|
 
 |
| ORIGINAL ARTICLE |
|
| Year : 2013 | Volume
: 1
| Issue : 3 | Page : 83-88 |
|
Relative comparison and assessment of patient's attitude and discomfort between two different types of fixed functional appliances: A comprehensive survey
Pooja Gandhi1, Meenu Goel2, Puneet Batra2
1 Dental Surgeon, Woodside Specialty Dental Clinic, 51-23 Queens Blvd, Office Dentist Woodside, NY 11377, USA
2 Department of Orthodontics and Dentofacial Orthopaedics, Institute of Dental Studies and Technologies, Modinagar, Ghaziabad, Uttar Pradesh, India
| Date of Web Publication | 20-Dec-2013 |
Correspondence Address:
Meenu Goel
Department of Orthodontics & Dentofacial Orthopaedics, Institute of Dental Studies and Technologies, Modinagar, Ghaziabad, Uttar Pradesh
India
 Source of Support: None, Conflict of Interest: None  | Check |
DOI: 10.4103/2321-3825.123317

Objective: The aim of this study was to assess the patient's attitude and follow the progress of patient's adaptation to discomfort between two types of fixed functional appliances. Materials and Methods: A total of 16 patients undergoing treatment with either fixed functional appliance, i.e., forsus fatigue resistant device (FFRD) (hybrid) and mandibular protraction appliance (MPA) IV (rigid) rated their experiences during the 1 st day of treatment and after 7 days, 14 days and 30 days of appliance insertion. Results: There were no significant differences in patient's attitude toward both the appliances. Soft-tissue laceration was the most serious side-effect (about 50% in MPA IV and 25% in FFRD). Soft-tissue laceration and other negative effects generally decreased over time. Conclusion: The results of the study indicate that there is no considerable difference in acceptance of FFRD and MPA IV by the patients. Most patients experience some discomfort and functional limitations; however, the effect generally diminishes with time and patients adapt to the appliance. Keywords: Class II malocclusion, fixed functional appliances (forsus fatigue resistant device and mandibular protraction appliance IV), survey
How to cite this article:
Gandhi P, Goel M, Batra P. Relative comparison and assessment of patient's attitude and discomfort between two different types of fixed functional appliances: A comprehensive survey. J Orthod Res 2013;1:83-8 |
How to cite this URL:
Gandhi P, Goel M, Batra P. Relative comparison and assessment of patient's attitude and discomfort between two different types of fixed functional appliances: A comprehensive survey. J Orthod Res [serial online] 2013 [cited 2016 Dec 28];1:83-8. Available from: http://www.jorthodr.org/text.asp?2013/1/3/83/123317 |
| Introduction | |  |
Orthodontic appliances represent foreign objects inserted in a physically and psychologically sensitive area of the body. An important factor in a person's decision to seek orthodontic treatment is the desire to improve dentofacial aesthetics, improvements in social life and self-confidence. [1],[2] Discomfort caused by orthodontic treatment may affect patient's compliance; satisfaction with treatment and it might lead to stress between patient and practitioner. [3],[4],[5] Class II malocclusions have been described as the most frequent treatment problem in orthodontic practice and as one of the more difficult orthodontic problems to treat. [6],[7] Combinations of dental and skeletal factors ranging from mild to severe provide the multiple characters of this discrepancy. [8],[9] Class II malocclusions can be treated by several means, according to the characteristics associated with the problem, such as anteroposterior discrepancy, age and patient compliance. [10] Methods include extraoral appliances, functional appliances and fixed appliances associated with Class II intermaxillary elastics. [6] On the other hand, correction of Class II malocclusions in non-growing patients usually includes orthognathic surgery or selective removal of permanent teeth, with subsequent dental camouflage to mask the skeletal discrepancy.
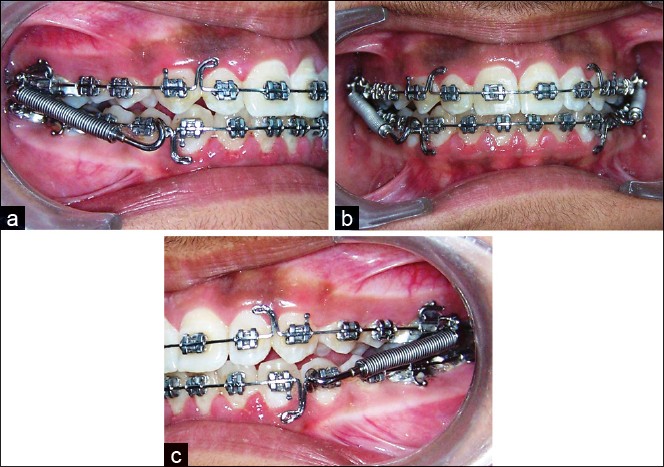
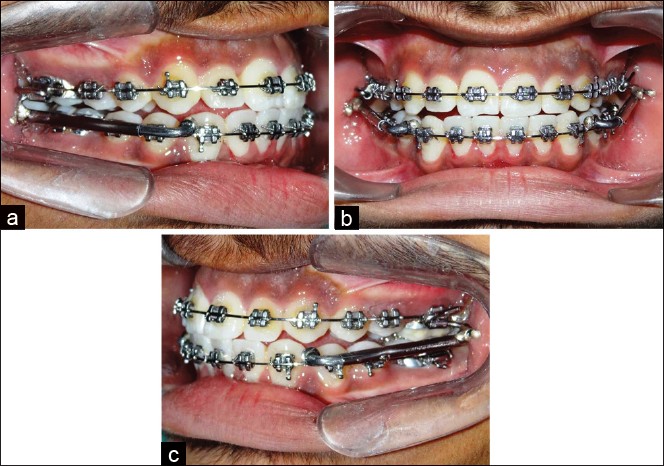
One category of appliances frequently used, typically in growing patients, is the functional orthopedic appliance. [11] They can be grouped into removable or fixed devices. [12],[13] Fixed functional appliances are designed to provide a simple non-compliant solution to orthodontic Class II treatment. Fixed functional appliances first appeared in 1900 when Emil Herbst presented his system at the Berlin International Dental Congress. [14] Ritto and Ferreira classified fixed functional as rigid, flexible and hybrid fixed functional appliances. [15] A number of fixed functional appliances have gained popularity in recent years to help achieve better results in non-compliant patients. Coelho Filho in 1995 presented two versions of a rigid fixed functional appliance that could be made in the office, called the mandibular protraction appliance (MPA) I and II. [16],[17] These appliances were soon replaced by an improved MPA III. [18],[19] The latest version, MPA IV is much easier to construct and install. [20] The forsus fatigue resistant device (FFRD) is a fixed, hybrid functional appliance. [12] As opposed to rigid, fixed functional devices, such as the Herbst appliance; the spring of the FFRD allows flexibility in the position of the mandible. [12] Currently, there is limited data published to access patient experiences with the FFRD with only one published an article by Bowman et al.; whereas there is no quantitative or qualitative data available to evaluate patients experience wearing MPA IV appliance regarding the pain and discomfort of patient. Evaluation of patient experiences during orthodontic treatment will allow clinicians to better select a modality of treatment that will be best accepted by their patients. [21] The purpose of this study was to investigate any potential link between patient's attitudes and the amount of functional and social discomfort experienced with the FFRD and MPA IV. Clinicians using fixed functional appliances may find this information useful in preparing a patient.
| Materials and Methods | | |
A total of 24 patients (15 males, 9 females and mean age 14.5 ± 1.5 years) were recruited for the study from the Department of Orthodontics and Dentofacial Orthopedics, Institute of Dental Studies and Technologies, Modinagar, India. The study comprised of two groups of 12 patients each treated with orthodontic appliances (0.022" MBT prescription): Group I-Class II patients treated with FFRD and Group II-Class II patients treated with MPA IV. Patients undergoing treatment with either fixed functional appliance i.e., FFRD (hybrid) and MPA IV (rigid) shared their experiences during the 1 st days of treatment and after 7 days, 14 days and 30 days of appliance insertion. Subjects having fixed appliance, FFRD and MPA IV in place for at least 2 months and still had the appliance present in their mouth were included in the study [Figure 1] and [Figure 2]. Patients treated with extractions in FFRD and MPA IV groups were excluded. Subjects having unilateral FFRD or MPA IV were excluded regardless of the location of the pushrod. Informed consent was obtained from the subjects' parents and assent was obtained from the subjects.
A questionnaire was used to gather information from orthodontic patients. The questionnaire developed for this study [Appendix] [Additional file 1] was based on two existing surveys. One was the "Smiles Better" survey that was used in the research of O'Brien et al. comparing the Herbst and Twin Block appliances and the other were based on a survey developed by Bowman et al. in investigating the patient experiences with the FFRD. [21],[22] Questionnaire was designed in English and verbally translated in Hindi. The same investigating dentist further explained the question in case of doubts to the patient. The questionnaire consisted of 16 questions. At the end of the data collection period, all responses were collected and subjected to statistical analysis. Descriptive statistics of all questions were calculated. In addition to descriptive statistics, Pearson Chi-square test was used to test for associations, accepting P values of less than 0.05 as statistically significant. Analyses were performed using the Statistical Package for Social Sciences Statistical Package for the Social Sciences (SPSS) Version 16.0, SPSS Inc. Chicago for Windows.
| Results | | |
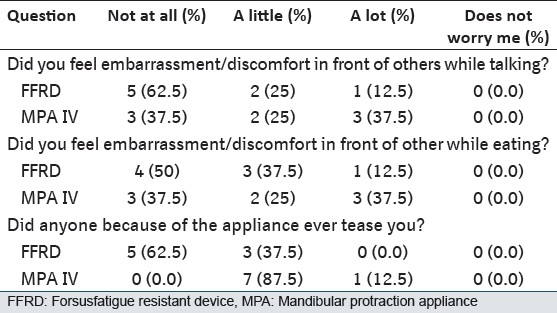
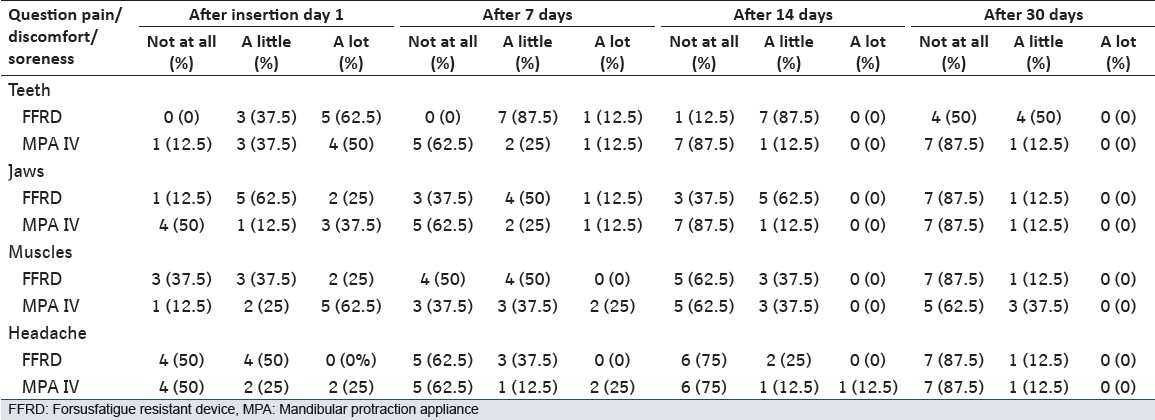
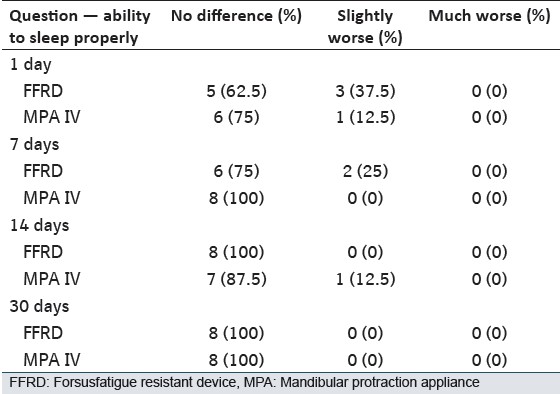
Most patients (93.75%) felt that they were given a complete description and usage instructions of the FFRD and MPA IV before wearing it. Over 68.75% of the subjects agreed that they were happy to look at themselves in the mirror with their appliances on, 31.25% subjects were glad to let their friends see their appliances while 25% were happy when people generally noticed their appliances. Responses regarding the initial effects of FFRD and MPA IV on certain functions (speech and eating) are shown in [Table 1]. They seemed to suffer the greatest initial negative impact, while talking, eating and appearance with MPA IV as compared with FFRD. MPA IV group of patients were annoyed by teasing (P < 0.022) in comparison to FFRD group of patients. When asked about their experience with side-effects when they got the FFRD or MPA IV appliance [Table 2], the majority of respondents reported being affected by (in descending order) sore teeth, jaw, muscle and headache and ability to sleep [Table 3]. Soreness on the lip/cheek from rubbing was significant with both the type of fixed functional appliances and when asked to remove the appliance 75% of subjects using MPA IV wanted to get it removed because of its rigidity and soft-tissue laceration. Subjects were asked to give advice to future FFRD or MPA IV patients. Answers were analyzed and categorized as "yes" or "no." Replies were also categorized by subject matter. Using this classification, 62.5% of the responses were yes in FFRD group and 50% replied yes in MPA IV group.
| Discussion | | |
The likelihood of patient cooperation is one of the most important factors influencing the choice of orthodontic treatment. This present survey showed there is no statistically significant difference between the two (rigid and hybrid) fixed functional appliances in terms of patient's cooperation and pain and discomfort to the patients. The results from an analysis should be of special interest to clinicians as they may assist them to prepare their patients for the inconveniences they may undergo while wearing their appliances. Questions 1 and 2 dealt with the patients' initial experience with the FFRD and MPA IV. The vast majority of patients agreed that they were given a good description of the appliance and that they were provided with instructions for the care of the appliance. Questions 3 through 5 dealt with how noticeable the subject felt the FFRD or MPA IV was responses were varied. The location of mandibular attachment of the FFRD or MPA IV could be one factor. If the appliances were placed more distally, it may have seemed less noticeable to the patient. One survey rated pain as the greatest dislike during treatment and fourth among major fears and apprehensions prior to orthodontic treatment. [23] Pain is a subjective response, which shows large individual variations. It is dependent upon factors such as age, gender, individual pain threshold, the magnitude of the force applied, present emotional state and stress, cultural differences and previous pain experiences. [24] It is notable that although the FFRD and MPA IV group average indicates a downward trend in the experience of pain/discomfort in teeth, jaws, muscles, headache and soreness on the lip or cheek from rubbing, when individual scores were compared, MPA IV group reported the more negative impact, this can be due to the rigidity of the appliance and development of ulcers subsequent to mechanical irritation. Clinicians should be aware of the worsening in lip and cheek irritation that tends to occur in some individuals and they should be ready to manage this side-effect.
In a study of fixed and removable appliances, it was found that discomfort, described as "tightness" and "sensitivity," was the most frequently reported problem by the group in fixed appliances on the 1 st day, with a mean score of 3 on a scale of 1-4. [25] This is in agreement with the present study in that initial discomfort was the most frequently reported negative effect, more so than functional limitations. Bowman et al. also reported initial discomfort with FFRD. In Bowman et al. study, 13.4% reported that a FFRD affected their speech and 65.2% reported it affected their chewing, almost similar results are reported in the present study, in patients with FFRD, 37.5% of patients reported problems with speech, 50% reported problems with eating and 62.5% of patients reported problems with speech and eating respectively in patients with MPA IV appliance. [21] It seems that as compared with patients with FFRD, MPA IV wearers experience a similar amount of discomfort, but have issues with speech and mastication. In the present study, the FFRD and MPA IV group average of functional limitations, side-effects and impact on activities and relationships all decreased over time. This is in accordance with Stewart et al. and Sergl et al. who also found a significant reduction in the number of complaints decreases over time in patients wearing both fixed and removable appliances. [5],[25] This implies that orthodontic patients seem to accept a certain amount of discomfort and functional interferences associated with their orthodontic treatment. Other factors also play an important role in a patient's overall experience with an orthodontic appliance, such as the relationship with the orthodontist, the value patient places on orthodontic treatment or a patient's general outlook on life. Stewart et al. suggest that patient attitude plays a role. [25]
This study provides a comprehensive understanding of the patient's overall experience with the FFRD and MPA IV. The clinic setting, doctor and clinician experience level could all be considered confounding factors in this study. In addition, the results of this study could be strengthened with a larger sample size. Other researchers should repeat this methodology in other locations.
| Conclusion | | |
In general, the results of this study highlight a strong interrelationship between a patient's attitudes at the beginning of the fixed functional appliance phase, his/her capability to accommodate to discomfort associated with the orthodontic appliance. Moreover, there is no significant difference in patient cooperation between the 2 appliances. Most patients experience some discomfort and functional limitations; however, the effect generally diminishes with time and patients adapt to the appliance. Practitioners should be especially vigilant about problems with cheek irritation.
| References | | |
| 1. | Birkeland K, Bøe OE, Wisth PJ. Relationship between occlusion and satisfaction with dental appearance in orthodontically treated and untreated groups. A longitudinal study. Eur J Orthod 2000;22:509-18. 
|
| 2. | Utomi IL. Challenges and motivating factors of treatment among orthodontic patients in Lagos, Nigeria. Afr J Med Med Sci 2007;36:31-6.
[PUBMED] |
| 3. | Sergl HG, Klages U, Zentner A. Pain and discomfort during orthodontic treatment: Causative factors and effects on compliance. Am J Orthod Dentofacial Orthop 1998;114:684-91.
[PUBMED] |
| 4. | Doll GM, Zentner A, Klages U, Sergl HG. Relationship between patient discomfort, appliance acceptance and compliance in orthodontic therapy. J Orofac Orthop 2000;61:398-413.
[PUBMED] |
| 5. | Sergl HG, Klages U, Zentner A. Functional and social discomfort during orthodontic treatment - Effects on compliance and prediction of patients′ adaptation by personality variables. Eur J Orthod 2000;22:307-15.
[PUBMED] |
| 6. | McNamara JA Jr. Components of class II malocclusion in children 8-10 years of age. Angle Orthod 1981;51:177-202.
[PUBMED] |
| 7. | Proffit WR, Fields HW Jr, Moray LJ. Prevalence of malocclusion and orthodontic treatment need in the United States: Estimates from the NHANES III survey. Int J Adult Orthodon Orthognath Surg 1998;13:97-106.
[PUBMED] |
| 8. | Baccetti T, Franchi L, Kim LH. Effect of timing on the outcomes of 1-phase nonextraction therapy of Class II malocclusion. Am J Orthod Dentofacial Orthop 2009;136:501-9.
[PUBMED] |
| 9. | Baccetti T, Franchi L, Stahl F. Comparison of 2 comprehensive Class II treatment protocols including the bonded Herbst and headgear appliances: A double-blind study of consecutively treated patients at puberty. Am J Orthod Dentofacial Orthop 2009;135:698.e1-10.
|
| 10. | Salzmann JA. Practice of Orthodontics. Philadelphia: JB Lippincott Company; 1966. p. 701-24.
|
| 11. | Clark W. Functional treatment objectives. In: Nanda R, Kapila S, editors. Current Therapy in Orthodontics. St. Louis, MO: Mosby Elsevier; 2010. p. 87-102.
|
| 12. | Wahl N. Orthodontics in 3 millennia. Chapter 9: Functional appliances to midcentury. Am J Orthod Dentofacial Orthop 2006;129:829-33.
[PUBMED] |
| 13. | Dandajena T. Hybrid functional appliances for management of Class II malocclusions. In: Nanda R, Kapila S, editors. Current Therapy in Orthodontics. St. Louis, MO: Mosby Elsevier; 2010. p. 103-13.
|
| 14. | Herbst E. Atlas and layout of the dentist lichen orthopedics Munich, Germany: JF Lehmann Verlag; 1910.
|
| 15. | Ritto AK, Ferreira AP. Fixed functional appliances - A classification. Funct Orthod 2000;17:12-30, 32.
[PUBMED] |
| 16. | Coelho Filho CM. Mandibular protraction appliances for Class II treatment. J Clin Orthod 1995;29:319-36.
[PUBMED] |
| 17. | Coelho Filho CM. Clinical applications of the mandibular protraction appliance. J Clin Orthod 1997;31:92-102.
[PUBMED] |
| 18. | Coelho Filho CM. The Mandibular Protraction Appliance No. 3. J Clin Orthod 1998;32:379-84.
[PUBMED] |
| 19. | Coelho Filho CM. Employment clinic device for projection of the mandibule. Dental Press J Orthod 1998;3:69-130.
|
| 20. | Coelho Filho CM. Mandibular protraction appliance IV. J Clin Orthod 2001;35:18-24.
[PUBMED] |
| 21. | Bowman AC, Saltaji H, Flores-Mir C, Preston B, Tabbaa S. Patient experiences with the Forsus fatigue resistant device. Angle Orthod 2013;83:437-46.
[PUBMED] |
| 22. | O′Brien K, Wright J, Conboy F, Sanjie Y, Mandall N, Chadwick S, et al. Effectiveness of treatment for Class II malocclusion with the Herbst or twin-block appliances: A randomized, controlled trial. Am J Orthod Dentofacial Orthop 2003;124:128-37.
|
| 23. | O′Connor PJ. Patients′ perceptions before, during, and after orthodontic treatment. J Clin Orthod 2000;34:591-2.
[PUBMED] |
| 24. | Ngan P, Kess B, Wilson S. Perception of discomfort by patients undergoing orthodontic treatment. Am J Orthod Dentofacial Orthop 1989;96:47-53.
[PUBMED] |
| 25. | Stewart FN, Kerr WJ, Taylor PJ. Appliance wear: The patient′s point of view. Eur J Orthod 1997;19:377-82.
[PUBMED] |
[Figure 1], [Figure 2]
[Table 1], [Table 2], [Table 3]
|










 Search Pubmed for
Search Pubmed for