|


 |
| CASE REPORT |
|
| Year : 2011 | Volume
: 3
| Issue : 2 | Page : 102-105 |
|
|
Ankle arthrodesis following trauma, a useful salvage procedure - A report on three cases
Muhammad Oboirien
Department of Orthopaedics and Trauma, Trauma Centre, Usmanu Danfodiyo University Teaching Hospital, Sokoto, Nigeria
| Date of Web Publication | 11-Feb-2012 |
Correspondence Address:
Muhammad Oboirien
Department of Orthopaedics and Trauma, Trauma Centre, Usmanu Danfodiyo University Teaching Hospital, PMB 2370, Sokoto
Nigeria
 Source of Support: None, Conflict of Interest: None  | 2 |
DOI: 10.4103/2006-8808.92805

 Abstract Abstract | | |
Open musculoskeletal injuries remain a difficult problem to manage especially in resource-poor regions. They are complicated by prolonged morbidity and chronic osseous infections and sometimes gangrene. Our objective was to look at ankle arthrodesis as a primary and useful salvage procedure through simple technique for cases of severe open ankle injuries. Three patients with severe open ankle injuries between January 2007 and December 2009 were seen and had wound debridement done and compressive ankle arthrodesis with a Charnley's arthrodesis clamp. Tibiotalar and tibiocalcaneal arthrodesis was the procedure carried out. Patients were followed up for 3-12 months. Wound breakdown was seen in two cases and one later had skin grafting. All patients expressed satisfaction with the outcome of surgery. Ankle arthrodesis is a simple and useful salvage procedure for severe ankle disruption, guaranteeing patients satisfaction as against amputation. Keywords: Arthrodesis, severe open ankle injury, salvage
How to cite this article:
Oboirien M. Ankle arthrodesis following trauma, a useful salvage procedure - A report on three cases. J Surg Tech Case Report 2011;3:102-5 |
How to cite this URL:
Oboirien M. Ankle arthrodesis following trauma, a useful salvage procedure - A report on three cases. J Surg Tech Case Report [serial online] 2011 [cited 2016 Jun 12];3:102-5. Available from: http://www.jstcr.org/text.asp?2011/3/2/102/92805 |
| Introduction | |  |
Ankle arthrodesis is the surgical fusion of the ankle joint which aims to relieve pain, and restores function. Ankle arthrodesis, used as surgical treatment for tuberculosis of the ankle joint, is still used for the treatment of ankle joint destruction. Arthrodesis of the ankle joint is an important operation in the treatment of painful arthrosis, chronic infection, and malalignment, and instability. [1] It is commonly indicated in post-traumatic painful osteoarthritis and severe ankle injury. [2] Following severe trauma, the ankle mortise is disrupted, and also the tibiotalar articular cartilage with resulting inflammation, synovitis, osteophyte formation, progressive loss of ankle-joint motion, weight-bearing pain, and functional disability. [2],[3],[4] Ankle reconstruction is a viable option if a precise restoration of the ankle-joint anatomic relationship can be done. The anatomic reconstruction of a malunited ankle joint will prevent further progression of ankle arthritis, even in the presence of early disease. [5] In one series, good to excellent results were achieved in 85% of patients after the reconstruction of ankle malunions. [6] Ankle reconstruction procedures in cases of open injuries are time consuming, unsatisfactory, and complicated by infection especially when implants are used. Patients with severe ankle injuries who had reconstruction do have post-traumatic osteoarthritis as cartilage disintegration is irreversible. We therefore consider primary ankle fusion for open injuries as an alternative to reconstruction.
| Case Reports | | |
Case 1
We present the case of a 23-year-old male, commercial motorcyclist who was hit by a fast moving vehicle while negotiating a bend. He fell and sustained open injury to the right ankle with deformity. He bled moderately from the wound but there was no loss of consciousness or bleeding from the craniofacial orifices. There was no injury in any other part of the body. There was no history of alcohol use nor was there any premorbid condition. He was in painful distress and was unable to bear weight on the affected right lower limb. The patient had an injury severity score (ISS) of 16. Significant findings were in the right lower limb which showed that the right ankle was deformed with an avulsion wound on the medial malleolus and a 5-cm-deep laceration on the lateral malleolus [Figure 1]. The dorsalis pedis artery was palpable, so was the posterior tibial artery; the sensation was intact but the patient could move the toes. A radiograph of the right ankle showed a fracture dislocation with severe disruption of the ankle mortise [Figure 2]. A diagnosis of the Gustilllo-Anderson type 3b fracture dislocation of the right ankle was made. He was resuscitated and had tetanus toxoid with antibiotic prophylaxis. The wound was irrigated with 2 l of normal saline, and the patient had initial reduction and splintage of the ankle injury. He had a tibiotalar arthrodesis 48 h after presentation. Wound infection was noted 5 days postoperatively and was managed with daily wound dressings. Wound healed by secondary intention; the patient was discharged after 4 weeks and was followed up for 5 months. The external fixator was removed and replaced with a cast booth at 8 weeks. A radiologic union was noted by 12 weeks postoperatively. The patient started full weight bearing at 16 weeks.  | Figure 2: Radiograph of the right ankle with severe disruption of the ankle mortise
Click here to view |
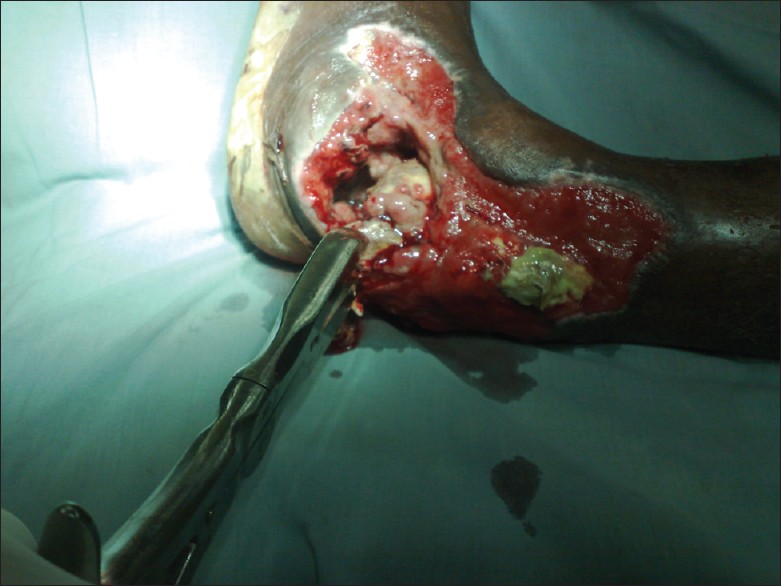
Case 2
This was a case of a 35-year-old businessman who was a middle seat passenger in an 18-seater commercial vehicle which crashed off the road following a tyre burst. The vehicle reportedly somersaulted and there were three fatalities. He sustained an open injury in the left ankle and there was transient loss of consciousness. He was first seen at the peripheral hospital where he was resuscitated; he later regained consciousness after 3 h. The patient however opted to see a traditional bonesetter. He presented 10 days later with an infected open ankle injury. He was not a known diabetic nor was he known to be on any steroid medication. He was pale but not in any distress. The left ankle showed an infected open wound with soft tissue loss and a defective Achilles tendon [Figure 3]. He was worked up for surgery and had a tibiotalar arthrodesis after debridement. Wound infection persisted postoperatively and was managed with wound dressings and later skin grafting after a sufficiently healthy granulation tissue was noted. The patient was followed up for 3 months during which the external fixator was removed and replaced with a cast.
Case 3
This is a case of a 30-year-old male student who was involved in a vehicular accident. He was a back seat passenger in a saloon car which had a head-to-side collision with a truck. There was no fatality and the patient did not lose consciousness nor was there bleeding from any of the craniofacial orifices. He sustained an open injury to the right ankle with no other injuries. He was seen at the emergency room 4 h after the accident. He was in painful distress with an ISS of 16. Significant findings were in the right lower limb which showed a deformed ankle and an 8-cm-deep laceration on the posterior aspect showing a talus loss. He was resuscitated and had a tibiocalcaneal arthrodesis 24 h after the presentation. The patient did well postoperatively and was followed up for 12 months. Varus angulation was noted during the initial stage of partial weight bearing and this was corrected with the application of a plaster of Paris cast. A radiologic union was noted at 20 weeks and the patient commenced full weight bearing with a limb length discrepancy of 2 cm.
Surgical technique
Several techniques are available for performing the procedure, the most successful being an open approach with compression and internal fixation. The selection of the surgical technique should be based on the underlying disorder. As a general rule, external fixators are preferred for patients undergoing arthrodesis for a pre-existing septic joint and for those with severe open injuries. The Charnley method which we used combined open surgical debridement of the ankle-joint cartilage with the application of an external fixator by placing one pin through the tibia and another through the calcaneus, with connecting bars running between the two pins. Compression across the arthrodesis site relies on an intact Achilles tendon functioning as a tension band. Patients were allowed to bear weight on the treated ankle during the first 8 weeks after surgery. After the removal of the external fixator, patients were immobilized in a plaster walking cast for an additional 4 weeks.
In our patients, access was gained to the joint through wound extension making sure to preserve the dorsalis pedis artery. Its benefits are better visualization of the joint and improved access for bone resection. Extensive wound debridement was done and the articular cartilage in the tibia and talus was removed through transverse cuts to expose the subchondral bones. After the removal of the distal tibial articular surface, the talus was positioned so that the forefoot was in 5-10° of external rotation and the hind foot was in 5° of valgus, with neutral dorsiflexion and displacement so that the posterior margins of the talus and tibia were flush. The foot must be aligned with regard to the entire limb and it must be ensured that it is plantigrade. A cut through the dome of the talus was then made parallel to the distal tibia, resecting approximately 5 mm of the talus. The arthrodesis clamp is then assembled after passing distal transtibial and transcalcaneal Steinmann's pins [Figure 4].
The soft tissue defects were managed with split thickness skin grafting after sufficient healthy granulation tissues were formed in a later operation.
| Discussion | | |
Ankle arthrodesis is the procedure of choice for debilitating osteoarthritis of the ankle. It is however not a common operation in our subregion as cases of post-traumatic arthrosis of the ankle are commonly managed with nonsteroidal anti-inflammatory drugs and few see the need for surgery especially when minimally invasive procedures are still lacking. Fifty-eight patients underwent ankle arthrodesis in Lagos over a 15-year period with an average of 3.9 patients per year and the common indications were post-traumatic arthrosis followed by severe acute ankle injuries. [2] Various techniques are available for ankle arthrodesis. [7],[8],[9] The selection of the surgical technique should be based on the underlying disorder. As a general rule, external fixators are preferred for patients undergoing arthrodesis for a pre-existing septic joint and for those with severe osteopenia. Arthroscopic arthrodesis or the "mini-open" arthrodesis should be used only for patients with minimal deformity. Open arthrodesis is appropriate for patients with a significant ankle deformity from severe injury and foot and ankle malalignment. [3],[9],[10] Our patients had their surgeries between 1 and 14 days after the injury with a high potential for infection; hence, the choice of wound debridement and compressive arthrodesis using a Charnley's clamp was made. [11] This procedure is safe and easy as access is readily gained into the joint through the wound. Wound infection and nonunion are common complications of this procedure. Two of our patients had wound breakdown and one had skin grafting and one healed by secondary intention. Antibiotic use played a part in the early remission of the wound infection.
| References | | |
| 1. | Bauer G, Kinzl L. Arthrodesis of the ankle joint. Orthopade 1996;25:158-65. 
[PUBMED] |
| 2. | Yinusa W, Adegbite O, Owoola A. Arthrodesis of the ankle- 5 year review. Niger Postgrad Med J 2009;16:64-7.
[PUBMED] |
| 3. | Abidi NA, Gruen GS, Conti SF. Ankle arthrodesis: Indications and techniques. J Am Acad Orthop Surg 2000;8:200-9.
[PUBMED] [FULLTEXT] |
| 4. | Richter D, Hahn MP, Laun RA, Ekkernkamp A, Muhr G, Ostermann PA. Arthrodesis of the infected ankle and subtalar joint: Technique, indications, and results of 45 consecutive cases. J Trauma 1999;47:1072-8.
[PUBMED] [FULLTEXT] |
| 5. | Marti RK, Raaymakers EL, Nolte PA. Malunited ankle fractures: The late results of reconstruction. J Bone Joint Surg Br 1990;72:709-13.
[PUBMED] [FULLTEXT] |
| 6. | Rosen H. Reconstructive procedures about the ankle joint. In: Jahss MH, editor. Disorders of the Foot and Ankle: Medical and Surgical Management, 2nd ed. Philadelphia: WB Saunders; 1991. p. 2593-613.
|
| 7. | Clare MP, Sanders RW. The anatomic compression arthrodesis technique with anterior plate augmentation for ankle arthrodesis. Foot Ankle Clin 2011;16:91-101.
[PUBMED] [FULLTEXT] |
| 8. | Shah KS, Younger AS. Primary tibiotalocalcaneal arthrodesis. Foot Ankle Clin 2011;16:115-36.
[PUBMED] [FULLTEXT] |
| 9. | Thermann H, Hüfner T, Roehler A, Tscherne H. Screw arthrodesis of the ankle joint. Technique and outcome. Orthopade 1996;25:166-76.
|
| 10. | Labitzke R. Ankle arthrodesis using the cable technique. Oper Orthop Traumatol 2005;17:392-406.
[PUBMED] |
| 11. | Charnley J. Compression arthrodesis of the ankle and shoulder. J Bone Joint Surg Br 1951;33B:180-91.
[PUBMED] |
[Figure 1], [Figure 2], [Figure 3], [Figure 4]
| This article has been cited by | | 1 |
Tibiocalcaneal arthrodesis using an Ilizarov fixator |
|
| Leite, A.M. and Menezes, H.M. and Castro Aquino, I.E. and Martins, J.S. and De Moraes, F.B. | | Revista Brasileira de Ortopedia. 2013; 48(1): 57-61 | | [Pubmed] | | | 2 |
Tibiocalcaneal arthrodesis using an Ilizarov fixator |
|
| Alessandro Marcondes Leite,Helder Mattos Menezes,Igor e Castro Aquino,Jefferson Soares Martins,Frederico Barra de Moraes | | Revista Brasileira de Ortopedia (English Edition). 2013; 48(1): 57 | | [Pubmed] | [DOI] | | | 3 |
Artrodese tibiocalcaneana usando fixador de Ilizarov |
|
| Alessandro Marcondes Leite,Helder Mattos Menezes,Igor e Castro Aquino,Jefferson Soares Martins,Frederico Barra de Moraes | | Revista Brasileira de Ortopedia. 2013; 48(1): 57 | | [Pubmed] | [DOI] | |
|




 |
|
|
|