|
 
 |
| ORIGINAL ARTICLE |
|
| Year : 2015 | Volume
: 3
| Issue : 1 | Page : 4-10 |
|
Study of the effects of oral irrigation and automatic tooth brush use in orthodontic patients with fixed appliances
Dolly Patel1, Falguni Mehta2, Ipsit Trivedi3, Nishit Mehta4, Unnati Shah5, Vijay Vaghela3
1 Department of Orthodontics and Dentofacial Orthopaedics, Ahmedabad Municipal Corporation Dental College and Hospital, Ahmedabad, Gujarat, India
2 Department of Orthodontics and Dentofacial Orthopaedics, Government Dental College and Hospital, Ahmedabad, Gujarat, India
3 Department of Orthodontics, College of Dental Sciences and Research Center, Ahmedabad, Gujarat, India
4 Ahmedabad Dental College, Gujarat, India
5 Graduate student of MPH in Epidemiology, University of Texas Science Health Centre, Houston, Texas, USA
| Date of Web Publication | 29-Dec-2014 |
Correspondence Address:
Nishit Mehta
1, Gyandip Society, Dhumketu Road, Paldi, Ahmedabad - 380 007, Gujarat
India
 Source of Support: None, Conflict of Interest: None  | Check |
DOI: 10.4103/2321-3825.147973

Objective: To compare effectiveness of: 1) Conventional tooth brush alone (control) 2) Powered tooth brush alone 3) Conventional tooth brushing with oral irrigation device 4) Powered tooth brush with oral irrigation device, as home use oral hygiene methods in adult fixed orthodontic patients. Materials and methods: Sixty orthodontic patients with fixed orthodontic appliances were divided into four study groups: (A) brushing with automatic tooth brush twice daily (n = 15); (B) oral irrigation with manual toothbrushing, (n = 15); (C) oral irrigation with automatic tooth brushing, (n = 15); (D) control group with continued normal tooth brushing only, (n = 15). Gingival and plaque indices, bleeding after probing, and gingival sulcus depths were assessed at baseline, 1-month, and 2-month periods. Results: Paired t test was used for within group analysis. Tukey's honestly significant difference (HSD) statistical analysis was used for the inter-group multiple comparisons. Level of significance was at P < 0.05. Within group comparison reveal that there are no statistically significant differences between the groups regarding reductions in gingival index mean scores in all 3 time durations except for group C (P = 0.68) and group D (P = 0.93) in the time period of 1 month to 2 months. After 1 to 2 months use of the automatic tooth brush, there was a significant reduction in plaque when compared with the control group who used only the manual tooth brush (P = 0.04). For this population of orthodontic patients, powered brushes alone or along with oral irrigation do not have additional beneficial effect when comparisons are made with other groups. Conclusion: All plaque control methods evaluated in the study provides significant improvement in reduction of plaque accumulation and gingival inflammation. Powered brushes alone or along with oral irrigation do not seem to be additionally beneficial when comparisons are made with other groups. Keywords: Ortho-Perio relationship, plaque control, manual tooth brush, automated tooth brush, oral irrigation device
How to cite this article:
Patel D, Mehta F, Trivedi I, Mehta N, Shah U, Vaghela V. Study of the effects of oral irrigation and automatic tooth brush use in orthodontic patients with fixed appliances. J Orthod Res 2015;3:4-10 |
How to cite this URL:
Patel D, Mehta F, Trivedi I, Mehta N, Shah U, Vaghela V. Study of the effects of oral irrigation and automatic tooth brush use in orthodontic patients with fixed appliances. J Orthod Res [serial online] 2015 [cited 2018 Sep 6];3:4-10. Available from: http://www.jorthodr.org/text.asp?2015/3/1/4/147973 |
| Introduction | |  |
As orthodontists enter the twenty-first century, the adoption of evidence based health care and invention of the new preventive strategies are primary goals. No matter how talented the orthodontist, a magnificent orthodontic correction can be destroyed by failure to recognize periodontal susceptibility. [1]
One of the most important services that the dentist can render while his patient is under fixed orthodontic treatment is to take proper care of oral hygiene and gingival condition. [2]
Patients undergoing treatment with fixed orthodontic appliances, have an increased risk of plaque accumulation because of increased difficulty in plaque removal. [3] Plaque induced gingivitis is the first step in the disease process, which can progress to attachment loss if kept unchecked. [4]
Mechanical plaque control with conventional tooth brush with proper method forms the important part for maintaining oral hygiene in orthodontic patients.
Previous studies have demonstrated that 20% to 40% of orthodontic patients with fixed orthodontic appliances will show less than ideal plaque removal with conventional tooth brushes even with repeated instructions. [5],[6]
Two of those considered beneficial adjuncts to manual tooth brushing are: Automatic (powered) tooth brushes and water irrigation devices. [7]
Automatic (powered) tooth brushes have specifically been shown to improve oral health for patients with fixed orthodontic appliances. [7]
Oral Irrigators are shown to be particularly helpful for removing debris from inaccessible areas around fixed orthodontic appliances. When used as adjuncts to tooth brushing, these devices can have a beneficial effect on periodontal health. [7]
Reports and studies regarding automatic tooth brush and oral irrigation devices used in orthodontic patients in comparison with conventional tooth brush alone are controversial. Some report significant benefits, [7] whereas others report no difference. [8]
Study by James G. Burch showed significant reductions in plaque, gingival inflammation, and a tendency for reduced bleeding after probing. These improvements were most attributable to the effect of the oral irrigation device. [7] Similarly, study by Wilcoxon showed that plaque and gingival scores were significantly less after brushing 2 months with the counter rotational power brush than with the manual brush. [8] In contrast, study by Hickman showed no measurable differences between the powered toothbrush with modified orthodontic brush head and a manual tooth when used by patients wearing fixed appliances. [9] Similarly, study by Jackson showed no significant difference between the means for plaque and gingival health in each group represented by manual or electric tooth brush alone or with irrigation device. [10]
Further, the present study is undertaken to clarify the effects of these adjuncts in improving gingival health in fixed orthodontic patients, in combination with conventional method of brushing or alone.
| Aims and Objectives | | |
The present study is conducted to compare effectiveness of conventional tooth brush alone (control), powered tooth brush alone, conventional tooth brushing with oral irrigation device and powered tooth brush with oral irrigation device as home-use oral hygiene methods in patients undergoing fixed orthodontic treatment with regard to gingival health using plaque and gingival for a 2-month period.
| Materials and Methods | | |
- The present study was carried out in the Department of Orthodontics, Government dental College and Hospital, Ahmedabad with sixty patients being treated by fixed preadjusted edgewise labial appliances, between age group of 12-22 years. Approval of the study from ethical committee of the college and informed consent for the study was taken from the patients or patients' parents as the subjects were randomly assigned to various oral hygiene methods.
Criteria for Patient Selection
- Patients treated by non-extraction modality were considered and included, who otherwise had full complement of permanent dentition up to permanent first molars with well aligned upper and lower dental arches without any crowding.
- Patients must have had full fixed pre adjusted edgewise labial orthodontic appliance in place for minimum of one month with the clinical diagnosis of generalized gingivitis at the beginning of study.
- At the time of study 24 teeth-central incisors to first molar in all 4 quadrants were taken into account. All permanent teeth were bonded except first permanent molars, which were banded.
- The medical history was reviewed to exclude anyone with a history of heart murmur, rheumatic heart disease, rheumatic fever, mitral valve prolapse, cardiovascular problems or history of any condition, which might put them at risk of bacteremia.
- Pregnant patients or patients planning pregnancy within next three months or if were taking antibiotics were excluded.
Sixty subjects were divided in four groups randomly, each group having fifteen subjects. Groups were named A, B, C and D by the researcher and these naming was not disclosed to the evaluator for the whole duration of the study for blinding.
Groups
Group A: Subjects in this group were instructed to do brushing twice daily with automatic tooth brush (Oral B Cross Action Dual Clean Electric Toothbrush, India) for two minutes (as instructed by manufacturer) in place of the conventional one. The powered toothbrush provided to the patient had two movements: Rotating and Oscillating.
Group B: Subjects in this group were instructed to use oral irrigation device with orthodontic tip (The Waterpik® Cordless Plus Water Flosser, USA) along with the conventional brushing. The device used was capable of producing pulsating stream of water with exit pressure ranging from 45 to 75 psi, having a capacity of 210 ml in the reservoir. They were instructed to brush manually using modified bass method and then use irrigation on all surfaces of teeth, total irrigation time being one minute as recommended by the manufacturer.
Group C: Subjects in this group were instructed to use automatic tooth brush instead of the conventional one every day twice for two minutes followed by irrigation with orthodontic tip (The Waterpik® Cordless Plus Water Flosser, USA) as described in group B.
Group D: This was a control group in which the patients were asked to continue brushing with conventional tooth brush (Oral B Pro Health All in one toothbrush, India). They were instructed to do brushing with modified bass method. It was made sure that subjects were using conventional tooth brush complying with American Dental Association (ADA) specifications of design.
Subjects in all groups were instructed to use fluoridated but without any periodontal medicated toothpaste.
All subjects were evaluated at 3 sequential appointments.
Baseline
At 1 month
At 2 months
As for compliance, each subject was given a sheet containing the dates of two months and subjects were instructed to mark on a given date two times, when procedure was performed by them.
Before checking the gingival health parameters, erythrosine disclosing agent was applied to patients' teeth and marginal gingiva for disclosing the location and amount of plaque. After ten minutes, subjects were asked to gargle gently and then were evaluated by the evaluator (NM) of the study.
Two parameters were measured and recorded for all present teeth up to first molars in all quadrants, of each subject of all the groups thrice at above stated intervals.
The following parameters were recorded:
Plaque Index
Plaque was assessed on buccal and lingual surfaces of all teeth up to permanent first molars in all quadrants by orthodontic modification [11] of Silness and Loe plaque index. [12] The plaque component of this index divides the buccal surface of each tooth into four zones, according to the position of the bracket: Incisal, distal, mesial and gingival to the bracket. And codes 0-3 were assigned.
Palatal or lingual surface was considered as one area:
0. No plaque visible
1. A film of plaque adhering to the free gingival margin and adjacent area of tooth, which may be recognized only by running a probe across the tooth surface.
2. Moderate accumulation of soft deposits within the gingival pocket and on gingival margin and/or on adjacent tooth surface, which can be seen by the naked eye.
3. Abundance of soft matter within the gingival pocket and/or on the gingival margin and on the adjacent surface of tooth.
A briault probe, which has two angled ends was used to differentiate code 0 from code 1, since it could be maneuvered around the brackets.
Calculation of the Index
For each tooth, the scores of five areas were added and then divided by five. This gives the plaque index for the tooth. The scores of individual teeth were totaled and divided by number of teeth. This gave plaque index for that individual.
Gingival Index
Modification of gingival index by Loe [13] was used.
All teeth up to permanent first molars were considered. The tissues surrounding each tooth were divided into four gingival scoring units: Distal-facial papilla, facial margin, mesial-facial papilla and the entire lingual gingival margin.
A blunt instrument such as a periodontal pocket probe was used to assess the bleeding potential of the tissues.
Each of the four units was assessed according to the following criteria:
0. Absence of inflammation/normal gingiva.
1. Mild inflammation, slight change in color, slight edema; no bleeding on probing.
2. Moderate inflammation; moderate glazing, redness, edema and hypertrophy. Bleeding on probing.
3. Severe inflammation; marked redness and hypertrophy ulceration. Tendency to spontaneous bleeding.
Calculation of the Index
The scores around each tooth were totaled and divided by four, which gave the gingival index for the tooth. Summing up all the scores per tooth and dividing by the number of teeth, provided the gingival index score for that subjects.
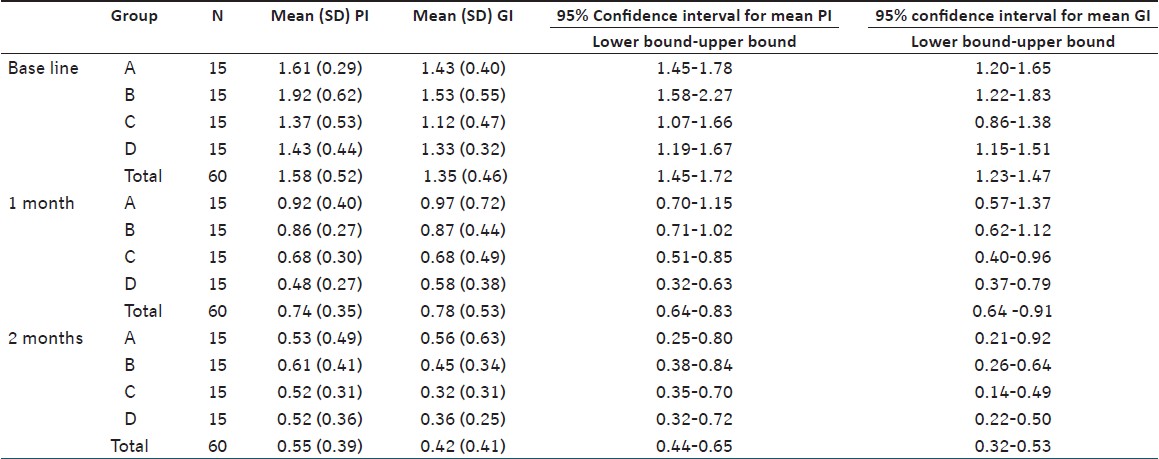
An oral hygiene form for recording the indices was prepared for each patient. An unbiased evaluator who was a post-graduate student in periodontics was appointed for evaluation of indices for each patient on each appointment. Once the data was collected, appropriate statistical analyses were employed. Mean were calculated for the four groups at baseline, 1 month and 2 months for both plaque and gingival indices [Table 1]. Paired t test was used for within group analysis. Tukey's HSD statistical analysis was used for the inter- group multiple comparisons. Level of significance was at P < 0.05.
| Results | | |
Group Wise Analysis
Plaque index [Table 2]
Statistical results of within group analysis reveal that samples in all 4 groups demonstrate statistically significant reduction of mean plaque index values in all 3 time durations considered, except in case of group C (powered tooth brush plus oral irrigation) and group D (Conventional tooth brushing) in the time period of 1 month to 2 months. 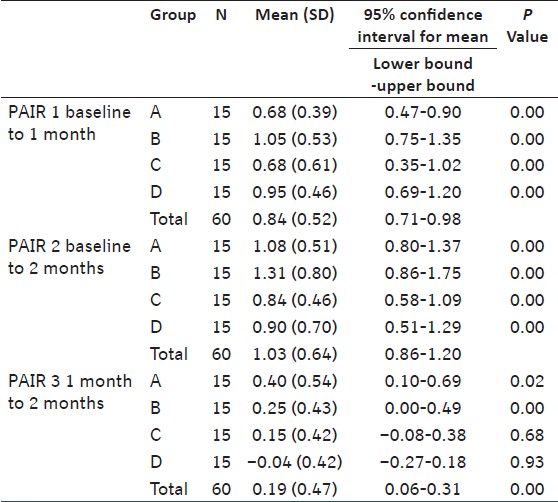 | Table 2: Within group comparison for plaque index (Paired sample t test)
Click here to view |
Gingival index [Table 3]
Statistical results of within group analysis reveal that samples in all 4 groups demonstrate statistically significant reduction of mean gingival index values in all 3 time durations.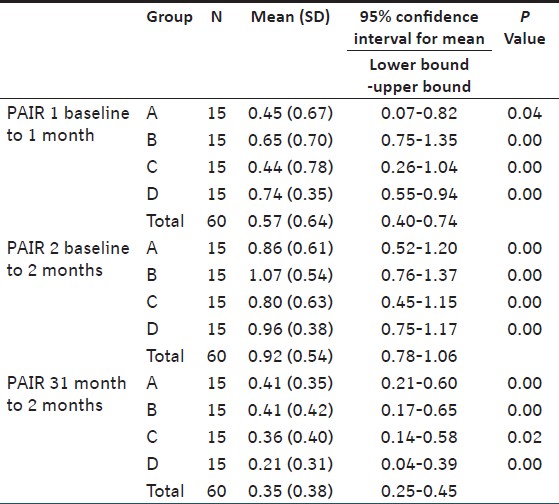 | Table 3: Within group comparison for gingival index (Paired sample t test)
Click here to view |
Between group analysis
Plaque index [Table 4]
Statistical analysis of inter-group comparison reveal that there are no statistically significant differences between the groups regarding reductions in plaque index mean scores in all 3 time durations except between group A and D regarding the reduction in mean PI scores from 1 month to 2 months. In this particular comparison, group A showed statistically significantly more reduction than group D for PI for this particular time period [Table 4].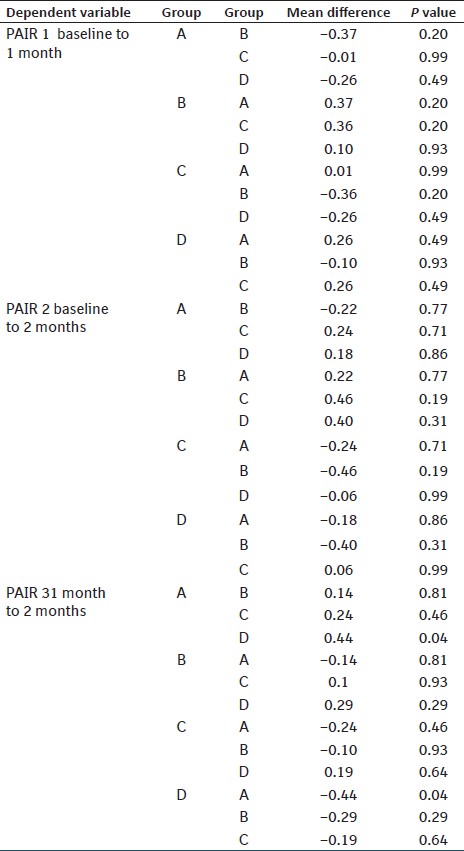 | Table 4: Comparison of changes in values of plaque index between all groups in 3 �� me periods (Tukey HSD test)
Click here to view |
Gingival index [Table 5]
Inter-group comparison reveals that there are no statistically significant differences between the groups regarding reductions in gingival index mean scores in all 3 time durations.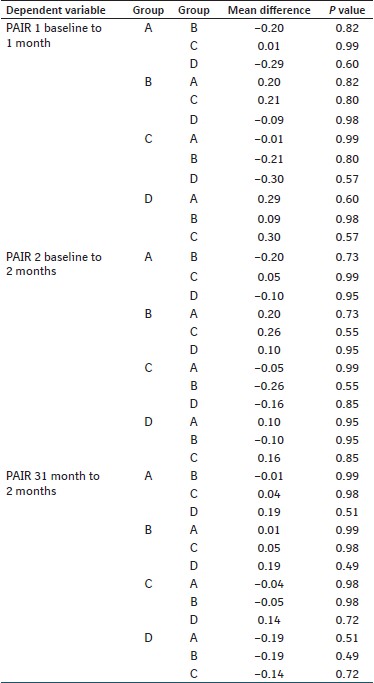 | Table 5: Comparison of changes in values of gingival index between all groups in 3 �� me periods (Tukey HSD test)
Click here to view |
| Discussion | | |
Mechanical plaque control plays most important role in maintaining oral hygiene in orthodontic patients. According to some previous studies, traditional methods alone might not be appropriate or sufficient because of increased plaque retention and limitations in access. [14]
Power toothbrushes have been studied extensively in non-orthodontic patients and have demonstrated beneficial outcomes in supragingival plaque removal and gingival health when compared with manual toothbrushes. [15] Some power tooth brushes have also been studied with orthodontic subjects but rarely were superior to manual brushes. [16],[17] Heasman et al. [16] , Hickman et al.[9] and Costa et al.[17] showed no measurable differences between the powered toothbrush with modified orthodontic brush head and a manual tooth when used by patients wearing fixed appliances.
The use of oral irrigation device has consistently shown significant improvements in gingivitis and bleeding in addition to pro-inflammatory mediators interleukin-1 beta (IL-1B) and Prostaglandin E (PGE 2 ). [18] Unlike conventional brushing, a dental water jet was shown to remove sub-gingival pathogenic bacteria. [19] Though some of the studies in orthodontic patients with fixed appliances show no significant improvement Jackson showed no significant difference between the means for plaque and gingival health in each group represented by manual or electric toothbrush alone or with irrigation device. [10]
Present study evaluated automatic tooth brush and conventional tooth brush alone and as an adjunct to oral irrigation, in patients with fixed orthodontic appliances having band on 1 st permanent molars.
Subjects in the present randomized clinical study attended a single researcher and a single evaluator during the study duration. The evaluator was kept blind regarding the group of the subjects. All subjects were having a similar preadjusted edgewise fixed appliance therapy, with all the appliance components from the same manufacturer and were only accepted for the study if they had been under strap up for at least 1 month and having a clinical diagnosis of generalized gingivitis. For obtaining further uniformity in the baseline, only subjects with good alignment were selected.
The 2-month period of the present study satisfies the recommendation in the ADA acceptance program guidelines for tooth brushes that the study should be conducted over at least thirty days. [20] However, the improvement in plaque scores over the 2-month study period in all groups may well be attributed to the requirement for a timed cleaning period, and the Hawthorne effect as a result of participating in the study. Extending the study to at least 6 months could have reduced the potential Hawthorne effect and enable the effect of adjuncts on plaque and gingivitis around orthodontic fixed appliances to be more thoroughly evaluated. [20] In a study by Ainamo [21] , the effects of powered tooth brush were safe and superior than manual tooth brush in improving gingival health, these differences being statistically significant at 6 and 12 months, but not yet apparent at 3 months; however, no differences in the overall plaque scores were apparent at any of the examinations.
The number of patients included in each group were same as that of Burch's [7] study (15 in each), which is more than Jackson's study group. [10] Age group used by Burch [7] was adult (21-48 years), which was different than the present study which has the age group of 12-22. This age group is more representative of the patients, who usually undergo fixed orthodontic treatment and may signify the results obtained here. However, the variability in use and compliance may be questioned.
In the present study, significant reduction in plaque and gingival indices (P < 0.05) are found in all the four groups from baseline to 2 months [Table 2] and [Table 3]. Moreover, during 2 months of use of the automatic tooth brush and the conventional tooth brush alone or as adjuncts to oral irrigation, there are statistically insignificant differences (P > 0.05) in the improvement observed between the groups [Table 4] and [Table 5]. So the magnitudes of differences among the four groups are small. This shows that oral irrigation with conventional tooth brushing do not have statistically significant differences with other groups with regard to improvements in gingival health. These results are same as those obtained by Jackson [10] but in contrast with the result achieved by Burch [7] , who found statistically significant differences between two test groups they used and the control group.
In the present study, the largest reduction in plaque index occurs within the first month of the investigation [Table 2] and [Table 4]. Further reductions between the 1-month follow up and the 2 - month follow up were relatively small but were significant [Table 2] and [Table 4]. This particular pattern of reduction between different time period was also noted in the study by Burch [7] . In contrast to plaque index, gingival index reduction occurs relatively more from 1-month follow-up to 2-month follow-up for all groups, may be due to better plaque control achieved in the previous month.
In a study by Jackson [10] , he reported no statistically significant benefit to the orthodontic patient from using an automatic tooth brush, a water irrigation device, or a combination of the two. These were the same results obtained in present study except for the fact that the group B (conventional tooth brush plus oral irrigation) showed slightly better improvement in both the indices, though statistically insignificant [Table 4] and [Table 5]. This shows that in our study, powered brushes alone or along with oral irrigation do not seem to be additionally beneficial when comparisons are made with other groups. In contrast, the study by Burch et al.[7] for the age group 21-48 years, showed that daily water irrigation, with manual or electric brushing, provided significant improvement in gingival inflammation after 2 months.
| Conclusion | | |
- All plaque control methods evaluated in the study provides significant improvement in reduction of plaque accumulation and gingival inflammation.
- Powered brushes alone or along with oral irrigation do not have additional beneficial effect when comparisons are made with other groups.
- Oral irrigation with conventional tooth brushing do not have statistically significant differences with other groups with regard to improvements in gingival health.
| References | | |
| 1. | Vanarsdall RL Jr., Secchi AG. Periodontal-orthodontic interrelationships. In: Grabar TM, Vanarsdall RL Jr, Vig KW, editors. Orthodontics: Current Principles and Techniques, Mosby: St. Louis; 2005.  |
| 2. | Graber TM. Dental care during orthodontic therapy. In: Graber TM, editor. Orthodontics Principles and Practice. Philadelphia: WB Saunders; 2001. |
| 3. | Boyd RL. Periodontal considerations during orthodontic treatment. In: Bishara SE, editor. Textbook of Orthodontics. Philadelphia: Saunders; 2001. |
| 4. | Proffit WR, Fields HW, Sarver DM. Special considerations in treatment for adults. In: Proffit WR, Fields HW, Sarver DM, editors. Contemporary Orthodontics. Mosby: St. Louis; 2007. |
| 5. | Boyd RL, Leggott PJ, Quinn RS, Eakle WS, Chambers D. Periodontal implications of orthodontic treatment in adults with reduced or normal periodontal tissues versus those of adolescents. Am J Orthod Dentofacial Orthop 1989;96:191-9. |
| 6. | Alstad S, Zachrisson BU. Longitudinal study of periodontal condition associated with orthodontic treatment in adolescents. Am J Orthod Dentofacial Orthop 1979;76:277-86. |
| 7. | Burch JG, Lanese R, Ngan P. A two-month study of the effects of oral irrigation and automatic toothbrush use in an adult orthodontic population with fixed appliances. Am J Orthod Dentofacial Orthop 1994;106:121-6. |
| 8. | Wilcoxon DB, Ackerman RJ Jr, Killoy WJ, Love JW, Sakumura JS, Tira DE. The effectiveness of a counterrotational-action power toothbrush on plaque control in orthodontic patients. Am J Orthod Dentofacial Orthop 1991;99:7-14. |
| 9. | Hickman J, Millett DT, Sander L , Brown E, Love J. Powered vs manual tooth brushing in fixed appliance patients: A short term randomized clinical trial. Angle Orthod 2002;72:135-40. |
| 10. | Jackson CL. Comparison between electric toothbrushing and manual toothbrushing, with and without oral irrigation, for oral hygiene of orthodontic patients. Am J Orthod Dentofacial Orthop 1991;99:15-20. [ PUBMED] |
| 11. | Williams P, Clerehugh V, Worthington HV, Shaw WC. Comparison of two plaque indices for use in fixed orthodontic appliance patients. J Dent Res 1991;70:703. |
| 12. | Silness J, Loe H. Periodontal disease in pregnancy. II. Correlation between oral hygiene and periodontal condition. Acta Odontol Scand 1964;22:121-35. |
| 13. | Loe H. The gingival index, the plaque index and the retention index systems. J Periodontol 1967;38:610-6. |
| 14. | Sharma NC, Lyle DM, Qaqish JG, Galustians J, Schuller R. Effect of a dental water jet with orthodontic tip on plaque and bleeding in adolescent patients with fixed orthodontic appliances. Am J Orthod Detofacial Orthop 2008;133:565-71 |
| 15. | Tritten CB, Armitage GC. Comparison of a sonic and manual toothbrush for efficacy in supragingival plaque removal and reduction in gingivitis. J Clin Periodontol 1996;23:641-8 |
| 16. | Heasman P, Wilson Z, Macgregor I, Kelly P. Comparative study of electric and manual toothbrushes in patients with fixed orthodontic appliances. Am J Orthod Dentofacial Orthop 1998;114:45-9. |
| 17. | Costa MR, Silva VC, Miqui MN, SakimaT, Spolidorio DM, Cirelli JA. Efficacy of ultrasonic, electric and manual toothbrushes in patients with fixed orthodontic appliances. Angle Orthod 2007;77:361-6. |
| 18. | Barnes CM, Russel CM, Reinhardt RA, Payne JB, Lyle DM. Comparison of irrigation to floss as an adjunct to tooth brushing: Effect on bleeding, gingivitis and supragingival plaque. J Clin Dent 2005;16:71-7. |
| 19. | Cobb CM, Rodgers RL, Killoy WJ. Ultrastructural examination of human periodontal pockets following the use of an oral irrigation device in vivo. J Periodontol 1988;59:155-63. |
| 20. | Clerehugh V, Williams P, Shaw WC, Worthington HV, Warren P. A practice-based randomised controlled trial of the efficacy of an electric and a manual toothbrush on gingival health in patients with fixed orthodontic appliances. J Dent 1998;26:633-9. |
| 21. | Ainamo J, Xie Q, Ainamo A, Kallio P. Assessment of the effect of an oscillating/rotating tooth brush on oral health. A 12 month longitudinal study. J Clin Periodontol 1997;24:28-33. |
[Table 1], [Table 2], [Table 3], [Table 4], [Table 5]
|










 Search Pubmed for
Search Pubmed for