|
 
 |
| ORIGINAL ARTICLE |
|
| Year : 2014 | Volume
: 2
| Issue : 3 | Page : 135-141 |
|
Evaluation of efficacy of the MBT appliance in expressing inbuilt tip and torque values: Using torque angulation device
MB Raghuraj1, Vivek Amin2, Akhter Husain2, Rohan Mascarenhas2, Sandeep Shetty2
1 Department of Orthodontics and Dentofacial Orthopaedics, Dr. Syamala Reddy Dental College Hospital and Research Centre, Munnekolala, Marathalli (Post), Bengaluru, India
2 Department of Orthodontics and Dentofacial Orthopaedics, Yenepoya Dental College, Mangalore, Karnataka, India
| Date of Web Publication | 12-Sep-2014 |
Correspondence Address:
M B Raghuraj
Department of Orthodontics and Dentofacial Orthopaedics, Dr. Syamala Reddy Dental College Hospital and Research Centre, #111/1 SGR College Main Road, Munnekolala, Marathalli (Post), Bengaluru - 560 037, Karnataka
India
 Source of Support: None, Conflict of Interest: None  | Check |
DOI: 10.4103/2321-3825.140684

Objectives: Several studies on faciolingual inclination have been published and a few statistical investigations have been performed with regard to the preadjusted edgewise appliances, but there is lack of studies which have evaluated the inbuilt characteristics of the MBT preadjusted appliance. This retrospective study was conducted to evaluate the efficacy of the MBT appliance system in terms of expressing its inbuilt characteristics of tip and torque values. Materials and Methods: The study sample consisted of 30 subjects who received full fixed appliance treatment involving four 1 st premolar extractions using the MBT appliance. Pretreatment and posttreatment study models of these subjects were measured for the tip and torque using Torque Angulation Device. Treatment changes were analyzed statistically and the posttreatment measurements were compared with the MBT prescription values. Results: The posttreatment angulation and inclination values when compared with MBT prescription a mean difference of ±2.1° for the tip and ±11.9° for torque. Tip was almost fully expressed in all teeth except for the maxillary 2 nd premolar, 1 st molar, mandibular canine, 2 nd premolar, 1 st and 2 nd molar, where the discrepancy was more than 1°. Torque was under expressed in maxillary central incisor by 1.8°, 1 st molar by 1.5° and 2 nd molar by 11.9°. Torque was over expressed in maxillary lateral incisor by 2.1°, canine by 2.4° and mandibular central and lateral incisor by 4.9° and 4.6°, canine by 4.8°. Torque was sufficiently expressed in maxillary 2 nd premolar, 1 st and 2 nd molar and mandibular 2 nd premolar, with a discrepancy between 0.5°. Conclusion: Tip was almost fully expressed in all teeth except for the maxillary-2 nd premolar, 1 st molar, mandibular- canine, 2 nd premolar, first and 2 nd molar, where the discrepancy was only around 1°. Torque was sufficiently expressed in maxillary-2 nd premolar, 1 st and 2 nd molar and mandibular- 2 nd premolar, where the discrepancy was between 0° and 0.5°. Torque was under expressed in maxillary-central incisor, 1 st molar and 2 nd molar. Torque was over expressed in maxillary- lateral incisor, canine and mandibular-central, lateral incisor and canine. Deviation around the mean measurements was found for all the parameters in all teeth. Keeping in account of individual bracket positioning errors it would be fair to anticipate that MBT appliance would result in reasonably optimal tooth positioning at the end of the treatment without any manual archwire adjustments. Tip was comparatively better expressed when compared to torque. Keywords: Bracket positioning Device, MBT appliance, preadjusted edgewise appliance, tip, torque, Torque Angulation Device
How to cite this article:
Raghuraj M B, Amin V, Husain A, Mascarenhas R, Shetty S. Evaluation of efficacy of the MBT appliance in expressing inbuilt tip and torque values: Using torque angulation device. J Orthod Res 2014;2:135-41 |
How to cite this URL:
Raghuraj M B, Amin V, Husain A, Mascarenhas R, Shetty S. Evaluation of efficacy of the MBT appliance in expressing inbuilt tip and torque values: Using torque angulation device. J Orthod Res [serial online] 2014 [cited 2018 Feb 13];2:135-41. Available from: http://www.jorthodr.org/text.asp?2014/2/3/135/140684 |
| Introduction | |  |
Orthodontic treatment objectives can be stated as obtaining functional occlusion, esthetics and stability. One of the criteria for obtaining a functional occlusion is to have ideal axial inclinations of all teeth at the end of active treatment. The advent of sophisticated appliance and materials has helped to raise the standard of orthodontic treatment, and as a consequence achieving ideal occlusion has become a realistic aim.
Over the years, clinicians have considered how bracket design can help achieve these objectives. [1] Andrews made extensive measurements on untreated excellent occlusions. [2] He determined the average tip and torque angles as well as in-out dimensions of the labial surface of each tooth relative to a flat labial arch wire plane.
The MBT bracket system developed by McLaughlin, Bennett, and Trevisi is a third generation preadjusted edgewise appliance which introduced a range of improvements and specification changes to overcome the clinical shortcomings of earlier preadjusted edgewise bracket systems. [3]
Estimating incisor inclination cephalometrically by reference lines Nasion to A point (NA) and Nasion to B point (NB) makes it difficult for the orthodontist to correlate axial inclination data to the torque prescription of the bracket. Hence, it is important to evaluate the relationship between cephalometrically assessed incisor inclination and torque values. [4] Precise measurements of crown angulation and inclination are crucial for the manufacturing of brackets. Only one study until date has used the Torque Angulation device (TAD), which measured the crown angulation and inclination in precise and objective fashion. [5]
Several studies on faciolingual inclinations have been published and a few statistical investigations have been performed with regard to the preadjusted edgewise appliances, but there is lack of studies which have evaluated the built-in characteristics of the MBT preadjusted appliance.
The main objective of the present retrospective study is to evaluate the efficacy of MBT preadjusted appliance in terms of achieving the optimal expression of its inbuilt characteristics of tip and torque values using TAD.
| Materials and Methods | | |
The sample for the study consisted of 30 subjects who received full fixed appliance treatment in the Department of Orthodontics and Dentofacial Orthopedics, Yenepoya Dental College, Yenepoya University; Mangalore using the MBT preadjusted edgewise appliance system. [6]
The inclusion criteria were as follows:
- Angle's Class I malocclusion with bimaxillary protrusion
- An average mandibular plane angle as defined by McNamara's mandibular plane angle (Gonion-Menton to Frankfurt horizontal plane) of 22° ± 4°
- Cases treated with four 1 st premolar extractions
- Cases treated by MBT appliance prescription.
Method of Measurement
The study model was attached to an adjustable surveying table. The horizontal occlusal line (HOL) of each model was set to be parallel to the Bracket Positioning Device (BPD) granite platform [Figure 1]. The HOL represents an imaginary line connecting the right and left mid-crown molar points and the average of the clinical mid-crown points of the right and left central incisors. The three points on each model were set to be parallel to the BPD platform by adjusting the surveying table unit on BPD by keeping it in reference to the "Bracket Attachment Jaws" of the BPD. The surveying table is locked when it is confirmed that the HOL is achieved and transferred back to the TAD platform [Figure 2]. [5] 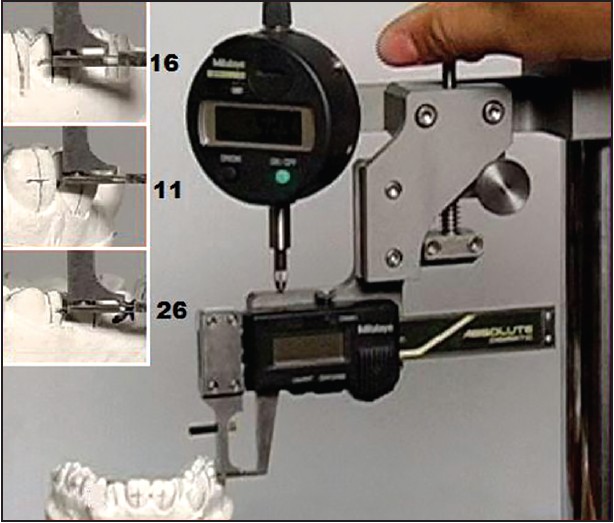 | Figure 1: Setting of horizontal occlusal plane using Bracket Positioning Device
Click here to view |
The crown angulations were measured according to the concept of Andrews. The long axis of the clinical crown (LACC) was drawn on the labial surface of the clinical crowns of every tooth except 3 rd molars [Figure 3]. The midpoint of the clinical crown (LA point) was marked on the long axis of the clinical crown of each tooth. The LA point was constructed by bisecting the height of the clinical crown (add 1.0 mm of the gingival sulcus) on the long axis of the clinical crown. [5] The HOL was used as the occlusal plane The surveying table with a model was transferred to the TAD granite base. The survey base with a model was then offered up to the blade' of the TAD at the same time as adjusting the fine height adjustment screw. The blade was set to lie along the LACC by adjusting the fine angulation adjustment knob, which was located at the center of the mechanism. The crown angulation was read from digital screen on TAD [Figure 3]; the positive or negative value could be adjusted by a micro switch located on the back of the TAD, according to which side of the arch was being worked on.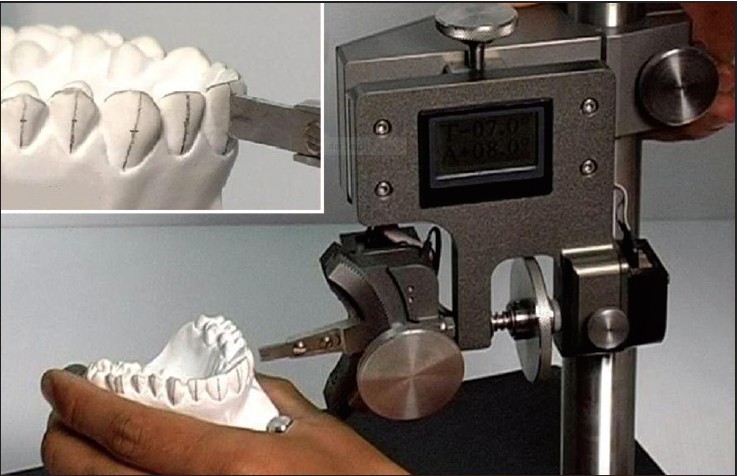 | Figure 3: Adjusting the Torque Angulation Device arm for the best fit on to the long axis of clinical crown line
Click here to view |
The crown inclination was recorded by moving torque fine adjustment knob until the middle of the blade was located well with the LA point and also the curvature of the blade had a "best fit" to the vestibular surface of the tooth being measured. The crown inclination measurement displayed on the digital screen [Figure 3] was then recorded.
Each study model was measured twice by starting at tooth 17 or tooth 37 and working around to tooth 27 or tooth 47 for the first measurement, and then recommencing for the second measurement.
Measurements were recorded for the below mentioned parameters on the pretreatment and the posttreatment study models of 30 study models.
- Tip or crown angulation.
- Torque or crown inclination.
Measurements were recorded for the maxillary and mandibular central incisors, lateral incisors, canines, 2 nd premolars, 1 st molars and 2 nd molars as the sample consisted of cases which had their 1 st premolars extracted as a part of the treatment.
Measurements recorded for the pretreatment models were designated as T1 and those recorded for the posttreatment models were designated as T2.
Radiographic Measurement
Pretreatment and posttreatment lateral cephalograms and orthopantomograms were used for the purpose of measurement. The cephalograms are evaluated for inclination of the upper and lower incisor. The orthopantomograms are evaluated for angulation of the upper and lower incisor. [4]
- Upper incisor inclination was evaluated by connecting long axis of incisor and NA line, the angle formed is taken as reading. Similarly, the long axis of lower incisor and NB line.
- Upper and lower incisor angulations are evaluated by connecting long axis of incisor and midline, the angle formed is taken as reading.
Statistical Analysis
All the statistical analyses were performed using Statistical Product and Service Solutions (SPSS Version 11) software.
Results are expressed as mean ± standard deviation and 95% confidence intervals (CIs) wherever necessary. 95% CIs were calculated as mean ± 2 standard error and represent the population mean.
Treatment changes were analyzed using paired t-test. An unpaired t-test was used to compare with tip, torque, and in-out values from Andrews' original study. [6] P ≤ 0.05 was considered to be significant.
| Results | | |
- The pre and post treatment comparison values of angulation of the upper 2 nd premolar, 1 st and 2 nd molar, lower central and lateral incisor showed statistically very high significance and high significance was noted with lower 1 st and 2 nd molar, whereas significant changes was noted with upper central and lateral incisor and no significant changes was noted with upper canine, lower canine, and 2 nd premolar [Table 1] and [Graph 1 [Additional file 1]].
- The pre and post treatment comparison values of inclination of the upper lateral incisor, lower central and lateral incisor and canine showed statistically very high significance and high significance was noted with upper central incisor and 2 nd premolar, whereas no significant changes was noted with upper canine, 1 st and 2 nd molar, lower 2 nd premolar and 1 st and 2 nd molar [Table 2] and [Graph 2 [Additional file 2]].
- The post treatment angulation and inclination values when compared with MBT values showed a mean difference of which was ±2.1° for the tip and ±11.9° for torque [Table 3] and [Graph 3 [Additional file 3]].
- The difference of radiographic measurements and cast measurements showed a very high significance in lower incisor for the tip and torque but was not significant in upper incisor [Table 4] and [Graph 4 [Additional file 4]].
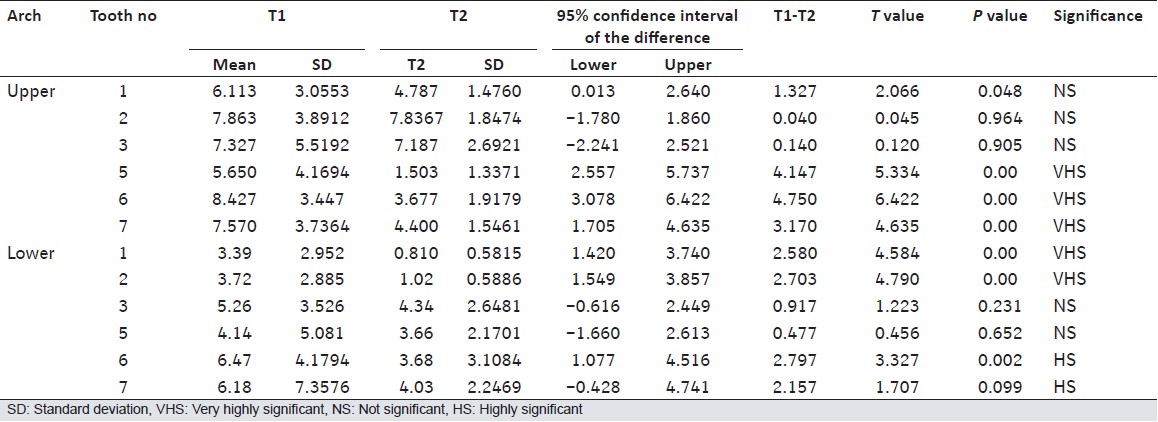 | Table 1: Comparison of pretreatment (T1) and posttreatment (T2) angulation values
Click here to view |
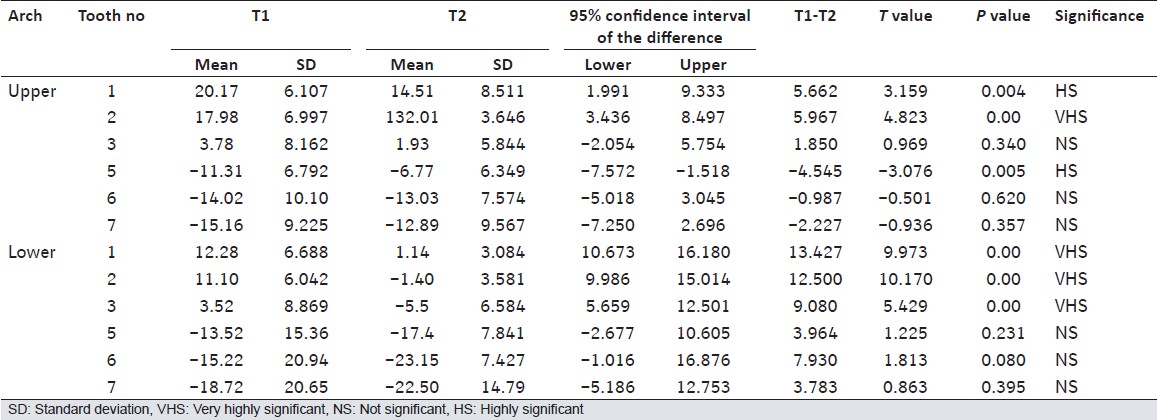 | Table 2: Comparison of pretreatment (T1) and posttreatment (T2) inclination values
Click here to view |
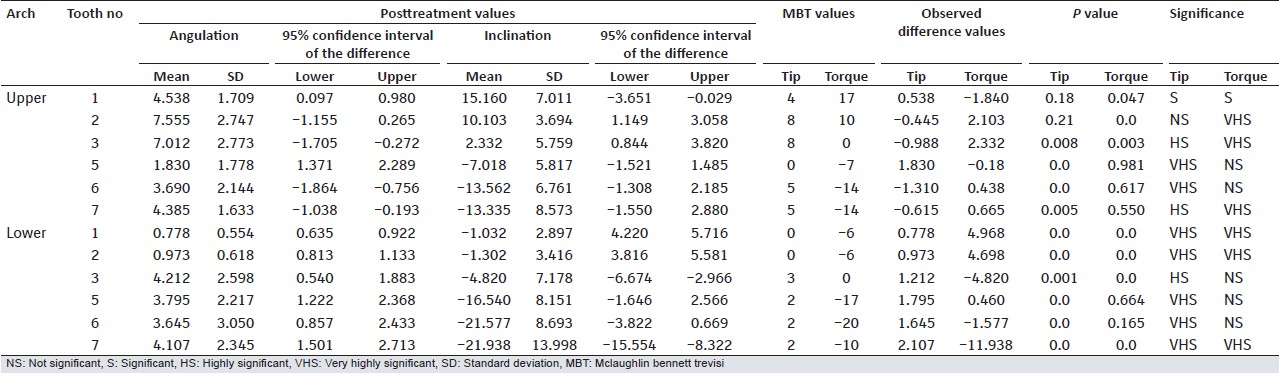 | Table 3: Comparison of posttreatment angulation (tip) and inclination (torque) values with MBT values
Click here to view |
 | Table 4: Comparison of radiographic pre and posttreatment tip and torque values with TAD measurements
Click here to view |
| Discussion | | |
MBT appliance system is the latest of such preadjusted appliances which introduced a range of improvements and specification changes to overcome the clinical shortcomings of the earlier systems. [3]
Tip or Crown Angulation
In normal occlusion, this is seen as a distal inclination of the gingival portion of each crown i.e., positive tip. [7] This was the finding in the present study where all teeth at the posttreatment stage showed a positive tip. Regarding individual teeth, maxillary 2 nd premolar, 1st and 2 nd molar, mandibular central and lateral incisor showed statistically very high significant changes in tip during treatment. Tip measurements for maxillary 2 nd premolar showed a mean decrease of 4.14°, 1 st molar showed 4.75°, 2 nd molar showed 3.17°, mandibular central incisor showed 2.58° and lateral incisor showed 2.7° during the treatment [Table 1].
According to the proponents of the MBT system, with light continuous force mechanics, tip can be well controlled and are fully and rapidly expressed in clinical use. [3] Present study posttreatment tip values point to similar findings:
In the maxillary arch, the MBT tip values for none of the teeth fall in the 95% confidence limits. MBT tip of 0° for maxillary 2 nd premolar is only slightly less than the lower limit of 95% confidence limits for this tooth (1.77-1.37°) [Table 1].
In the mandibular arch, MBT tip values for 1 st and 2 nd molars (2°), fall between the 95% CIs of the posttreatment measurements in the present study (0.85-2.43° and 1.50-2.71°, respectively). MBT tip of 2° for mandibular 2 nd premolars is only slightly less than the lower limit of 95% confidence limits for this tooth (−1.37-2.28°) [Table 1].
In the maxillary arch, tip measurements for central incisor, canine, 2 nd premolar, 1 st and 2 nd molars showed statistically significant difference from MBT tip measurements, except for maxillary lateral incisor. In the mandibular arch, tip measurements for all the teeth showed statistically significant difference from MBT tip values [Table 3].
Torque or Crown Inclination
The present study sample consisted of cases with bi-maxillary dentoalveolar protrusion whose treatment involved four 1 st premolar extractions. Posttreatment occlusion showed a considerable reduction in torque of upper anteriors 5.66°, 5.96° and 1.98°, respectively as well as lower anteriors 13.42°, 12.5° and 9.08°, respectively after treatment [Table 2] which was statistically significant, indicating an expected progress toward the treatment goals.
The treatment changes for maxillary as well as mandibular 2 nd premolars and 1 st molars were statistically nonsignificant.
In the present study, MBT torque values [4] for all the teeth in maxillary and mandibular arch fall between the 95% CIs of the posttreatment measurements [Table 2].
Problems with expression of torque values built into the appliance may be due to two mechanical reasons. First, area of torque application is small and depends on the twist effect of a relatively small wire, compared with the bulk of the tooth. Second, in order to slide teeth we use 0.19" × 0.25" steel wires in 0.22 slot reason being that a full thickness wire prevents sliding. This 0.19" × 0.25" stainless steel wires have a "slop" or "play" of about 10°, depending on the tolerances in the bracket and wire manufacturing and the amount of wire edge "rounding." [3]
The maxillary lateral incisors torque value (10°) is only slightly higher than the upper limit of the 95% CIs for this measurement (1.14-3.05°) and when compared to MBT torque value (7.83° ± 1.83°), the posttreatment measurement is significantly higher [Table 1].
Though full torque built into the appliance was not expressed, yet maxillary incisors showed posttreatment torque closer to MBT values. This might be attributed to the effectiveness of the appliance, but the pretreatment high torque measurements of these teeth might as well be responsible for adequate posttreatment torque.
High pretreatment torque measurements might also be responsible for positive posttreatment torque of mandibular incisors. Several reasons being;
Increase in labio-lingual inclination of mandibular incisors may also occur during leveling of the curve of spee and elimination of lower incisor crowding. [1] The labio-lingual inclination of lower incisors has been found to decrease as the mandibular plane angle increases and vice versa, [8] which demonstrates that different norms need to be used, depending on the underlying skeletal patterns. [3] The present study included only the subjects with an average mandibular plane angle to eliminate the effect of this variable.
In the upper arch, there was no much significant difference from MBT torque values in the following teeth; maxillary central and lateral incisors, 2 nd premolar, 1 st and 2 nd molar. In the lower arch mean posttreatment torque measurements of the tooth 2 nd premolar and 1 st molar showed no much difference from MBT torque values [Table 3].
Despite the fact that the full amount of torque built into the MBT appliance was not expressed, but were significantly higher than Andrews' values for these teeth. While designing the MBT bracket system, it was considered necessary to build extra torque into the important incisor and molar regions in order to meet clinical goals.
| Summary and Conclusions | | |
Pretreatment and posttreatment study models of 30 subjects who received full fixed appliance treatment involving four 1 st premolar extractions using the MBT appliance system were measured for the tip and torque values using TAD. Treatment changes were analyzed statistically and the posttreatment measurements were compared with the MBT prescription values for the above mentioned parameters.
The results indicated that the inbuilt tip was almost fully expressed in all teeth except for the maxillary-2 nd premolar, 1 st molar, mandibular-canine, mandibular 2 nd premolar, mandibular 1 st and 2 nd molar where the discrepancy was only around 1°.
Torque was sufficiently expressed in maxillary-2 nd premolar, first and 2 nd molar and mandibular-2 nd premolar, with a discrepancy between 0° and 0.5°. Torque was under expressed in maxillary-central incisor by 1.8°, 1 st molar by 1.5° and 2 nd molar by 11.9°. Torque was over expressed in maxillary-lateral incisor by 2.1°, canine by 2.4° and mandibular-central and lateral incisor by 4.9° and 4.6°, canine by 4.8°.
Deviation around the mean measurements was found for all the parameters in all teeth. Keeping in account of individual bracket positioning errors it would be fair to anticipate that MBT appliance would result in reasonably optimal tooth positioning at the end of the treatment without any manual archwire adjustments. Tip was comparatively better expressed when compared with torque.
| Acknowledgment | | |
The first author would like to thank all the other authors and other teaching and nonteaching Faculty of Orthodontics Department, Yenepoya Dental College, Yenepoya University, Mangalore for all the support during the study.
| References | | |
| 1. | Thickett E, Taylor NG, Hodge T. Choosing a pre-adjusted orthodontic appliance prescription for anterior teeth. J Orthod 2007;34:95-100. 
|
| 2. | Andrews LF. Straight Wire, the Concept and Appliance. San Diego: L. A. Wells; 1989.
|
| 3. | McLaughlin RP, Bennet JC, Trevisi HJ. Systemized Orthodontic Treatment Mechanics. Wolfe, London, Mosby; 2001.
|
| 4. | Knösel M, Attin R, Kubein-Meesenburg D, Sadat-Khonsari R. Cephalometric assessment of the axial inclination of upper and lower incisors in relation to the third-order angle. J Orofac Orthop 2007;68:199-209.
|
| 5. | Jotikasthira D, Sheffield P, Kalha A, Syed Z. Crown angulation and inclination of Northern Thais with good occlusion. World J Orthod 2010;11:71-4.
|
| 6. | Raghuraj MB. Evaluation of efficacy of the MBT appliance in expressing the inbult tip and torque values - Using torque angulation devic. Dissertation Submitted To Yenepoya University Mangalore, India; 2012.
|
| 7. | Andrews LF. The six keys to normal occlusion. Am J Orthod 1972;62:296-309.
[PUBMED] |
| 8. | Roth RH. Treatment mechanics for the straight-wire appliance. In: Graber LW, Swain BF, editors. Orthodontics, Current Principles and Techniques. St. Louis: CV Mosby; 1985. p. 665-716.
|
[Figure 1], [Figure 2], [Figure 3]
[Table 1], [Table 2], [Table 3], [Table 4]
|











 Search Pubmed for
Search Pubmed for