|
 
 |
| CASE REPORT |
|
| Year : 2015 | Volume
: 3
| Issue : 1 | Page : 76-79 |
|
Non-surgical management of unilateral cleft lip and palate in growing patient
Falguni Mehta, Renuka Patel, Vaibhav Gandhi, Manop Agrawal
Department of Orthodontics, Government of Dental College and Hospital, Ahmedabad, Gujarat, India
| Date of Web Publication | 29-Dec-2014 |
Correspondence Address:
Vaibhav Gandhi
D/1, New Anjali Society, Opp Sun Power Flats, Nr. Vishramnagar, Gurukul Road, Memnagar - 380 052, Ahmedabad
India
 Source of Support: None, Conflict of Interest: None  | Check |
DOI: 10.4103/2321-3825.147987

Cleft lip and palate (CLCP) is one of the most common congenital deformities of the craniofacial complex. It has multifactorial etiology with skeletal, dental, soft tissue defects; functional defects such as speech, swallowing, hearing; in addition to psychological and social implications along with facial disfigurement. Thus, the treatment approach is also multidisciplinary involving orthodontist, plastic surgeons, ear-nose and throat surgeon, oral and maxillofacial surgeon, prosthodontist, speech therapist, etc. This case report describes a nonsurgical approach for treating the CLCP patient with rapid maxillary expansion followed by Facemask therapy for protraction of maxilla during the mixed dentition phase to correct the developing malocclusion. Keywords: Cleft lip and palate, nonsurgical approach, rapid maxillary expansion and facemask
How to cite this article:
Mehta F, Patel R, Gandhi V, Agrawal M. Non-surgical management of unilateral cleft lip and palate in growing patient. J Orthod Res 2015;3:76-9 |
How to cite this URL:
Mehta F, Patel R, Gandhi V, Agrawal M. Non-surgical management of unilateral cleft lip and palate in growing patient. J Orthod Res [serial online] 2015 [cited 2018 Sep 6];3:76-9. Available from: http://www.jorthodr.org/text.asp?2015/3/1/76/147987 |
| Introduction | |  |
Cleft lip and palate (CLCP) is one of the most common congenital deformities of the craniofacial complex leading to various dental anomalies in early childhood. The incidence of CLCP is reported to be highest among Afghans as 4.9 and lowest in Negroid population, 0.4/1000 live birth. According to rough estimates, about 30,000 children afflicted with CLCP are born every year. Although organized epidemiological surveys to evaluate CLCP yet to be carried out, >2 dozen studies have been done on newborns in past three decade. From this reports, the pooled incidence for CLCP is estimated to be 1.2/1000 birth and 0.46/1000 for cleft palate alone. [1]
| Case Report | | |
History
A 13-year-old girl reported to our Department of Orthodontics, Government Dental College and Hospital with the chief complaint of irregularly placed teeth. Patient had cleft lip and alveolus on the left side extending through hard palate up to the soft palate which had been surgically corrected (cleft lip at 6 months of age and cleft palate at 1 years of age).
Clinical Examination
Extraoral examination
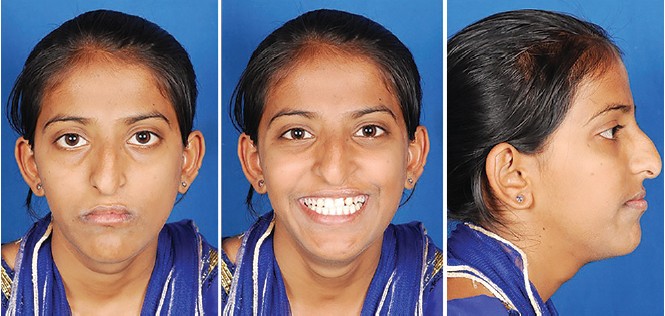
Patient is having leptopropic facial type with normal gait and posture, concave soft tissue profile, shallow mentolabial sulcus, nonconsonant smile arc, wide buccal corridors and scar tissue of cleft lip repair [Figure 1].
Intraoral examination
Intraoral examination is showing right molar in class I and left molar in end on relation. Patient's upper dental midline shifted towards the right side, full upper arch except first molars are in cross bite. Patient having 6 mm reverse overjet and 4 mm over bite with 1 mm curve of spee [Figure 2].
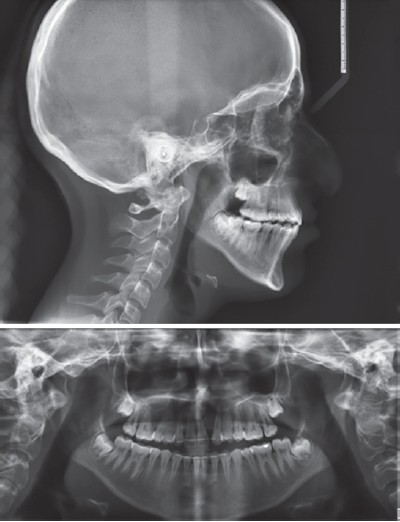
Radiographic examination
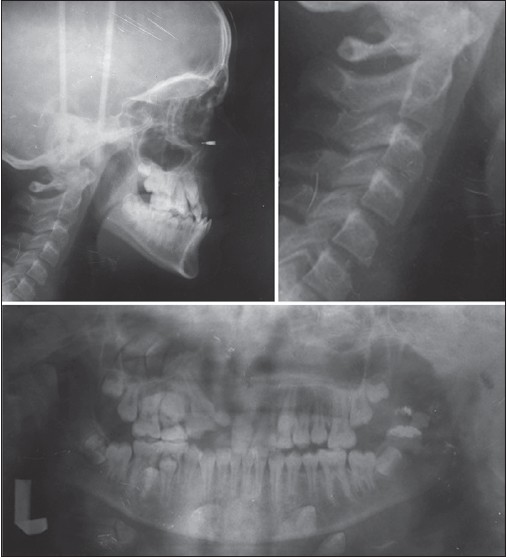
- Orthopantomogram is showing absence of the tooth bud of left and right maxillary lateral incisors. Radiographically upper and lower right second premolars are seen in different the stages of eruption.
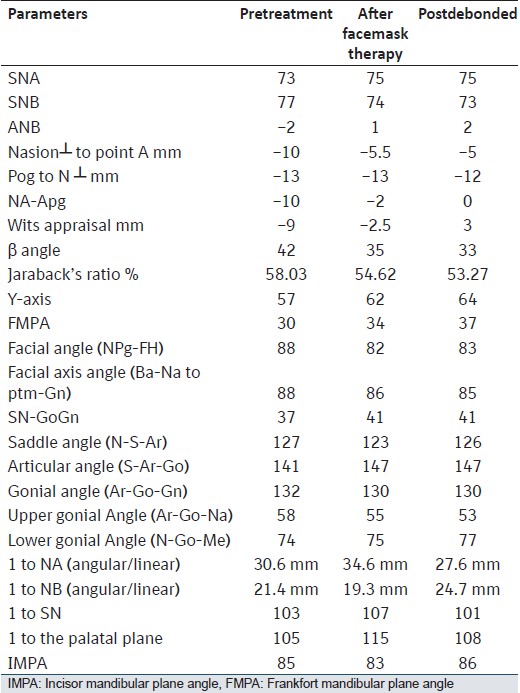
- Lateral cephalogram is showing skeletal class III pattern due to retrognathic maxilla and vertical growth pattern [Table 1]. Cervical Vertebral Maturity Indicator Stage II-Acceleration - 65-85% of adolescent growth expected [Figure 3].
| Diagnosis | | |
Cleft lip and palate patient with partially unrepaired defect behind upper left central incisor, with Angle's Class I molar on the right side and end on molar on the left side imposed over skeletal Class III base relationship with decreased maxillary base length and vertical growth pattern due to downward, and backward rotation of mandible.
Treatment Objective
- Correct the transverse maxillary deficiency.
- Correct the sagittal skeletal base relationship.
- Alignment and leveling of upper and lower arches.
- Correct the upper and lower midlines.
- Achieve ideal overjet and over bite.
- Achieve and maintain Class I molar relation bilaterally
- Improve soft tissue profile and smile
Treatment Plan
Orthodontic-Orthopedic Treatment in mixed dentition.
Once retrusion becomes apparent, clinical options include:
- Allowing abnormal facial development to continue, with surgical intervention after growth is completed.
- Treating with extraoral traction to maxilla. The latter choice minimizes the amount of therapy that will be necessary as the patient matures. Therefore, expansion and protraction of maxilla, secondary bone grafting, are the primary goals during mixed dentition treatment.
Treatment plan was divided into four stages:
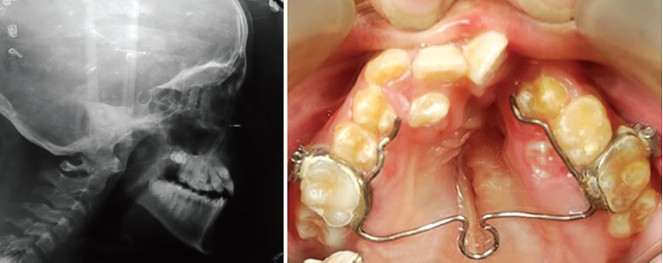
- Rapid maxillary expansion (RME): A banded rapid palatal expansion appliance with Jack screw was cemented, which was activated twice daily (180 degree daily) for 10 days. On the 11 th day, activation of the appliance was stopped. RME screw was sealed using self-cure acrylic [2],[3],[4] [Figure 4].
- Orthopedic correction - for correction of sagittal discrepancy with face mask: The protraction headgear type-2 (petit type) was started using extra oral heavy elastics attached to the RME hooks applying 500 g force on each side for a minimum of 16 h/day. After 6 months of protraction therapy, positive overjet was attained, but the protraction headgear was continued for another 4 months with the same force applied 8-10 h a day to prevent relapse [5],[6],[7],[8] [Figure 5] and [Figure 6]. Later on RME appliance was removed, and extended arm transpalatal arch was given to maintain the corrected transverses relationship [Figure 7].
- Fixed mechanotherapy-dentoalveolar correction with the use of preadjusted straight wire appliance (0.022'' MBT): The teeth were bonded with 0.022'' MBT appliance. Alignment and leveling was done using 016 NiTi wire. Subsequent wire progression was done with 17 × 25 HANT, 17 × 25 SS, 19 × 25 HANT and 19 × 25 SS.
- Retention: Post treatment retention with upper and lower canine to canine fixed retainer with upper and lower Hawley's retention plates.
 | Figure 4: Rapid maxillary expansion appliance with hooks for fackmask therapy
Click here to view |
 | Figure 5: Extraoral photographs after rapid maxillary expansion and facemask therapy
Click here to view |
 | Figure 6: Intraoral photographs after rapid maxillary expansion and facemask therapy
Click here to view |
 | Figure 7: Lateral cephalogram after rapid maxillary expansion and facemask therapy and photograph showing extended arm transpalatal arch
Click here to view |
| Results | | |
With the use of facemask considerable changes have been achieved. SNA improved from 73 to 75, ANB −2 to + 2, Wits appraisal −9 mm to + 3 mm. 5 mm improvement of Nasion┴ to point A has been achieved (from −10 mm to −5 mm). Angle of convexity corrected from −10 to 0 suggesting profile became straight from concave previously. Upper incisor to NA line is changed from 30, 6 mm to 27, 6 mm angular and linear respectively. Same as lower incisor to NB line is changed from 21, 4 mm to 24, 7 mm angular and linear respectively [Table 1] and [Figure 8], [Figure 9] and [Figure 10].
| Discussion | | |
The result shows definite and desirable response to RME as well as facemask therapy. It must be emphasized that result is due to marked orthopedic correction that is maxillary protraction and downward, backward rotation of the mandible. Due to this maxillary protrusive effect there is a marked improvement of the profile. The force vector for facemask passes below the center of the resistance of the maxilla thus dual effect of protraction as well as counter clockwise rotation of the maxilla can be seen. This means maxillary posterior region moves downward leading to clockwise rotation of mandible and opening of mandibular plane angle [Table 1]. As in this case RME appliance with an acrylic coverage was used in the posterior region, which prevents maxillary posterior extrusive effect to a certain extent, downward rotation of mandible as a consequence to the expansion per se, would be minimal.{Table 1}
| Conclusion | | |
Cleft lip and palate cases have always been challenging in clinical practice due to long duration of treatment, compliance due to use of orthopedic appliances and/or orthognathic surgery. Combine team approach is very important aspect for treating cases like this. Early diagnosis and treatment in growing age can avoid jaw surgeries. [9] Here we have treated this case nonsurgically using face mask therapy and RME with acceptable occlusion.
| References | | |
| 1. | Kharbanda OP. Diagnosis and Management of Malocclusion and Dentofacial Deformities. 2 nd ed. New Delhi: Elsevier; 2013. p. 685.  |
| 2. | Garib DG, Henriques JF, Carvalho PE, Gomes SC. Longitudinal effects of rapid maxillary expansion. Angle Orthod 2007;77:442-8. |
| 3. | Gautam P, Zhao L, Patel P. Biomechanical response of the maxillofacial skeleton to transpalatal orthopedic force in a unilateral palatal cleft. Angle Orthod 2011;81:503-9. |
| 4. | Kawakami M, Yagi T, Takada K. Maxillary expansion and protraction in correction of midface retrusion in a complete unilateral cleft lip and palate patient. Angle Orthod 2002;72:355-61. |
| 5. | Khurana G, Arora N, Mogra S, Shetty VS. Role of facemask in correction of skeletal midface deficiency in unilateral cleft lip and palate. J Indian Orthod Soc 2008;42:3-12. |
| 6. | Buschang PH, Porter C, Genecov E, Genecov D, Sayler KE. Face mask therapy of preadolescents with unilateral cleft lip and palate. Angle Orthod 1994;64:145-50. |
| 7. | Nanda R. Biomechanical and clinical considerations of a modified protraction headgear. Am J Orthod 1980;78:125-39. |
| 8. | Jia H, Li W, Lin J. Maxillary protraction effects on anterior crossbites. Repaired unilateral cleft versus noncleft prepubertal boys. Angle Orthod 2008;78:617-24. |
| 9. | Subtelny JD. The importance of early orthodontic treatment in cleft palate planning. Angle Orthod 1957;27:148-58. |
[Figure 1], [Figure 2], [Figure 3], [Figure 4], [Figure 5], [Figure 6], [Figure 7], [Figure 8], [Figure 9], [Figure 10]
[Table 1]
|













 Search Pubmed for
Search Pubmed for