|
 
 |
| ORIGINAL ARTICLE |
|
| Year : 2015 | Volume
: 3
| Issue : 3 | Page : 170-174 |
|
Computed tomographic analysis of condyle-fossa relationship in skeletal class I and skeletal class II vertically growing males
Ankur Chaukse1, Sandhya Jain2, Rachna Dubey1, Rajkumar Maurya3, Chandresh Shukla4, Ashutosh Sthapak1
1 Department of Orthodontics, People's Dental Academy, Bhanpur, Bhopal, India
2 Department of Orthodontics, Government Dental College and Hospital, Indore, Madhya Pradesh, India
3 Department of Orthodontics, Corps Dental Unit, Bhanpur, Bhopal, India
4 Department of Orthodontics, People's College of Dental Science, Bhanpur, Bhopal, India
| Date of Web Publication | 11-Sep-2015 |
Correspondence Address:
Rajkumar Maurya
Department of Orthodontics, Corps Dental Unit, Bhopal - 462 001, Madhya Pradesh
India
 Source of Support: None, Conflict of Interest: None  | Check |
DOI: 10.4103/2321-3825.152120

Aim: The aim of the present study was to investigate the computed tomographic (CT) analysis of condyle-fossa relationship in skeletal Class I and Class II vertically growing males. Materials and Methods: The selected cases were divided into Group I: Control group, which comprised of 15 cases of skeletal Class I occlusion and Group II: Experimental group, which comprised of 15 cases of skeletal Class II malocclusion with cephalometric evaluation done to categorize the growth pattern. Occlusal state was evaluated on study models to exclude dentition with cross-bite, rotations, premature contacts, and absence of teeth. CT scan analyses were done to evaluate temporomandibular joint in both axial and coronal sections in centric occlusion. Results: Patients in Group II showed more angulated condyle, reduced posterior joint space, and decreased superior joint space with significant statistical difference (P < 0.05) in comparison to Group I. Group II also showed decreased glenoid-fossa width, less medial joint space, less condylar width anteroposteriorly but more mediolaterally in comparison to Group I, but it was statistically insignificant. Conclusion: Group II patient with retrognathic mandible showed more angulated condyle, which was positioned more posteriorly in the glenoid fossa with decreased superior joint space and constricted glenoid width in comparison with Group I patient. Keywords: Computed tomographic, glenoid-fossa, temperomandibular joint, temperomandibular joint spaces
How to cite this article:
Chaukse A, Jain S, Dubey R, Maurya R, Shukla C, Sthapak A. Computed tomographic analysis of condyle-fossa relationship in skeletal class I and skeletal class II vertically growing males. J Orthod Res 2015;3:170-4 |
How to cite this URL:
Chaukse A, Jain S, Dubey R, Maurya R, Shukla C, Sthapak A. Computed tomographic analysis of condyle-fossa relationship in skeletal class I and skeletal class II vertically growing males. J Orthod Res [serial online] 2015 [cited 2018 Sep 6];3:170-4. Available from: http://www.jorthodr.org/text.asp?2015/3/3/170/152120 |
| Introduction | |  |
The last few years have seen an increase in emphasis on the relationship of temporomandibular joint (TMJ) and malocclusion by orthodontists, as it plays an important role in planning orthodontic treatment. Occlusal disharmony is caused by various factors such as tipped and rotated molars, cross-bite, deep-bite, and various individual tooth malocclusions. All these factors play an important role in causing or aggravating TMJ dysfunction. The influence of occlusion on joint morphology is still not completely understood. Various studies showed a significant correlation between these variables. [1],[2],[3],[4],[5],[6] However, Cohlmia et al., [7] reported no relationship between them. The mandibular condyle is generally regarded as an active growth site, which responds to the functional forces. Most orthodontists agree that larger the discrepancy between the seated condyle and tooth intercuspation, the more difficult is to achieve the desired result posttreatment. [8] The significance of TMJ condyle-fossa relationship is still unclear. Many investigations have reported nonconcentric relationships in 50-89% of patients with TMJ disorders while other authors report no association of symptoms to posterior condyle position. [4] Anterior and posterior condylar positions have been associated with remodeling of the condyle and articular eminence with the predisposition for arthrosis.
According to Bednar, [9] visualization of the TMJ is often difficult because of its anatomy and the adjacent structures. Danforth et al., [10] stated that such difficulty might be eliminated by the use of computed tomographic (CT), which allows precise visualization of anatomic details. Thus, reliable data concerning morphology, irregularities, and condyle-fossa relationship can be obtained. CT scan bony window shows the condylar relation to the glenoid fossa in sections that can be measured to assess the joint and its various forms in relation to malocclusion. Hence, this study was conducted to assess the relationship of condylar fossa of the TMJ with the help of CT scan in subjects having Class I occlusion and in subjects having Class II malocclusion.
| Materials and Methods | | |
The present study was conducted in the Government Dental College and Hospital in coordination with Department of Radiology. Ethical Committee clearance (Government Dental College Ethical Committee Board, reference number GDC/Ortho/002/07) was obtained from the board before the commencement of the study. Cases were selected from the Outdoor Patients Department of Medical and Dental College. A total number of 100 patients were screened for the study, meeting with following criteria:
Inclusion criteria
- Age: 18-24 years was selected.
- Gender: Only males were selected.
- Class I occlusion and Class II malocclusion patients.
- Vertically growing patient to avoid any biasness in different growth pattern. Cephalometric analysis by Steiner's parameters, Y axis, gonial angle, and Wits appraisal was performed to select vertically growing patient.
Exclusion criteria
- Complete case history and clinical examination were conducted to exclude those with a history of TMJ disorders and pain.
- Occlusal state was evaluated on study models to exclude dentition with cross-bite, rotations, premature contacts, and absence of teeth.
Selected cases were divided into two groups:
Group I: Control group, those who are having skeletal Class I occlusion and meeting following cephalometric parameters:
- SNA 82 ± 2°
- SNB 80 ± 2°
- ANB 0-4°
- Wit's appraisal -1 mm
- Gonial angle >135°
- Mandibular plane angle >30°.
A total number of 15 subjects were selected for this group.
Group II: Experimental group, those who are having skeletal Class II malocclusion and fulfilling following cephalometric parameters:
- ANB >°.
- Wit's appraisal >2 mm.
- Gonial angle >135°.
- Mandibular plane angle >30°.
A total number of 15 subjects were also selected for this group.
Selected subjects and their guardians were informed about the study, and radiation exposure and informed consent were obtained from them.
All the above-selected cases were analyzed with the help of CT scan to assess and measure the TMJ. CT scan was conducted on light speed VCT machine at 140 kV and 220 mA in the Department of Radiology, CHL-Apollo Hospitals. Sections of 0.6 mm thickness CT scan slides were taken to evaluate TMJ in both axial and coronal sections in centric occlusion. Axial sections, which were parallel to the Frankfort horizontal plane as well as coronal sections which were parallel to N-Pog line were measured. Axial sections having maximum condyle width within the glenoid fossa were used for measurement. Coronal section showing maximum mediolateral width in the glenoid fossa was taken for measurement. All measurements were done directly on CT scan machine.
In axial section, following measurements were taken:
- Anterior space (space anterior to the condyle in the glenoid fossa) [Figure 1].
- Posterior space (space posterior to the condyle in the glenoid fossa) [Figure 1].
- Medial space (space medial to the condyle in the glenoid fossa) [Figure 1].
- Antero-posterior width of the glenoid fossa [Figure 1].
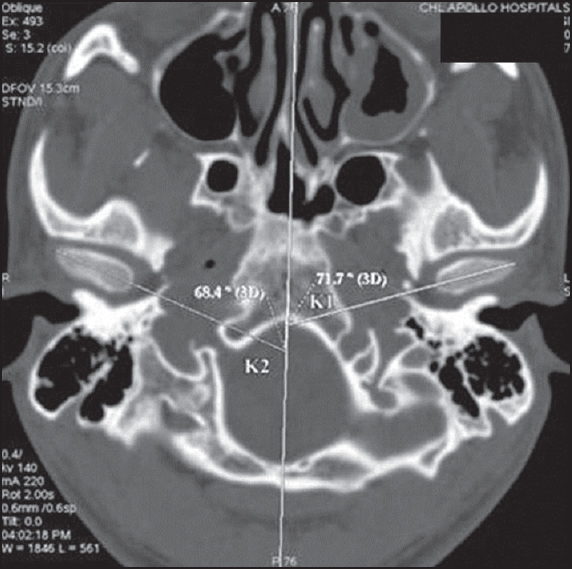
- Condylar angulation with the mid-sagittal plane [Figure 2].
- Mediolateral width of condyle [Figure 2].
- Antero-posterior width of condyle [Figure 2].
- Inter-condylar width (distance between the geometric center of condyles).
 | Figure 1: Computed tomographic scan of temporomandibular joint showing axial section
Click here to view |
 | Figure 2: Computed tomographic scan of temporomandibular joint showing coronal section
Click here to view |
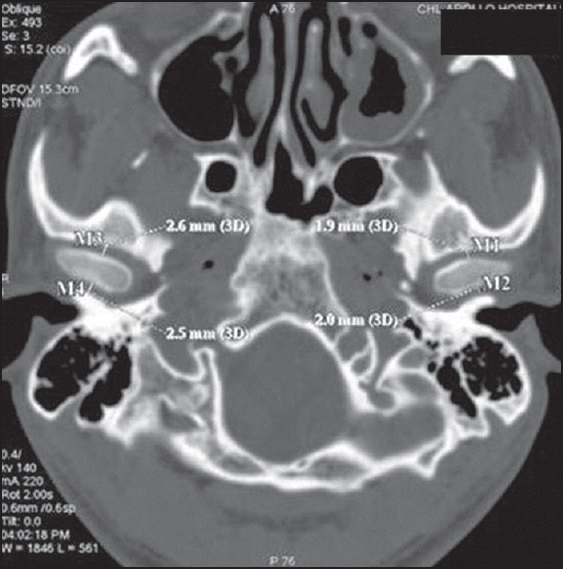
In coronal section, superior joint space or vertical depth (space superior to the condyle in the glenoid fossa) was measured [Figure 3].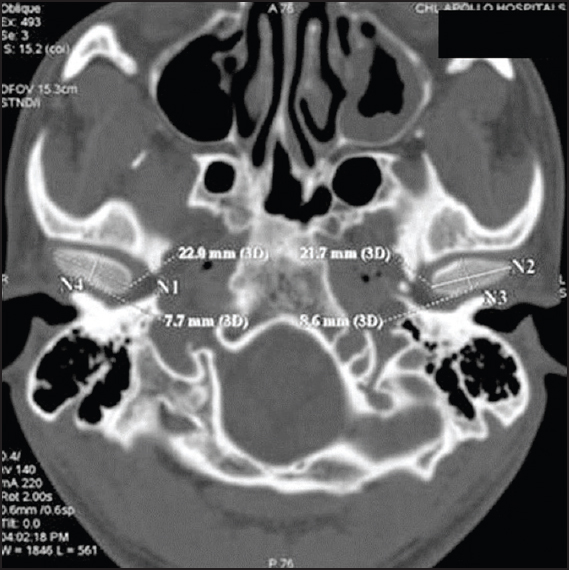 | Figure 3: Axial section showing medial and lateral space as M1 and M2 for right condyle and as M3 and M4 for left condyle
Click here to view |
Condylar position in glenoid-fossa was determined with the help of the formula as suggested by Pullinger et al: [4]
This formula represents condylar position as percent displacement from absolute concentricity, whereby a perfectly centered condyle would be expressed as 0%. A positive value indicates an anterior condylar positioning and a negative value would indicate posterior condylar positioning. Paired Student's t-test was applied. Different variables were compared between two groups by t-test to check the difference in two samples.
| Results | | |
The experimental group (Group II), which comprised of skeletal Class II malocclusion with retruded mandible showed more angulated condyle with reduced posterior joint space in comparison with the control group (Group I). The difference was statistically significant at P < 0.05 level [Table 1]. Group II also showed decreased superior joint space in the glenoid fossa in comparison with the Group I. The difference was statistically significant at P < 0.05 level [Table 1]. There was less medial joint space and decreased glenoid-fossa width in Group II in comparison to Group I, but the difference was not statistically significant at P < 0.05 level [Table 1]. Group II showed a less condylar width anteroposteriorly but more mediolaterally. The difference was statistically insignificant at P < 0.05 level [Table 1]. No significant difference was found in between the right and left side of TMJ in relation to condylar angulation, anterior space, posterior space, medial space, superior joint space, mediolateral condylar width, and glenoid fossa width in Group II and Group I subjects [Table 2] and [Table 3]. No significant difference in the intercondylar width [Table 1] was found.
| Discussion | | |
The relationship of malocclusion and TMJ disorders has since long affected orthodontic treatment. The significance of condylar position in the glenoid fossa in cases of TMJ disorders caused due to different malocclusions is a persistent controversy. This is mainly due to difficulties associated with visualization of TMJ radiographically. This may be a factor responsible for the discrepancies in the results of different studies related to this joint. Researchers have used various techniques to study the TMJ and its correlation with the malocclusion. All the above methods failed to give sufficient details of condylar position within the glenoid fossa to permit measurement of TMJ structures. However, even though their studies had limitations, they have paved a way for future progress in the research, for better and more accurate visualization of TMJ and its structures. The present study was carried out using CT scan, which was first introduced by Hounsfield in 1970's. [9]
Result of the study showed that there is a significant difference in condylar angulations, which showed reduced condylar angulations in the experimental group than in the control group showing altered condyle glenoid fossa relation. The angulations of the condyle were measured in relation to the mid-sagittal plane. According to Kurita et al., [11] pathological changes at the lateral part of the condyle might be responsible for TMJ pain and disc displacement. TMJ disc is firmly fixed at the lateral and medial aspects of the condyles. Change in the condylar angulations to the mid-sagittal plane in the experimental group moves the condyle more lateromedially resulting in altered lateral and medial pole position leading to altered disc attachment and its relation with the glenoid fossa. Significant difference was seen in the posterior space but no significant difference in anterior space was noted, suggesting of decreased posterior space or retruded condylar position in the glenoid fossa in the experimental group. Previous study on condyle-fossa relationship in different malocclusions and skeletal relationships was done by taking males and female subjects done by Cohlmia et al., [7] and found no significant differences in both skeletal cases. These discrepancies in results of different studies may be related to difficult visualization of TMJ with previous radiographic techniques.
Present study showed significant reduction of vertical depth or superior joint space in skeletal Class II cases showing a close approximation of the bony structures, therefore these cases are more prone in causing condyle and glenoid fossa erosions and degradation. Burke et al. [12] investigated a possible correlation between condylar characteristics and facial morphology in Class II adolescents. They used tomograms to measure joint spaces and found patients with vertical facial morphology had decreased superior joint spaces. As we have selected cases with vertical growth pattern only in this study, this might be the reason of nonsignificant decreased superior joint space in Group II. Results showed no significant difference in the condylar width in anteroposterior and mediolateral dimension but showed significant difference in glenoid width in the Group II in comparison with Group I; suggest decreased joint spaces again resulting in altered condyle-glenoid-fossa relation in the experimental group. This could lead to increased friction in the joint causing TMJ disorders. Posterior positioning of condyle and reduced glenoid width in experimental group vertical growers make them more prone for TMJ disorders. No significant difference was noted in intercondylar width in Group II in comparison with Group I. As this study showed marked variations in the condyle-glenoid-fossa relationship in the Group II, it can be assumed that these cases could be more prone to internal derangement, which may further lead to TMJ disorders. Pullinger et al. [13] in 1985, through his study concluded that malocclusion was associated with morphologic changes in the TMJ, particularly when correlated with age, sex, and longer exposure to malocclusion may be associated with more extensive TMJ changes. Earlier studies had shown that there was a significant difference in the measurements of males and females, to reduce this deviation and to get more standardized results; we have restricted our study to males only. This study showed that in group subjects on the right side, condyles were more angulated. This result corelates with the studies of Blaschke and Blaschke. [14] They concluded that there was a great variation in the condylar position in the glenoid fossa in centric occlusion in normal asymptomatic group also. Earlier, this type of correlation has not been studied; nonsignificant correlation in this study may be due to selection of mild to moderate malocclusions with vertical growth pattern only. Therefore, maximum times, TMJ disorders are associated with malocclusions. [15] In the future, if we try to correlate these variables in severe malocclusion groups and with different growth patterns, it might be possible that some significant correlation may be observed.
The present study revealed that the experimental Group II, which comprised of skeletal Class II malocclusion with retruded mandible showed more angulated condyle with reduced posterior joint space in comparison with the control Group I. The difference was statistically significant at P < 0.05 level [Table 1]. Group II also showed decreased superior joint space in glenoid fossa in comparison with the Group I. These results were also been supported by the study done by Arieta-Miranda et al. [16] and the results revealed that the anterior distance of the condyle to the articular eminence was statistically significant when comparing the Class I against the Class II (P = 0.033).
| Conclusion | | |
Based on the recorded data and statistical analysis, it can be concluded that:
- In skeletal Class II cases, condyle is more angulated and positioned more posteriorly in glenoid-fossa.
- There is decreased superior joint space and constricted glenoid width in comparison with skeletal Class II subjects.
| References | | |
| 1. | Myers DR, Barenie JT, Bell RA, Williamson EH. Condylar position in children with functional posterior crossbites: Before and after crossbite correction. Pediatr Dent 1980;2:190-4.  [ PUBMED] |
| 2. | Mongini F. Influence of function on temporomandibular joint remodeling and degenerative disease. Dent Clin North Am 1983;27:479-94. [ PUBMED] |
| 3. | Mongini F, Schmid W. Treatment of mandibular asymmetries during growth. A longitudinal study. Eur J Orthod 1987;9:51-67. [ PUBMED] |
| 4. | Pullinger AG, Solberg WK, Hollender L, Petersson A. Relationship of mandibular condylar position to dental occlusion factors in an asymptomatic population. Am J Orthod Dentofacial Orthop 1987;91:200-6. [ PUBMED] |
| 5. | O′Byrn BL, Sadowsky C, Schneider B, BeGole EA. An evaluation of mandibular asymmetry in adults with unilateral posterior crossbite. Am J Orthod Dentofacial Orthop 1995;107:394-400. |
| 6. | Schudy FF. Treatment of adult midline deviation by condylar repositioning. J Clin Orthod 1996;30:343-7. [ PUBMED] |
| 7. | Cohlmia JT, Ghosh J, Sinha PK, Nanda RS, Currier GF. Tomographic assessment of temporomandibular joints in patients with malocclusion. Angle Orthod 1996;66:27-35. |
| 8. | Girardot RA Jr. Comparison of condylar position in hyperdivergent and hypodivergent facial skeletal types. Angle Orthod 2001;71:240-6. |
| 9. | Bednar J. TMJ imaging. CDS Rev 1990;83:45-8. [ PUBMED] |
| 10. | Danforth RA, Otis LL, Kipnis V, Ong SH, Voss R. Corrected TMJ tomography: Effectiveness of alternatives to SMV tracing. Am J Orthod Dentofacial Orthop 1991;100:547-52. |
| 11. | Kurita H, Ohtsuka A, Kobayashi H, Kurashina K. A study of the relationship between the position of the condylar head and displacement of the temporomandibular joint disk. Dentomaxillofac Radiol 2001;30:162-5. |
| 12. | Burke G, Major P, Glover K, Prasad N. Correlations between condylar characteristics and facial morphology in Class II preadolescent patients. Am J Orthod Dentofacial Orthop 1998;114:328-36. |
| 13. | Pullinger AG, Hollender L, Solberg WK, Petersson A. A tomographic study of mandibular condyle position in an asymptomatic population. J Prosthet Dent 1985;53:706-13. [ PUBMED] |
| 14. | Blaschke DD, Blaschke TJ. Normal TMJ bony relationships in centric occlusion. J Dent Res 1981;60:98-104. [ PUBMED] |
| 15. | Gupta OP, Forrest EJ, Sassouni V, Mundell RD. Studies on experimental malocclusion in rabbis. 1. Method of induction of malocclusion and its effects on the temporomandibular joint. Am J Orthod Dentofacial Orthop 1971;60:54-67. |
| 16. | Arieta-Miranda JM, Silva-Valencia M, Flores-Mir C, Paredes-Sampen NA, Arriola-Guillen LE. Spatial analysis of condyle position according to sagittal skeletal relationship, assessed by cone beam computed tomography. Prog Orthod 2013;14:36. |
[Figure 1], [Figure 2], [Figure 3]
[Table 1], [Table 2], [Table 3]
|










 Search Pubmed for
Search Pubmed for