|
 
 |
| ORIGINAL ARTICLE |
|
| Year : 2015 | Volume
: 3
| Issue : 1 | Page : 11-16 |
|
Pharyngeal airway parameters in subjects with Class I malocclusion with different growth patterns
Dipti Shastri, Pradeep Tandon, Amit Nagar, Alka Singh
Department of Orthodontics and Dentofacial Orthopaedics, Faculty of Dental Sciences, King George's Medical University, Lucknow, Uttar Pradesh, India
| Date of Web Publication | 29-Dec-2014 |
Correspondence Address:
Dipti Shastri
Department of Orthodontics and Dentofacial Orthopaedics, Faculty of Dental Sciences, King George's Medical University, Lucknow - 226 003, Uttar Pradesh
India
 Source of Support: None, Conflict of Interest: None  | Check |
DOI: 10.4103/2321-3825.146359

Objectives: (1) To test the null hypothesis that there are no significant difference in the pharyngeal airway in subjects with Class I malocclusion with different growth patterns. (2) To test the null hypothesis that there are no significant difference in dentofacial structure in subjects with Class I malocclusion with different growth patterns. Materials and Methods: Lateral cephalometric radiographs of 120 skeletally Class I were separated into three groups according to the SN-MP angle. Lateral cephalometric radiographs of 39 low angle, 45 high angle and 36 normal angle were examined. Group difference were analyzed with analysis of variance (ANOVA) and the Tukey test, at the P < 0.05 level. Results: For pharyngeal airway measurements statistically significant difference were found in pharyngeal airway length, and D5 (retroepiglottal) pharyngeal width. No statistically significant sagittal pharyngeal (D1-D5) parameters difference were determined between low angle and normal angle subjects. High angle subjects had lower sagittal pharyngeal D2 (retropalatal) and D5 (retroepiglottal) parameters than those with low and normal angle, additionally in high angle subjects had lower D1 (retropalatal) and D4 (retroglossal) parameters than those with normal angle subjects. According to ANOVA only 1 out of 9 dentofacial measurements showed not statistically significant difference among different growth patterns. Conclusion: The null hypothesis was rejected. Significant difference in pharyngeal airway measurements and dentofacial morphology of Class I subjects with different growth patterns were identified. Keywords: Cephalogram, growth patterns, normal occlusion, pharynx
How to cite this article:
Shastri D, Tandon P, Nagar A, Singh A. Pharyngeal airway parameters in subjects with Class I malocclusion with different growth patterns. J Orthod Res 2015;3:11-6 |
How to cite this URL:
Shastri D, Tandon P, Nagar A, Singh A. Pharyngeal airway parameters in subjects with Class I malocclusion with different growth patterns. J Orthod Res [serial online] 2015 [cited 2018 Sep 6];3:11-6. Available from: http://www.jorthodr.org/text.asp?2015/3/1/11/146359 |
| Introduction | |  |
The pharynx is a tube-shaped structure formed by muscles and membranes. It is located behind the nasal and oral cavities and larynx, and extends from the cranial base to the level of sixth cervical vertebra and the lower border of cricoids cartilage. Its length is approximately 12-14 cm, and it is divided into three parts: The nasopharynx, oropharynx, and laryngopharynx. In a midsagittal image, the nasopharynx extends from the nasal turbinates to the hard palate; the oropharynx can be subdivided into the retropalatal pharynx, from the hard palate to the caudal margin of the soft palate, and the retroglossal pharynx, which extends from the caudal margin of the soft palate to the base of the epiglottis; and the hypopharynx is from the base of the epiglottis to the larynx. [1]
Sagittal facial growth is seen as downward, and forward growth [2] Isaacson et al. [2] and Schudy [3] indicated that vertical growth of condyles is lesser than vertical growth of facial sutures and alveolar processes, resulting in backward mandibular rotation and bite opening. On the contrary, if vertical growth of condyles is greater than vertical growth of facial sutures and molar areas, forward mandibular rotation and bite closing are seen. Therefore, the ultimate vector of mandibular growth is a consequence of the competition between horizontal and vertical growth. [4]
An interaction occurs between respiratory function and the maxillary and mandibular growth pattern. [5]
Pharyngeal space size is determined primarily by relative growth and size of the soft tissues surrounding the dentofacial skeleton. From adulthood to older age (20-50 years of age), the nasopharyngeal skeleton may change. [6] Craniofacial anomalies, including mandibular or maxillary retrognathism, short mandibular body, and backward and downward rotation of the mandible, may lead to a reduction of the pharyngeal airway passage. [7] Decreased space between the mandibular corpus and the cervical column may lead to changes in posture of the tongue and soft palate posteriorly, may impair respiratory function during the day, and may cause possible nocturnal problems such as snoring, upper airway resistance syndrome, and obstructive sleep apnea. [8]
Some authors [9] have reported associations between vertical growth pattern and obstruction of the upper and lower pharyngeal airways and mouth breathing. If this relationship presents, vertical growth patterns and Class II malocclusions are required to reveal anatomic predisposing factors.
A significant relationship exists between airway space and facial morphology; also, airway space may be affected by conditions such as functional anterior shifting, [10] head posture, [11] sagittal skeletal relation, [12] and maxillary protraction. Consequently, healthy subjects with Class I skeletal malocclusions and vertical growth patterns might have narrower airway passages than healthy subjects with horizontal growth patterns.
Studies involving the pharyngeal airway space relation are somewhat limited in the orthodontic literature and hence this study was undertaken to evaluate: The aims of the study was to compare pharyngeal airway parameters (vertical and sagittal) and dentofacial morphology in a healthy Class I subjects with different vertical growth patterns (low, normal and high angle). For these purpose, the null hypothesis assumed that no significant difference were present in pharyngeal airway measurements and dentofacial morphology of Class I subjects with different vertical growth patterns.
| Materials and Methods | | |
We conducted a study on the lateral cephalometric radiographs from the records of the Department of Orthodontics and Dentofacial Orthopaedics, Faculty of Dental Sciences, King George's Medical University, Lucknow (UP), India. Subjects included had skeletal Class I relationship on the basis of horizontal distance between the perpendicular drawn from Point A and Point B on palatal plane (App-Bpp) (5 mm ± 2 mm), [13] no history of prior orthodontic treatment, natural dentition and no craniofacial anomalies, syndromes, clefting, or symptoms or signs of dysfunction of the masticatory system. Standard lateral cephalometric radiographs with the teeth in habitual occlusion and with the head oriented horizontally with the Frankfort plane were taken with a cephalostat in accordance with standard cephalometric procedures.
The subjects were divided into three groups on the basis of SN-MP angle [Table 1]: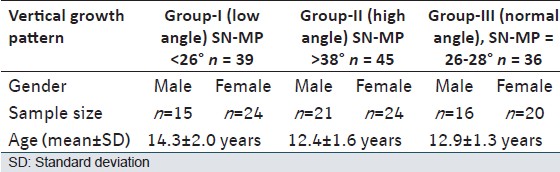 | Table 1: Distribution (sex and number) of subjects by vertical growth pattern and age
Click here to view |
- Group I: Low angle (n = 39)
- Group II: High angle (n = 45)
- Group III: Normal angle (n = 36).
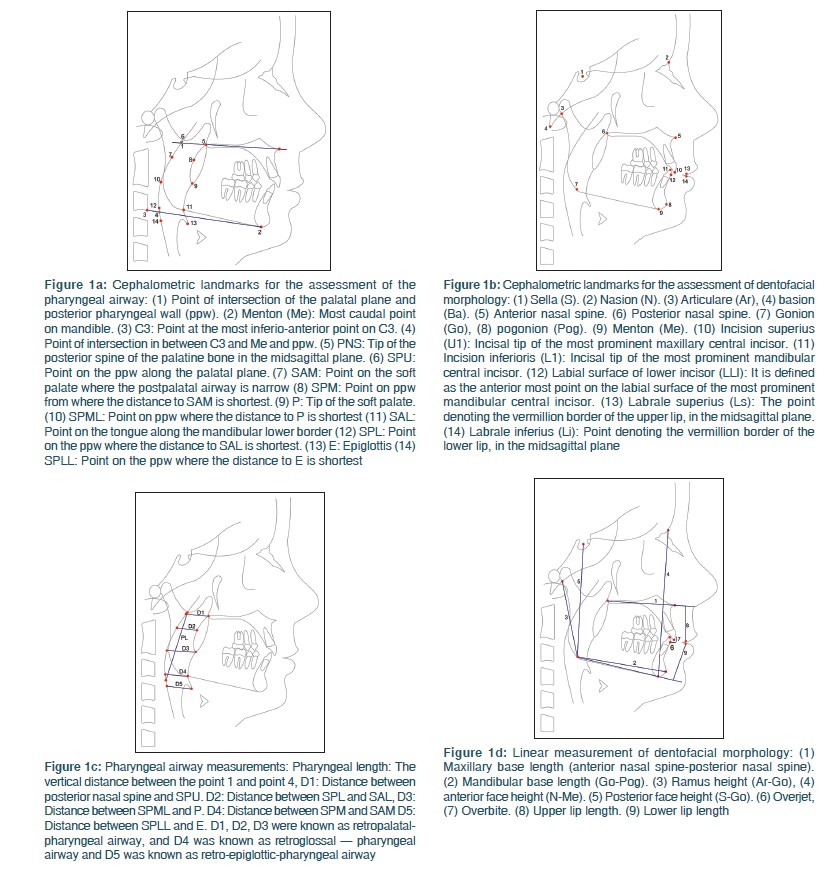
Pharyngeal airway space were evaluated according to Tsai, [14] Sheng et al. [15] All radiographs were traced by hand over an illuminated viewer onto acetate paper, and 14 landmarks were identified [Figure 1]a for pharyngeal linear measurements and another 14 landmarks [Figure 1]b were used to measure linear measurement of dentofacial morphology. There were 1 linear measurement describing pharyngeal length 5 linear items for the pharyngeal airway depth [Figure 1]c, and 9 items describing dentofacial morphology [Figure 1]d and [Table 2].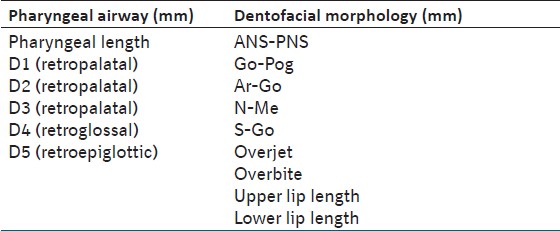 | Table 2: Linear measurement of pharyngeal airway and dentofacial morphology
Click here to view |
All cephalometric landmarks were coordinated with the X- and Y-axis; the X-axis is the Frankfort horizontal (FH) plane and the Y-axis is the line perpendicular to the FH plane from the Sella reference point. Calculations were performed by means of the computerized cephalometric system, Winceph (version 7.0, Rise Co., Japan). Twenty lateral cephalometric radiographs, randomly selected, were traced twice to assess the intra-examiner reliability. Differences between the means of the first and second tracings for each of the variables were tested by means of paired t-test to evaluate the error of the method, and all were well within an acceptable range. Continuous data were summarized in mean ± standard deviation while discrete (categorical) in %. Continuous groups were compared by growth pattern and age. Analysis of variance (ANOVA) and the significance of the mean difference within and between the groups were done by Tukey's honestly significance difference (HSD) post-hoc test. Categorical groups were compared using the Chi-square test. When P < 0.05 was statistically considered as significant. All analyses were performed on STATISTICA (window version 6.0, Rise Co., Japan).
| Results | | |
According to ANOVA, 2 of the 6 measurements showed statistically significant difference among three vertical growth pattern. Significant difference among groups were observed in the pharyngeal length (vertical measurement), D5 (retroepiglottic-pharyngeal depth) [Table 3].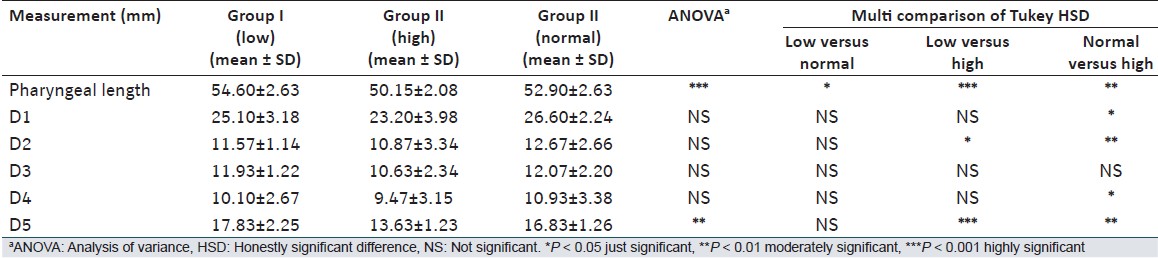 | Table 3: The results of statistics analysis of measurements and comparison (ANOVA) for pharyngeal airway space (length and depth) among different growth pattern (groups)
Click here to view |
Multiple comparisons of the groups in terms of pharyngeal measurements showed that the pharyngeal length (vertical measurement), was decreased from a low angle to normal to high angle subjects. In addition D1, D2, D3 (retropalatal), D4 (retroglossal), were decreased from normal to high angle and D2, D5 (retroepiglottal) were decreased from low to high angle [Table 3].
According to ANOVA results, statistically significant differences were found in all dentofacial parameters except overjet [Table 4].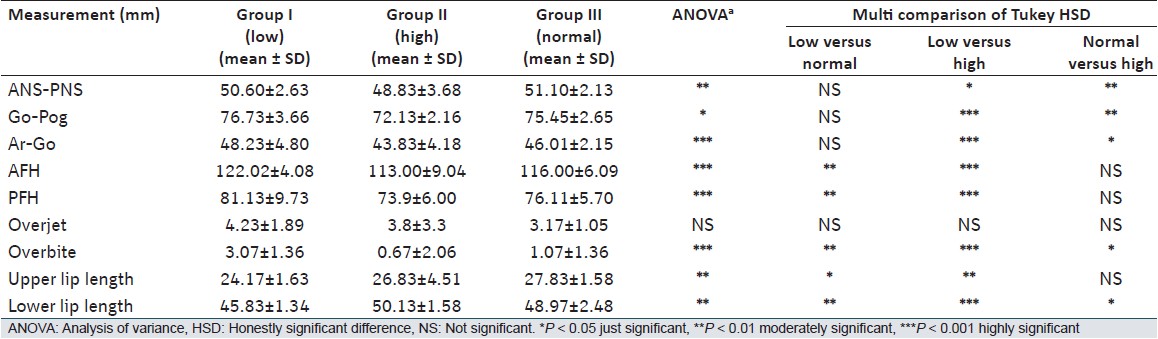 | Table 4: The results of statistics analysis of measurements for dentofacial morphology in all groups
Click here to view |
Pairwise comparisons among groups of dentofacial measurements were also done via the Tukey HSD test. The data demonstrated a significant difference between low angle and high angle groups at the level of the anterior nasal spine-posterior nasal spine (ANS-PNS), Go-Pog, Ar-Go, AFH, PFH, Overbite, upper lip length and lower lip length except Overjet. ANS-PNS, Go-Pog, Ar-Go, AFH, PFH, Overbite and lower lip length decreased from a low angle to normal to high angle. In contrast, overjet decreased from a low angle to high angle to normal. The upper lip length increased from a low angle to high angle to normal. The most significant difference was noted from a low angle to normal to high angle [Table 4].
| Discussion | | |
Good compatibility of age and sex was observed in this cross-sectional study.
This study was performed with two-dimensional cephalometric films to evaluate pharyngeal airway length and depth - not airway flow capacity, which would have required a more complex three-dimensional cone beam computed tomography (CBCT) and dynamic estimation. [12] Therefore, these results do not suggest that individuals with vertical growth patterns have smaller airway flow capacities than those with normal growth patterns. This should be further investigated.
Malkoc et al. [16] has stated that cephalometric films are significantly reliable and reproducible in determining airway dimensions. When computed tomography and cephalometric films were compared in subjects with skeletal malocclusion, Aboudara et al. [17] found a significant positive relationship between nasopharyngeal airway size on cephalometric films and its true volumetric size as determined from CBCT scan in adolescents. Ceylan and Oktay [18] reported that changes in the ANB angle affected nasopharyngeal airway size, and that the oropharyngeal space was reduced in subjects with an enlarged ANB angle. Samples were classified as skeletal Class I, according to the App-Bpp because it was more reliable than ANB. [18]
We selected pharyngeal length in vertical and five sites for sagittal, to know the pharyngeal parameters in both direction simultaneously and sagittaly it studied in five region because during inhalation, the conjoint activity of the intercostals muscles and the diaphragm creates negative airway pressure. Once this pressure surpasses the force generated by the pharyngeal muscles, the pharynx will collapse and occlude the airway. The patency of the pharyngeal airway is mainly dependent on the activity of the oropharyngeal muscles. [19] Three pharyngeal segments tend to collapse - the retropalatal pharynx, the retroglossal pharynx, and retroepiglottic pharynx (posterior to the epiglottis) because the anterior and lateral walls of these segments have no bony support.
Only pharyngeal length showed significant differences between groups, and highly significant difference was seen in between high and low angle group and sagittally increased Go-Pog, PFH and lower lip length in low angle group, and decreased Go-Pog, PFH and lower lip length in low angle group showed a high pharyngeal length in low angle group. An increase in the pharyngeal length occurs mainly in vertical direction. [20],[21]
No statistically significant difference seen in pharyngeal parameters D1, D2, D3, D4 in different growth pattern except D5. Retropalatal parameters showed (D1, D2) significantly higher in normal angle group when compared with high angle group except in D3 it was higher in normal angle, but not significantly. No statistically significant difference in D3 (retropalatal) was noted among groups, and no association of D3 was seen with a different vertical growth pattern. In this study, dentofacial parameters demonstrated that reduced Go-Pog, Ar-Pog and PFH may explain the lack of deficiency in high angle subjects, which may be caused by decrease in dimension of the D1, D2, D3 (retopalatal) part of the airway in high angle subjects. Given all subjects was in skeletal Class I (App-Bpp = 3-7 mm), and the impact of a different sagittal skeletal pattern on the superior part of upper airways was excluded from consideration because sagittal development of mandible has a significant effect on the pharyngeal airway space. [11],[17] It is necessary to include all subjects with similar sagittal development of mandible to eliminate any effect on pharyngeal airway space caused by changes in the sagittal plane, while pharyngeal airway dimensions are evaluated among subjects with different vertical growth patterns. In the current sample, although all subjects had a Class I sagittal relation, decreased Ar-Go in high angle group and increased Ar-Go in low angle group confirmed as forward and upward rotation. In the present study, the vertical pattern affected the retropalatal (D1, D2) and retroepiglottal (D5), and greater retropalatal (D1, D2) and retroepiglottal (D5) was found in low angle subjects than in high angle subjects and study confirms that retroglossal (D4) and retroepiglottal (D5) was decreased only in high angle subjects who had decreased Ar-Go and Go-Pog.
Ucar et al. in another study reported that nasopharyngeal airway space and upper pharyngeal airway space in Class I subjects were larger in low angle subjects than in high angle subjects. [10] We found that the hyperdivergent facial pattern subjects are belonging to skeletal Class I malocclusions showed a statistically significantly the narrow upper pharyngeal airway width when compared to normodivergent and hypodivergent facial patterns. Other researchers found that there is no relationship between upper airway space and the type of malocclusion. [22] However, in the present study statistically significant difference was found in the pharyngeal length between low angle, high angle and normal angle of skeletal Class I subjects, and pharyngeal sagittal width showed different statistical significant value at different region. Furthermore, it is recommended that a similar study with a larger sample size and equal distribution of subjects in various sagittal and vertical facial growth patterns should be conducted to confirm the results of the present study.
| Conclusion | | |
- Statistically, a significant difference were identified in most of the dentofacial measurements among Class I subjects with three different vertical growth pattern.
- Pharyngeal length was found to be larger in low angle subjects than in high angle subjects.
- Retropalatal (D1, D2, D3), retroglossal (D4) and retroepiglottal (D5) in Class I subjects were found to be larger in low angle subjects than in high angle subjects.
| References | | |
| 1. | Schwab RJ. Upper airway imaging. Clin Chest Med 1998;19:33-54.  |
| 2. | Isaacson JR, Isaacson RJ, Speidel TM, Worms FW. Extreme variation in vertical facial growth and associated variation in skeletal and dental relations. Angle Orthod 1971;41:219-29. [ PUBMED] |
| 3. | Schudy FF. The rotation of the mandible resulting from growth: Its implications in orthodontic treatment. Angle Orthod 1965;35:36-50. [ PUBMED] |
| 4. | Chung CH, Mongiovi VD. Craniofacial growth in untreated skeletal Class I subjects with low, average, and high MP-SN angles: A longitudinal study. Am J Orthod Dentofacial Orthop 2003;124:670-8. |
| 5. | Jena AK, Singh SP, Utreja AK. Sagittal mandibular development effects on the dimensions of the awake pharyngeal airway passage. Angle Orthod 2010;80:1061-7. |
| 6. | Johnston CD, Richardson A. Cephalometric changes in adult pharyngeal morphology. Eur J Orthod 1999;21:357-62. |
| 7. | Joseph AA, Elbaum J, Cisneros GJ, Eisig SB. A cephalometric comparative study of the soft tissue airway dimensions in persons with hyperdivergent and normodivergent facial patterns. J Oral Maxillofac Surg 1998;56:135-9. |
| 8. | Ozbek MM, Miyamoto K, Lowe AA, Fleetham JA. Natural head posture, upper airway morphology and obstructive sleep apnoea severity in adults. Eur J Orthod 1998;20:133-43. |
| 9. | Tourné LP. Growth of the pharynx and its physiologic implications. Am J Orthod Dentofacial Orthop 1991;99:129-39. |
| 10. | Ucar FI, Kurt G, Ekizer A, Ramoglu SI. Effects of functional anterior shifting on skeletal and airway structures. Turk J Orthod 2009;22:218-27. |
| 11. | Zhong Z, Tang Z, Gao X, Zeng XL. A comparison study of upper airway among different skeletal craniofacial patterns in nonsnoring Chinese children. Angle Orthod 2010;80:267-74. |
| 12. | Hiyama S, Suda N, Ishii-Suzuki M, Tsuiki S, Ogawa M, Suzuki S, et al. Effects of maxillary protraction on craniofacial structures and upper-airway dimension. Angle Orthod 2002;72:43-7. |
| 13. | Nanda RS, Merrill RM. Cephalometric assessment of sagittal relationship between maxilla and mandible. Am J Orthod Dentofacial Orthop 1994;105:328-44. |
| 14. | Tsai HH. Developmental changes of pharyngeal airway structures from young to adult persons. J Clin Pediatr Dent 2007;31:219-21. |
| 15. | Sheng CM, Lin LH, Su Y, Tsai HH. Developmental changes in pharyngeal airway depth and hyoid bone position from childhood to young adulthood. Angle Orthod 2009;79:484-90. |
| 16. | Malkoc S, Usumez S, Nur M, Donaghy CE. Reproducibility of airway dimensions and tongue and hyoid positions on lateral cephalograms. Am J Orthod Dentofacial Orthop 2005;128:513-6. |
| 17. | Aboudara C, Nielsen I, Huang JC, Maki K, Miller AJ, Hatcher D. Comparison of airway space with conventional lateral headfilms and 3-dimensional reconstruction from cone-beam computed tomography. Am J Orthod Dentofacial Orthop 2009;135:468-79. |
| 18. | Ceylan I, Oktay H. A study on the pharyngeal size in different skeletal patterns. Am J Orthod Dentofacial Orthop 1995;108:69-75. |
| 19. | Benumof JL. Obstructive sleep apnea in the adult obese patient: Implications for airway management. Anesthesiol Clin North America 2002;20:789-811. |
| 20. | Handelman CS, Osborne G. Growth of the nasopharynx and adenoid development from one to eighteeen years. Angle Orthod 1976;46:243-59. [ PUBMED] |
| 21. | King EW. A roentgenographic study of pharyngeal growth. Angle Orthod 1952;22:23-37. |
| 22. | Kerr WJ. The nasopharynx, face height, and overbite. Angle Orthod 1985;55:31-6. [ PUBMED] |
[Figure 1]
[Table 1], [Table 2], [Table 3], [Table 4]
|










 Search Pubmed for
Search Pubmed for