|


 |
| HOW DO I DO IT? |
|
| Year : 2011 | Volume
: 3
| Issue : 2 | Page : 106-109 |
|
|
Laparoscopic right radical nephrectomy
Sadhana V Deo1, Dhananjay S Kelkar2
1 Associate Professor in General Surgery, B. J. Medical College, Pune, India
2 Medical Director, Deenanath Mangeshkar Hospital, Pune, India
| Date of Web Publication | 11-Feb-2012 |
Correspondence Address:
Sadhana V Deo
43/67, Navsahyadri Society, Akshay, Pune - 411 052
India
 Source of Support: None, Conflict of Interest: None
DOI: 10.4103/2006-8808.92806

 Abstract Abstract | | |
Laparoscopic radical nephrectomy is a minimally invasive surgical procedure and is in practice since 1992 in USA. We describe the novel technique of this procedure with an added advantage. Controlling renal vessels first at the hilum with lymphadenectomy is our principle of surgery. This technique is known as transperitoneal medial to lateral approach radical nephrectomy. Keywords: Gerota′s fascia, laparoscopic, radical nephrectomy, renal cell carcinoma, renal hilum
How to cite this article:
Deo SV, Kelkar DS. Laparoscopic right radical nephrectomy. J Surg Tech Case Report 2011;3:106-9 |
| Introduction | |  |
Renal cell carcinoma is the most common malignancy of kidney accounting for 3% of adult malignancies. [1] More sensitive imaging techniques including USG and CT scan with contrast have helped in the early and incidental detection of renal cancer. Laparoscopic radical nephrectomy has become the preferred method for renal cancer due to the radical removal of tumor with all added advantages of laparoscopic surgery like less pain, rapid convalescence, and improved cosmesis. [1],[2],[3]
| Preoperative Evaluation | | |
The patient is evaluated with USG and CT scan with contrast to know the exact site, size of renal cell carcinoma, its extension beyond Gerota's fascia, liver secondaries, IVC involvement, and hilar lymphadenopthy. A routine blood check-up including liver function tests and renal function tests is mandatory to assess the contralateral renal function and fitness. X ray or CT of the chest is required for the assessment of pulmonary metastasis. A bone scan is obtained in patients with elevated serum calcium or alkaline phosphatase levels and in those with symptomatic bone pain. If there is a question of renal vein tumor thrombus, then an appropriate study (MRI, sonography, or three-dimensional CT) is done preoperatively to evaluate the vein.
| Positioning and Ports | | |
The patient is kept Nil by mouth for 8 hours. Ryle's tube is placed and the bladder is catheterized under general anesthesia.
Preoperative injectable antibiotics, i.e., Taxim and Amikacin are given.
In the OT, the patient is placed in right kidney position at an angle of 45°. Behind the back of the patient, a 1-L saline bottle is kept for support. The patient is kept in a secure position with multiple, broad adhesive strips. The upper leg is extended while the lower leg is flexed with a pillow between the legs. Two arms are kept comfortably with padding. The operating surgeon and camera person are on the left side of the patient and the monitor is kept on the right side of the patient at the level of eyes of the surgeons.
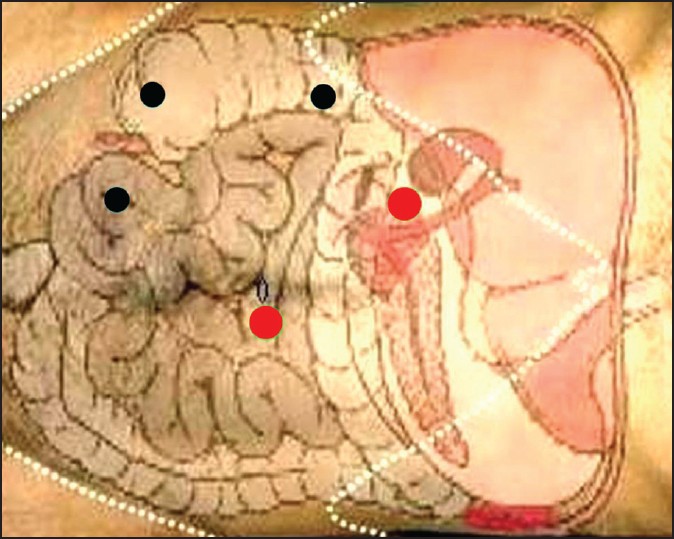
Pneumoperitoneum is done with a Veress needle through the umbilicus. Following ports are inserted [Figure 1]:
- 10-mm umbilical, camera port for the 0° telescope
- 10-mm right hand working port in the epigastrium pararectally
- 5-mm left hand working port in the hypogastric region pararectally
- One or two 5-mm ports are placed as per requirement for bowel and liver retraction.
| Operative Steps | | |
Laparoscopic radical nephrectomy is done medial to lateral through a transperitoneal approach. The following steps are taken:
- Reflection of the colon.
- Along the white line of Toldt, the right colon is reflected medially across the midline to provide an adequate visualization of the anterior surface of Gerota's fascia. The duodenum is kocherised until the IVC is clearly visualized.
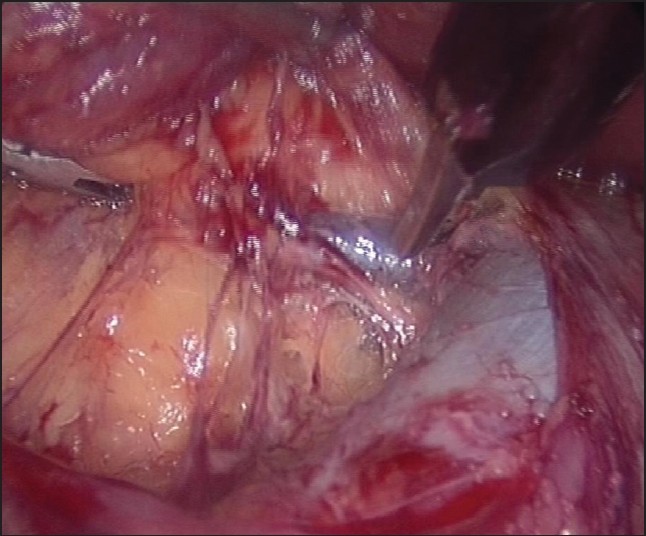
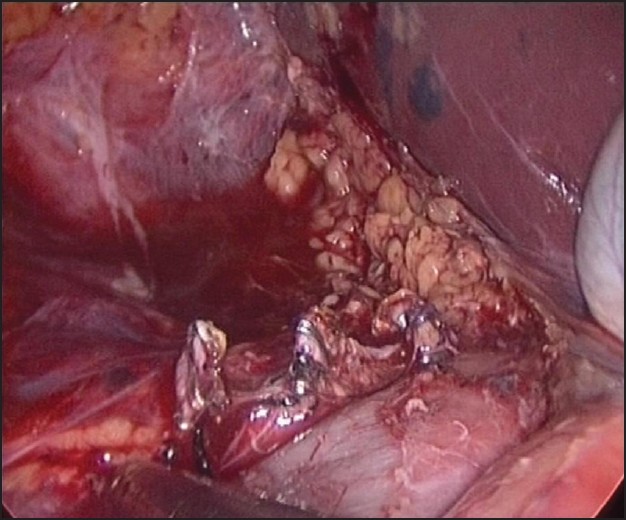
- Securing the renal blood vessels: The retraction of the liver to improve the visualization of the renal hilum is done by atraumatic grasper placed through an extra 5-mm trocar below the ribs in the anterior axillary line. The dissection of the right renal vein in relation to IVC is done by using the Harmonic Ace (Ethicon Endo-Surgery, Cincinnati, OH, USA) in transperitoneal approach [Figure 2].
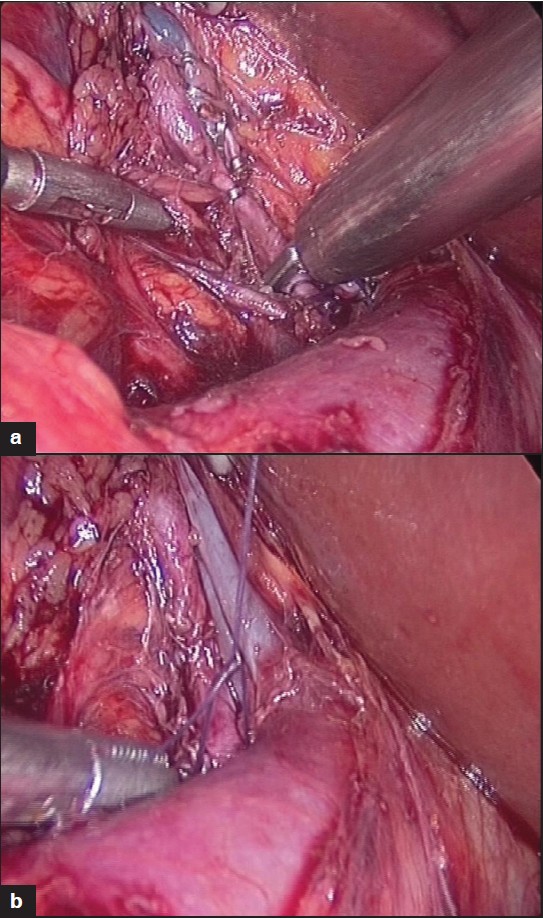 | Figure 2: (a) Clipping of renal vein tributary, (b) Clipping of all right renal veins
Click here to view |
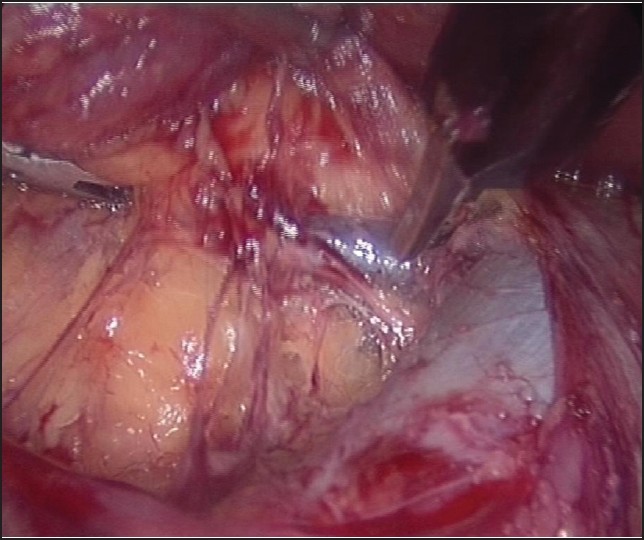
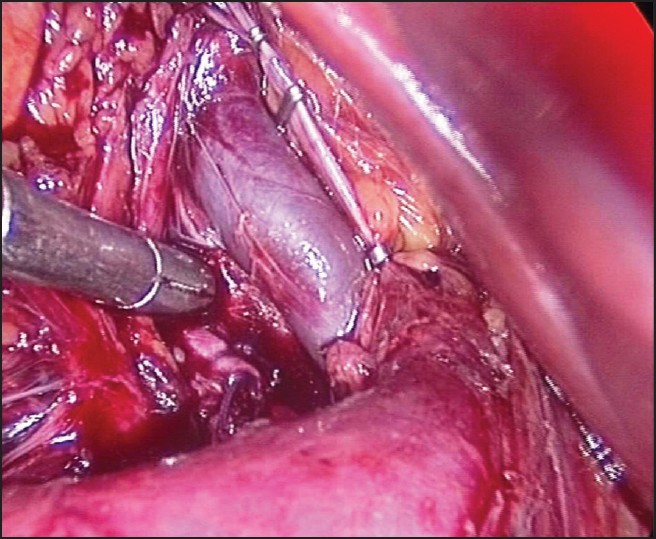
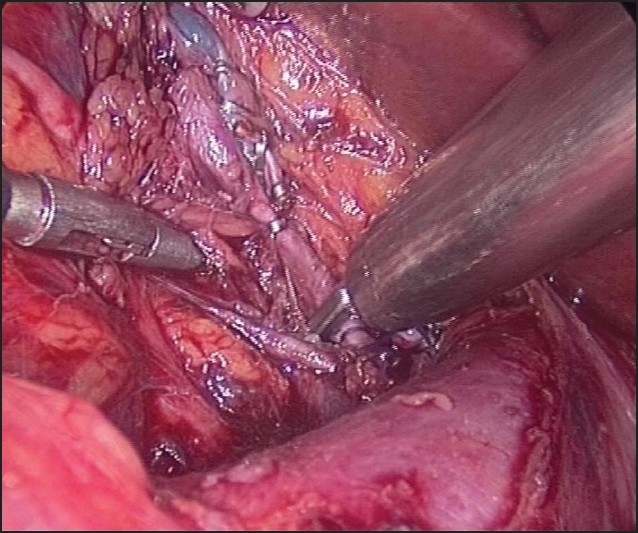
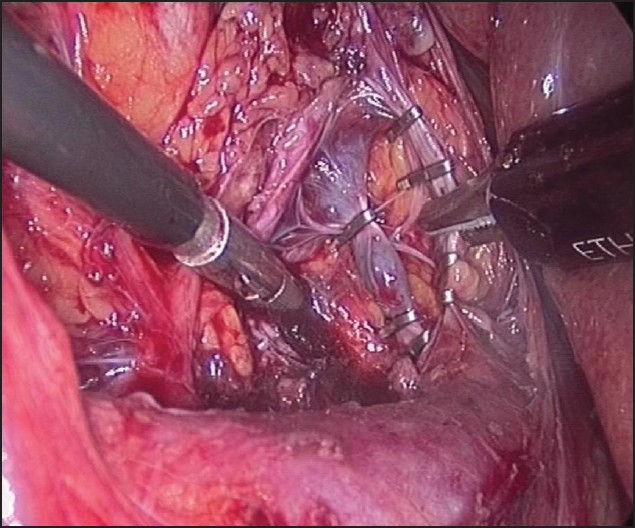
- The right renal vein is dissected circumferentially with the Mixter forceps. The right renal artery which lies inferior and posterior to the right renal vein is dissected and clipped with two hemoclips proximally and with two distally. The tributaries of the renal vein are clipped with titanium clips doubly and divided [Figure 3],[Figure 4],[Figure 5] and [Figure 6].
- The renal artery is divided first with Harmonic Ace to prevent congestion of the kidney. [1],[2],[3] The first lumbar vein and adrenal vein are clipped and divided. All fibro fatty tissues with lymph nodes around the renal hilum are dissected upward toward the specimen.
- The kidney is mobilized with Gerota's fascia from surrounding structures. The separation of the kidney from the lateral abdominal wall is done at last so that the specimen does not fall on the operative field.
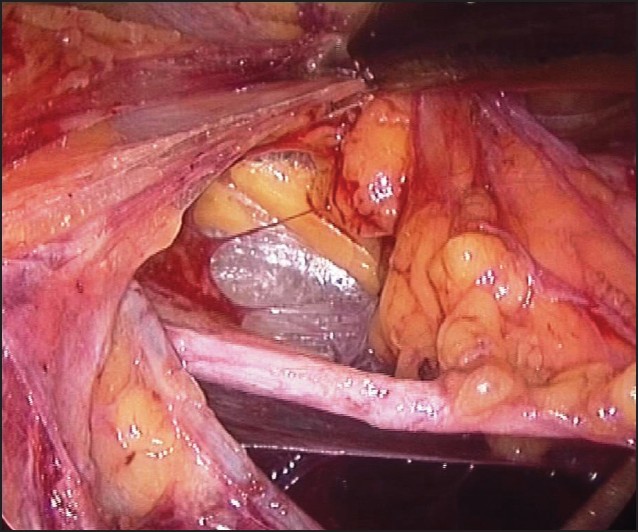
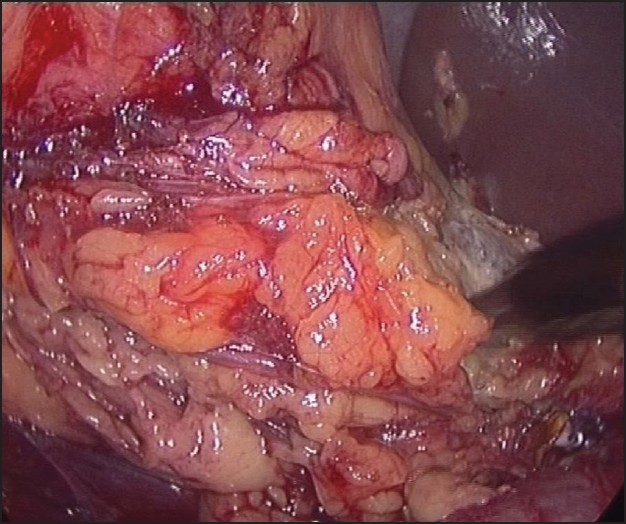
- Dissection of the ureter: The psoas tendon is a reliable landmark when searching for the gonadal vein and ureter. Once located, the ureter is elevated from the psoas muscle, clipped, and cut. The gonadal vein may be visualized at an early stage during the dissection of Gerota's fascia if the bowel is properly retracted medially [Figure 7],[Figure 8],[Figure 9],[Figure 10] and [Figure 11].
- The hemostasis is checked with the irrigation of a warm ringer lactate solution and also by reducing CO 2 pressure to reduce the tamponade effect on bleeding veins. Number 32 French drain is kept at the renal hilum.
- The specimen is kept in an endobag to prevent port site metastasis and delivered through a small muscle-splitting incision in the right iliac fossa [2],[3] or through an incision between two trocars.
- All port sites are irrigated with betadine and closed with Vicryl and Ethilon sutures.
| Postoperative Care | | |
Ryle's tube is removed at the conclusion of the procedure. Postoperatively, the patient is monitored hemo dynamically, and for urine and drain output. The patient is given liquids after 12 h. The Foley's catheter should be removed once the patient is comfortably ambulating. The patient is discharged when tolerating a regular diet. An unrestricted activity can usually be resumed according to the patient's comfort. As specimen is removed through an incision, lifting is limited to 6 weeks.
| Conclusion | | |
Laparoscopic radical nephrectomy has established its role as a standard of care for the management of renal neoplasms. [4] Long-term follow-up has demonstrated that laparoscopic radical nephrectomy has shorter patient hospitalization time and effective cancer control with no significant difference in the survival compared with open radical nephrectomy. [5],[6],[7],[8] After comparing open versus laparoscopic radical nephrectomy, the complication rates found are 10% and 12%, respectively. Thus, laparoscopic radical nephrectomy is better than open in overall survival without recurrence and early recovery. [8],[9],[10]
| References | | |
| 1. | Chan DY, Cadeddu JA, Jarrett TW, Marshall FF, Kavoussi LR. Laparoscopic radical nephrectomy: Cancer control in renal carcinoma. J Urol 2001;166:2095. 
|
| 2. | Cadeddu JA, Ono Y, ClaymanRV, Barrett PH, Janetschek G, Fentie DD, et al. Laparoscopic nephrectomy for renal cell cancer: Evaluation of efficacy and safety: A multi-center experience. Urology 1998;52:773-7.
|
| 3. | Jeschke K, Wakoing J, Pitzler C, Henning K. Laparoscopic radical nephrectomy: A single center experience of 51 cases. Tech Urol 2000;6:9-11.
|
| 4. | Ono Y, Kinukawa T, Hattori R, YamadaS, Nishiyama N, Mizutani K, et al. Laparoscopic radical nephrectomy for renal cell carcinoma: A five-year experience. Urology 1999;53:280-6.
|
| 5. | Dunn MD, Portis AJ, Shalhav AL, Elbahnasy AM, Heidorn C, McDougall EM, et al. Laparoscopic versus open radical nephrectomy: A 9-year experience. J Urol 2000;164:1153-9.
[PUBMED] |
| 6. | McDougall EM, Clayman CR, Elashry OM. Laparoscopic radical nephrectomy for renal tumor: The Washington University Hospital experience. J Urol 1996;155:1180-5.
|
| 7. | Ono Y, Hattori R, Gotoh M, Yoshino Y, Yoshikawa Y, Kamihira O. Laparoscopic radical nephrectomy for renal cell carcinoma: The standard of care already? CurrOpinUrol 2005;15:75-8.
|
| 8. | Portis AJ, Yan Y, Landman J, Chen C, Barrett PH, Fentie DD, et al. Long-term follow-up after laparoscopic radical nephrectomy. J Urol 2002;167:1257-62
|
| 9. | Lee BR. Laparoscopic total and partial nephrectomy-the new standard? Rev Urol 2003;5:9-14.
[PUBMED] [FULLTEXT] |
| 10. | Golimbu M, Joshi P, Sperker A, Tessler A, Al-Askari S, Morales P. Renal cell carcinoma: Survival and prognostic factors. Urology 1986;27:291-301.
|
[Figure 1], [Figure 2], [Figure 3], [Figure 4], [Figure 5], [Figure 6], [Figure 7], [Figure 8], [Figure 9], [Figure 10], [Figure 11]
|