distalization. The other accelerated canine distalization studies mostly uses distraction of canines. There is no report that uses piezocision for canine distalization to compare our case.
Possible risks of corticotomy procedures include potential damage to teeth and bone, potential marginal osteonecrosis risk, and impair bone regeneration. [24] Piezoelectric incisions are now recommended because of their safety and effectiveness in different type of surgeries. [25] Piezoelectric knife has micrometric and selective cut so there is no damage on bone tissue and no impact on soft tissue and blood supply. [26] Some authors use and recommend extensive flaps with buccal and palatinal incisions. Such incisions suggested having great clinical results but long surgical time, patient discomfort after surgery, subcutaneous hematomas of the neck and face, and long healing time are disadvantages. [27] The piezocision technique is being proposed because it provides similar clinical outcome as well as decreased surgical time, it is minimally invasive and less traumatic to patient. [28]
Surgically induced high tissue turnover is restricted to the surgical areas and effective only for the first 2 months, [29] but in our case canine distalization is done along a distance of about 7 to 8 mm and took 4 to 5 months. RAP is transient, [30] but the continuous mechanical stimulation of the teeth would prolong the osteopenic effect induced by the procedure; hence, reactivation of appliance every 2 weeks during treatment may be necessary to maintain high tissue turnover which is transient. Dibart et al suggested using higher force application to the teeth to maintain mechanical stimulation of the alveolar bone and the transient osteopenic state would allow rapid treatment. [29] In this case report, continuous and constant force used and reactivated monthly. We achieved 3-4 mm of distalization in first 4 weeks on the right side and 5 weeks on the left side. Faster canine distalization was obtained especially for the first 4-5 weeks on the right side. Amount of tooth movement diminished after fourth week [Figure 8]. Most of distalization is achieved in the first month. The reason may be the transience nature of RAP. A second piezocision might enhance tooth movement after fifth week. In this case, normal orthodontic treatment procedures and optimal force application were used. This procedure reduced overall canine distalization time only about 1 to 2 months. This technique is advised best to use in patients with moderate to severe Class I malocclusions for which the teeth are intended to be moved buccally to resolve crowding or to expand the arch in the needed direction. [29] To our knowledge there are no reports that use piezocision during canine distalization. All cases are nonextraction, minimal to moderate crowding cases. It may be due to insufficient osteopenic effect of piezocision to distalize canine for 7-8 mm. Effect of corticotomy is dose dependent [31] so piezocision cuts may not be enough for canine distalization in this case. Piezocision is a flapless corticotomy technique. Incisions are made through just vertical soft tissue incisions so efficiency of surgical operation may not be fully estimated. That can be the reason of movement differences between two sides.
Possible risks of corticotomy procedures include potential damage to teeth and bone, potential marginal osteonecrosis risk, and impair bone regeneration. [24] Piezoelectric incisions are now recommended because of their safety and effectiveness in different types of surgeries. [25] Piezoelectric knife has micrometric and selective cut so there is no damage on bone tissue and no impact on soft tissue and blood supply. [26] Some authors use and recommend extensive flaps with buccal and palatinal incisions. Such incisions suggested having great clinical results but long surgical time, patient discomfort after surgery, subcutaneous hematomas of the neck and face, and long healing time are disadvantages. [27] The piezocision technique is being proposed because it provides similar clinical outcome as well as decreased surgical time, it is minimally invasive, and less traumatic to patient. [28] In the piezocision technique, palatinal vertical cuts are not being performed.
The amount of root resorption in tooth movement using corticotomy is found to be nonsignificant. [32] In accordance to these results we found no significant root resorption.
Liu and Hung reported 17° distal tipping in rapid canine distraction. Tipping of canine can be effected by various factors. We found distal tipping of canines 3.95° on the right side and 8.2° on the left side and that can be assumed as parallel movement. We carried canine distalization on 0.016 inch stainless steel wires; more parallel movement could be achieved if a 0.016 x 0.022 stainless steel wire was used. Results can be changed if heavier forces used, or force magnitude could be increased progressively. Besides being a minimally invasive technique, piezocision is used successfully in nonextraction cases; its bone turnover enhancement effect was not enough in this extraction case.
| Conclusion | | |
The reduction of treatment time was not cost-effective in canine distalization. Recurrent piezocision can be used during tooth movement to enhance osteopenic effect periodically. Although very useful and noninvasive, piezocision is not a "cure for all" and does not in any case replace alveolar and periodontal distraction of canines. For the use of this minimally invasive surgical technique during canine distalization, further animal and clinical studies are needed.
| References | | |
| 1. | American Association of Orthodontists (AAO). How long does treatment take? Available from: http://www.mylifemysmile.org [Last accessed on 2013 Apr 23]. 
|
| 2. | Chumbley AB, Tuncay OC. The effects of indomethacin on the rate of tooth movement in cats. J Dent Res 1981;60:596.
|
| 3. | Chumbley AB, Tuncay OC. The effects of indomethacin [an aspirin-like drug] on rate of orthodontic tooth movement. Am J Orthod 1986;89:312-4.
[PUBMED] |
| 4. | Yamasaki K, Shibata Y, Fukuhara T. The effect of prostaglandins on experimental tooth movement in monkeys. J Dent Res 1982;61:1444-6.
[PUBMED] |
| 5. | Yamasaki K, Shibata Y, Imai S, Tani Y, Shibasaki Y, Fukuhara T. Clinical application of prostaglandin E1 [PGE1] upon orthodontic tooth movement. Am J Orthod 1984;85:508-18.
[PUBMED] |
| 6. | Lee W. Experimental study of the effect of prostaglandin administration on tooth movement with particular emphasis on the relationship to the method of PGE1 administration. Am J Orthod Dentofacial Orthop 1990;98:231-41.
|
| 7. | Hou Y, Liang T, Luo C. Effects of IL-1 on experimental tooth movement in rabbits. Chin J Stoma 1997;32:46-8.
|
| 8. | Mohammed AH, Tatakis DN, Dziak R. Leukotrienes in orthodontic tooth movement. Am J Orthod Dentofacial Orthop 1989;95:231-7.
[PUBMED] |
| 9. | Yamasaki K. The role of cyclic AMP, calcium, and prostaglandins in the induction of osteoclastic bone resorption associated with experimental tooth movement. J Dent Res 1983;62:877-81.
[PUBMED] |
| 10. | Takano-Yamamoto T, Kawakami M, Yamashiro T. Effect of age on the rate of tooth movement in combination with local use of 1,25[OH]2D3 and mechanical force in the rat. J Dent Res 1992;71:1487-92.
[PUBMED] |
| 11. | Collins MK, Sinclair PM. The local use of vitamin D to increase the rate of orthodontic tooth movement. Am J Orthod Dentofacial Orthop 1988;94:278-84.
[PUBMED] |
| 12. | Davidovitch Z, Finkelson MD, Steigman S, Shanfeld JL, Montgomery PC, Korostoff E. Electric currents, bone remodeling, and orthodontic tooth movement. II. Increase in rate of tooth movement and periodontal cyclic nucleotide levels by combined force and electric current. Am J Orthod 1980;77:33-47.
|
| 13. | Stark TM, Sinclair PM. Effect of pulsed electromagnetic fields on orthodontic tooth movement. Am J Orthod Dentofacial Orthop 1987;91:91-104.
[PUBMED] |
| 14. | Darendeliler MA, Sinclair PM, Kusy RP. The effects of samariumcobalt magnets and pulsed electromagnetic fields on tooth movement. Am J Orthod Dentofacial Orthop 1995;107:578-88.
[PUBMED] |
| 15. | Kawasaki K, Shimizu N. Effects of low-energy laser irradiation on bone remodeling during experimental tooth movement in rats. Laser Surg Med 2000;26:282-91.
|
| 16. | Leiker BJ, Nanda RS, Currier GF, Howes RL, Sinha PK. The effects of exogenous prostaglandins on orthodontic tooth movement in rats. Am J Orthod Dentofacial Orthop 1995;108:380-8.
|
| 17. | Bassett C. Pulsing electromagnetic fields: A new approach to surgical problems. In: Buchwald H, Vargo R, editors. Metabolic surgery. New York: Grune and Stratton; 1978. p. 255-306.
|
| 18. | Liou EJ, Huang CS. Rapid canine retraction through distraction of the periodontal ligament. Am J Orthod Dentofacial Orthop 1998;114:372-82.
[PUBMED] |
| 19. | Ren A, Lv T, Kang N, Zhao B, Chen Y, Bai D. Rapid orthodontic tooth movement aided by alveolar surgery in beagles. Am J Orthod Dentofacial Orthop 2007;131:160.e1-10.
|
| 20. | Dibart S, Sebaoun JD, Surmenian J. Piezocision: A minimally invasive, periodontally accelerated orthodontic tooth movement procedure. Compend Contin Educ Dent 2009;30:342-4.
[PUBMED] |
| 21. | Kumar KV, Umashankar K, Kumar DP. Evaluation of Canine Retraction through Distraction of the Periodontal Ligament: A Clinical Study. J Contemp Dent Pract 2012;13:799-805.
[PUBMED] |
| 22. | Fischer TJ. Orthodontic treatment acceleration with corticotomy-assisted exposure of palatally impacted canines. Angle Orthod 2007;77:417-20.
[PUBMED] |
| 23. | Aboul-Ela SM, El-Beialy AR, El-Sayed KM, Selim EM, El-Mangoury NH, Mostafa YA. Miniscrew implant-supported maxillary canine retraction with and without corticotomy-facilitated orthodontics. Am J Orthod Dentofacial Orthop 2011;139:252-9.
[PUBMED] |
| 24. | Allan W, Williams ED, Kerawala CJ. Effects of repeated drill use on temperature of bone during preparation for osteosynthesis self-tapping screws. Br J Oral Maxillofac Surg 2005;43:314-9.
[PUBMED] |
| 25. | Vercellotti T. Piezoelectric surgery in implantology: A case report-A new piezoelectric ridge expansion technique. Int J Periodontics Restorative Dent 2000;20:358-65.
[PUBMED] |
| 26. | Robiony M, Polini F, Costa F, Vercellotti T, Politi M. Piezoelectric bone cutting in multipiece maxillary osteotomies. J Oral Maxillofac Surg 2004;62:759-61.
[PUBMED] |
| 27. | Vercellotti T, Podesta A. Orthodontic microsurgery: A new surgically guided technique for dental movement. Int J Periodontics Restorative Dent 2007;27:325-31.
[PUBMED] |
| 28. | Dibart S, Sebaoun JD, Surmenian J. Piezocision: A minimally invasive, periodontally accelerated orthodontic tooth movement procedure. Compend Contin Educ Dent 2009;30:342-4.
[PUBMED] |
| 29. | Dibart S, Surmenian J, Sebaoun JD, Montesani L. Rapid treatment of Class II malocclusion with piezocision: Two case reports. Int J Periodontics Restorative Dent 2010;30:487-93. Frost HM. The biology of fracture healing. An overview for clinicians. Part I. Clin Orthop Relat Res 1989;248:283-93.
|
| 30. | Kim HS, Lee YJ, Park YG, Chung KR, Kang YG, Choo HR, et al. Histologic assessment of the biological effects after speedy surgical orthodontics in a beagle animal model: A preliminary study. Korean J Orthod 2011;41:361-70.
|
| 31. | Sukurica Y, Karaman A, Gürel HG, Dolanmaz D. Rapid canine distalization through segmental alveolar distraction osteogenesis. Angle Orthod 2007;77:226-36.
|
| 32. | Liou EJ, Huang CS. Rapid canine retraction through distraction of the periodontal ligament. Am J Orthod Dentofacial Orthop 1998;114:372-82.
[PUBMED] |
[Figure 1], [Figure 2], [Figure 3], [Figure 4], [Figure 5], [Figure 6], [Figure 7], [Figure 8]
[Table 1]
|












 Search Pubmed for
Search Pubmed for