|
 
 |
| ORIGINAL ARTICLE |
|
| Year : 2015 | Volume
: 3
| Issue : 3 | Page : 166-169 |
|
Variation of hyoid bone position in different sexes and different types of skeletal malocclusions
Nidhin Philip Jose1, Siddarth Shetty1, V Surendra Shetty1, Subraya Mogra1, Lida Mary2, Sarvesh Agrawal3
1 Department of Orthodontics, Manipal College of Dental Sciences, Manipal University, Mangalore, Karnataka, India
2 Department of Oral Surgery, Government Dental College and Hospital, Goa, India
3 Department of Orthodontics, Manubhai Patel Dental College, Vadodara, Gujarat, India
| Date of Web Publication | 11-Sep-2015 |
Correspondence Address:
Nidhin Philip Jose
Manipal College of Dental Sciences, Manipal University, Mangalore, Karnataka
India
 Source of Support: None, Conflict of Interest: None  | Check |
DOI: 10.4103/2321-3825.165041

Objective: This study was carried out to ascertain if the position of the hyoid bone demonstrates sexual dimorphism. Materials and Methods: This was a retrospective cross-sectional study conducted using patient records from the institution. Institutional Ethical Committee approval was obtained prior to the study. A total of 60 subjects were divided into three groups and studied. Hyoid triangle analysis by Bibby and Preston was carried out to determine the position of the hyoid bone. All radiographs were traced by a single operator and they were retraced to check for measurement error. Results: Student's t-tests and Mann-Whitney U-test were used to find out whether any sexual dimorphism exists. The horizontal distance from the hyoid bone to the retrognathion was found to be significantly larger in males than in females. The hyoid bone is positioned at a lower level in class I and II in males than in females. Also, it was observed that the hyoid angle was significantly greater in males than in females in class II group. Conclusion: Sexual dimorphism was observed in the sample studied. Keywords: Hyoid bone, sexual dimorphism, skeletal malocclusion
How to cite this article:
Jose NP, Shetty S, Shetty V S, Mogra S, Mary L, Agrawal S. Variation of hyoid bone position in different sexes and different types of skeletal malocclusions. J Orthod Res 2015;3:166-9 |
How to cite this URL:
Jose NP, Shetty S, Shetty V S, Mogra S, Mary L, Agrawal S. Variation of hyoid bone position in different sexes and different types of skeletal malocclusions. J Orthod Res [serial online] 2015 [cited 2018 Sep 6];3:166-9. Available from: http://www.jorthodr.org/text.asp?2015/3/3/166/165041 |
| Introduction | |  |
The hyoid bone is connected to the pharynx, mandible and cranium through muscles and ligaments. [1] It is unique because it is the only bone in the body that has no bony articulations. The hyoid bone is responsible for the careful control of functions like airway maintenance, swallowing, preventing regurgitation and maintaining the upright posture of the head. [2] Obstructive sleep apnea/hypopnea syndrome affects mainly middle-aged males and is known to be associated with a low hyoid bone position among others. [3] Determining the changes in the hyoid bone position in normal healthy subjects will help in planning treatment and further investigations into breathing disorder diseases. [4] There have been numerous attempts to study the differences in its position and shape of the hyoid bone between the male and female sexes. However, there remains a great deal of controversy on the subject. The aim of the study is to determine the position of the hyoid bone in class I, II and III skeletal malocclusions in males and females and to ascertain whether any sexual dimorphism exists in the position of the hyoid bone.
| Materials and Methods | | |
This was a retrospective cross-sectional study conducted using patient records from archives of Department of Orthodontics, Manipal College of Dental Sciences, Manipal University, Mangalore, Karnataka, India. Institutional Ethical Committee approval was obtained prior to the study. A total of 60 subjects were divided into three groups on the basis of antero-posterior skeletal relationships (on the basis of the ANB value) and further into two groups each on the sex of the patients.
- Group 1 Comprising of 20 samples with ANB = 0-3° and SNB = 78-82° (class I skeletal relationship)
- Group 2 Comprising of 20 samples with ANB ≥4° and SNB <78° (class II skeletal relationship)
- Group 3 Comprising of 20 samples with ANB ≤0° and SNB >82° (class III skeletal relationship).
In order to keep the sample standardized, SNB angle was also included in the selection criteria, such that the subjects with class II base have SNB <78°, and class III subjects have SNB >82°.
Each group is subdivided into two according to gender, with 11 females and 9 males in each sub-group respectively.
Inclusion criteria included healthy patients in the age group of 16-25 years with the normodivergent facial pattern (FMA between 21 and 28).
Patients with gross dental abnormalities, oral habits, previous orthodontic treatment history or history of any diseases affecting the pharyngeal structures were excluded.
Standardized lateral cephalograms that fulfilled the inclusion criteria were selected from the departmental archives.
The same cephalostat (PLANMECA proline EC machine) was used for all the radiographs. The radiographic technique was standardized, and the exposure parameters were maintained at 68 kV and 12 mA with a maximum exposure time of 0.5 s, with the focal spot to the mid sagittal plane distance at 5 feet. All cephalograms were developed using high-speed polyester based 18 cm × 24 cm Kodak X-Omat lateral head films and fixed under standardized conditions by the same operator maintaining a magnification of (8%) in all radiographs.
The cephalograms were traced the same operator. A few weeks later, randomly selected cephalograms were retraced by the same operator and the error was noted. During the tracing, in case of discrepancy in bilateral structures, the mean shadow of the bilateral structures is traced in order to minimize minor errors in head positioning and minor skeletal asymmetry.
Hyoid triangle analysis by Bibby and Preston [1] was carried out to determine the position of the hyoid bone.
Statistical analysis
Descriptive statistics including the range, mean and standard deviation were carried out. Kolmogorov-Smirnov and Shapiro-Wilks test was done to check the normality of data distribution.
The results showed the normal distribution for all data apart from the ANB angle and angular and vertical measurement of the hyoid bone.
Student's t-tests and Mann-Whitney U-test were used to find out whether any sexual dimorphism exists. The level of significance is set at P < 0.05. All statistical analysis was carried out with SPSS for windows software (version 13, SPSS Inc., Chicago, III).
| Results | | |
The preliminary Kolmogorov-Smirnov test and Shapiro-Wilks test was used to check the normality of data distribution. The results showed the normal distribution for all data apart from the ANB angle and angular and vertical measurement of the hyoid bone.
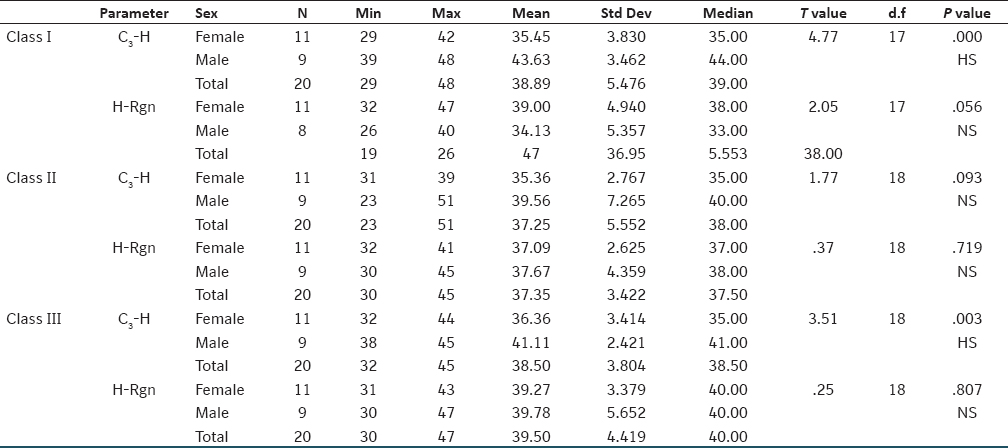
The results of the Student's t-test [Table 1] revealed that the horizontal distance from the cervical vetebrae to the hyoid bone was significantly larger in males than females in both class I and III groups. However, no significant sexual dimorphism was found in the class II group and in the horizontal distance from the hyoid bone to the retrognathion.
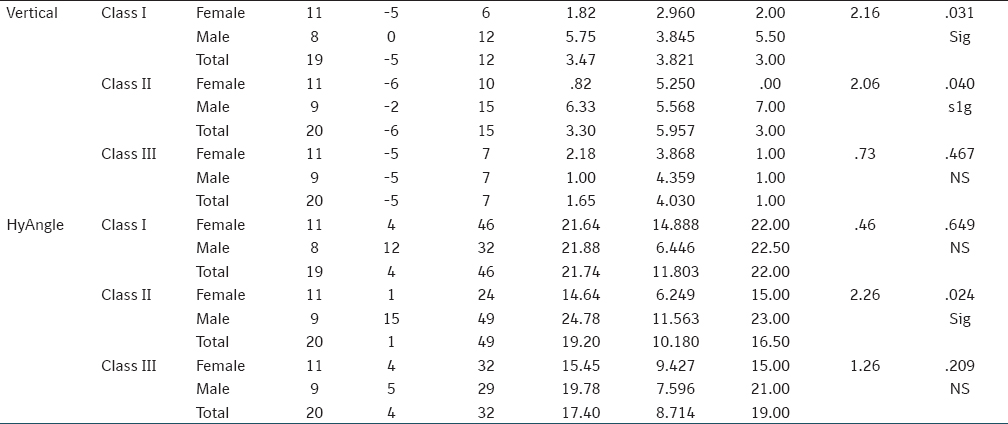
The Mann-Whitney test [Table 2] done to check for sexual dimorphism suggested that the hyoid bone is positioned at a lower level in class I and II in males than in females. Also, it was noted that the hyoid angle was significantly greater in males than in females in class II group. Nevertheless, no other significant differences were found in class I and II groups.
| Discussion | | |
The precise measurement of the hyoid bone position by cephalometric means is considered difficult. Previous investigators have found that the hyoid bone has a highly variable position not only from person to person, but also at different time intervals in the same person. [5],[6] Such variability in results could be attributed to the fact that most analysis has employed cranial structures to define the plane from which the hyoid bone position is measured and that a small variation in the position of the reference plane results in a much greater apparent variation of the hyoid bone irrespective of whether the hyoid bone changed or not. The present study attempts to minimize this effect by using the hyoid triangle analysis which employs planes between the mandibular symphysis and the vertebrae. The results of the hyoid triangle analysis are therefore more accurate compared with using other reference planes. [7]
Previous studies by Tsai [2] and Sheng et al. [4] concluded that the effects of gender on the hyoid bone position might begin during the period of adolescence due to the active growth of teenagers. In the present study also, only adult patients having permanent dentition were selected to avoid the effects of growth on the position of the hyoid bone.
It was seen that linear measurement from C 3 to the hyoid bone (C 3 -H) was significantly larger in males than in females in all the groups except the class II group. This was similar to results obtained by Kollias and Krogstad, [8] Adamidis and Spyropoulos [9] and Marsan. [10]
We did not note any significant differences in the linear distance between hyoid and the mandible (H-RGn) in any of the skeletal bases. This was in accordance with previously published results of Sahin Saglam and Uydas, [11] Muto and Kanazawa, [12] Taylor et al., [13] Marsan [10] and Haralabakis et al. [14]
The hyoid bone is positioned at a lower level in class I and II in males than in females which is in accordance with results obtained by Kollias and Krogstad [8] and longitudinal studies by Sheng et al. [4] Furthermore, it was noted that the hyoid angle was significantly greater in males than in females in class II group which was not reported in earlier studies.
Tsai [2] investigated the developmental changes of the hyoid bone position in children from deciduous dentition to early permanent dentition and concluded that there was no sexual dimorphism in hyoid bone position during that period. Bibby and Preston also concluded that there is no sexual dimorphism in the hyoid bone position, [1] however they too studied early adolescent patients having class I malocclusion only.
Adamidis and Spyropoulos [15] compared the hyoid bone position in class I to that in class III malocclusion and concluded that the latter patients, especially boys showed a different hyoid bone position and opinioned that the suprahyoid muscle might affect mandibular growth and that there may be different ways of regulating them between males and females.
Understanding the factors that affect the differential positioning of the hyoid bone in males and females would help in diagnosis, prediction and treatment of respiratory illness like obstructive sleep apnea where a definite male predilection is seen.
| Conclusion | | |
Sexual dimorphism was observed and the horizontal distance from the hyoid bone to the retrognathion was found to be significantly larger in males than in females. The hyoid bone is positioned at a lower level in class I and II in males than in females. Also, it was noted that the hyoid angle was significantly greater in males than in females in class II group.
| References | | |
| 1. | Bibby RE, Preston CB. The hyoid triangle. Am J Orthod 1981;80:92-7.  [ PUBMED] |
| 2. | Tsai HH. The positional changes of hyoid bone in children. J Clin Pediatr Dent 2002;27:29-34. |
| 3. | Miles PG, Vig PS, Weyant RJ, Forrest TD, Rockette HE Jr. Craniofacial structure and obstructive sleep apnea syndrome - a qualitative analysis and meta-analysis of the literature. Am J Orthod Dentofacial Orthop 1996;109:163-72. |
| 4. | Sheng CM, Lin LH, Su Y, Tsai HH. Developmental changes in pharyngeal airway depth and hyoid bone position from childhood to young adulthood. Angle Orthod 2009;79:484-90. |
| 5. | Brodie AG. Consideration of musculature in diagnosis, treatment and retention. Am J Orthod Dentofacial Orthop 1952;38:823. |
| 6. | Stepovich ML. A cephalometric positional study of the hyoid bone. Am J Orthod 1965;51:882-900. [ PUBMED] |
| 7. | Tsai HH, Ho CY, Lee PL, Tan CT. Cephalometric analysis of nonobese snorers either with or without obstructive sleep apnea syndrome. Angle Orthod 2007;77:1054-61. |
| 8. | Kollias I, Krogstad O. Adult craniocervical and pharyngeal changes - a longitudinal cephalometric study between 22 and 42 years of age. Part I: Morphological craniocervical and hyoid bone changes. Eur J Orthod 1999;21:333-44. |
| 9. | Adamidis IP, Spyropoulos MN. The effects of lymphadenoid hypertrophy on the position of the tongue, the mandible and the hyoid bone. Eur J Orthod 1983;5:287-94. [ PUBMED] |
| 10. | Marsan G. Head posture and hyoid bone position in adult Turkish Class III females and males. World J Orthod 2008;9:391-8. |
| 11. | Sahin Saglam AM, Uydas NE. Relationship between head posture and hyoid position in adult females and males. J Craniomaxillofac Surg 2006;34:85-92. |
| 12. | Muto T, Kanazawa M. Positional change of the hyoid bone at maximal mouth opening. Oral Surg Oral Med Oral Pathol 1994;77:451-5. |
| 13. | Taylor M, Hans MG, Strohl KP, Nelson S, Broadbent BH. Soft tissue growth of the oropharynx. Angle Orthod 1996;66:393-400. |
| 14. | Haralabakis NB, Toutountzakis NM, Yiagtzis SC. The hyoid bone position in adult individuals with open bite and normal occlusion. Eur J Orthod 1993;15:265-71. |
| 15. | Adamidis IP, Spyropoulos MN. Hyoid bone position and orientation in Class I and Class III malocclusions. Am J Orthod Dentofacial Orthop 1992;101:308-12. |
[Table 1], [Table 2]
|










 Search Pubmed for
Search Pubmed for