|


 |
| ORIGINAL ARTICLE |
|
| Year : 2011 | Volume
: 3
| Issue : 2 | Page : 84-86 |
|
|
Two-port laparoscopic-assisted appendicectomy under local anesthesia in adults: A pilot study
Saswata Bharati1, Dinesh K Singh1, Vijay K Shukla2
1 Department of Anesthesiology, Institute of Medical Sciences, Banaras Hindu University, Varanasi, Uttar Pradesh, India
2 Department of General Surgery, Institute of Medical Sciences, Banaras Hindu University, Varanasi, Uttar Pradesh, India
| Date of Web Publication | 11-Feb-2012 |
Correspondence Address:
Vijay K Shukla
Department of General Surgery, Institute of Medical Sciences, Banaras Hindu University, Varanasi - 221 005
India
 Source of Support: None, Conflict of Interest: None
DOI: 10.4103/2006-8808.92799

 Abstract Abstract | | |
Aim : Nowadays laparoscopic-assisted appendicectomy using the two-port technique is gaining popularity due to its certain benefits over the open version. General anesthesia with positive pressure ventilation is the preferred mode of anesthesia in this technique. We conducted a pilot study using the two-port technique in adult patients, with uncomplicated appendicitis under local anesthesia, to evaluate its feasibility. Materials and Methods: In this prospective study 12 consecutive patients of ASA grade I and II, with a mean age of 22.5 years, suffering from acute appendicitis, were included. All the patients received ondansetron, diazepam, and pentazocine as premedication. Monitored anesthesia care was given. The site of trocar insertions were infiltrated with 1% lignocaine with adrenalin. The pneumoperitoneum was created using carbon-di-oxide. After exteriorization of the appendix using the trocar, appendicectomy was performed as in the open procedure. Results : Eleven out of twelve patients were successfully operated using this method without converting it into an open method. Two cases required an extra port to free the appendix from the adhesion. There were no intra- or post-operative complications present. Conclusion: Two-port laparoscopic-assisted appendicectomy under local anesthesia is a safe and effective method for uncomplicated appendicitis in adults, and the procedure is suitable where limited set-up for anesthesia is present. Keywords: Laparoscopic appendicectomy, laparoscopic-assisted appendicectomy, local anesthesia, monitored anesthesia care
How to cite this article:
Bharati S, Singh DK, Shukla VK. Two-port laparoscopic-assisted appendicectomy under local anesthesia in adults: A pilot study. J Surg Tech Case Report 2011;3:84-6 |
How to cite this URL:
Bharati S, Singh DK, Shukla VK. Two-port laparoscopic-assisted appendicectomy under local anesthesia in adults: A pilot study. J Surg Tech Case Report [serial online] 2011 [cited 2016 Jun 12];3:84-6. Available from: http://www.jstcr.org/text.asp?2011/3/2/84/92799 |
| Introduction | |  |
Appendicectomy is the most commonly performed intra-abdominal operation. Semm [1] first introduced the laparoscopic method for appendicectomy in the early 1980s. Since then laparoscopic appendicectomy (LA) was made popular by various surgeons and preferred over the open method due to its inherent advantages. [2] However, this technically demanding procedure requires increased surgical time and general anesthesia with positive pressure ventilation. Also, this is an expensive procedure and requires an advanced surgical set-up and skilled surgeons, which prevent its use as routine practice in developing countries. The laparoscopic-assisted appendicectomy (LAA) technique has all the advantages of the laparoscopic method at less expense than the completely laparoscopic technique, with a shorter operating time as an added advantage. The aim of our study is to evaluate the feasibility of laparoscopic-assisted appendicectomy (LAA) using the two-port technique under local anesthesia in adults. As a pilot study we included a selected group of patients with low body mass index (BMI) and uncomplicated appendicitis.
| Materials and Methods | | |
We conducted a prospective study over a two-month period where LAA was performed on 12 patients (seven female and five male) of ASA grade I or II, who presented with acute appendicitis. Inclusion criteria included - pain in the right iliac fossa, with muscle guarding, tenderness at McBurney's point, vomiting, fever, leukocytosis, and age more than 18 years. All the patients had a plain abdominal radiograph, routine blood tests, and a sonographic examination. Patients with generalized peritonitis, appendicular abscess or perforation, and a palpable mass were excluded from the study. The patients who were found to have gangrenous or perforated appendicitis under laparoscopic view were excluded from this study and converted into the open technique. All the patients were explained about the procedure and the possible conversion into open technique and written consent was taken.
In the operation theater (OT), an intravenous catheter was placed in the patients and Ringer lactate infusion was started. Ondansetron (100 μg/kg.), diazepam (200 μg/kg.), and pentazocine (500 μg / kg) were used as premedication. Monitored anesthesia care (MAC) was given. All patients were monitored for blood pressure (non-invasive), heart rate, electrocardiogram, and oxygen saturation by pulse oximetry. The infra-umbilical area and the McBurney's point area were infiltrated with 1% lignocaine with adrenalin, keeping the dose under 6 mg/kg of body weight, to avoid lignocaine toxicity. The pneumoperitoneum was created using carbon-di-oxide and the pressure was kept at 11 mmHg. The table was kept in the Trendelenburg position with 15° left tilt. A 0° telescope was introduced through the umbilical port for complete examination of the abdomen. A 10 mm trocar in the McBurney's point area was introduced under vision, for holding the tip of the appendix. The appendix was then identified and grasped by a non-traumatic grasper. The pneumoperitoneum was deflated after the exteriorization of the appendix through the trocar placed at the McBurney's point. The appendicectomy was performed as an open procedure. The cut end was painted with betadine (aqueous solution of 10% povidone-iodine). The appendicular stump was then reposed within the abdomen. The pneumoperitoneum was re-established for final inspection. The port site wounds were closed with 2.0 vicryl. The patients were started oral feed immediately postoperatively and solid food on the next day. Postoperative analgesia was achieved by the diclofenac patch. Patients were called for a revisit after a week for follow-up.
| Results | | |
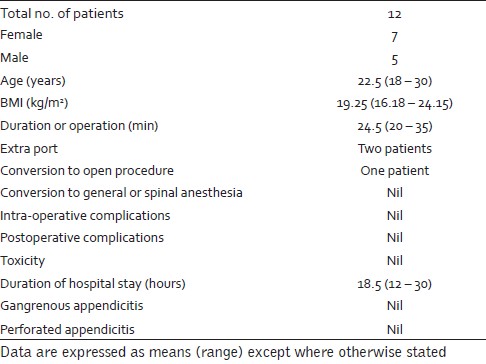
Twelve patients underwent LAA with a mean age of 22.5 years ranging from 18 to 30 years, with a mean BMI of 19.25 kg/m 2 ranging from 16.18 to 24.15 kg/m 2 . The appendix was in the normal position in nine patients and retro-cecal in three patients. Two cases required a 5 mm extra port to free the appendix from the adhesion. One case was converted to open procedure due to the presence of adhesions of inflammatory origin. The mean operative time was 24.5 minutes ranging from 20 to 35 minutes. The mean hospital stay was 18.5 hours ranging from 12 to 30 hours. No patients required conversion to general anesthesia with positive pressure ventilation or spinal anesthesia, and no patient developed signs of toxicity due to lignocaine. Two patients needed supplementation of injection ketamine 10 mg for analgesia. No postoperative complications, including wound infection, were encountered in the present study [Table 1].
| Discussion | | |
Use of local anesthesia for surgical procedures has been steadily refined since its introduction by Koller in 1884, and it is now widely used in several surgical procedures [3] like cholecystectomy, [4] thyroid surgeries, [5],[6] and appendicectomy. [7],[8] Non-compliance is the most important contraindication. Limited access for exploration, systemic toxicity due to excess amount of local anesthetics, limited duration of anesthesia, fear of failure are the reasons for avoidance of using local anesthesia for surgical procedures. Simplicity in using is the most important attraction for local anesthesia, provided the surgical procedure is limited in exploration and duration, and does not disturb the internal milieu of the human body. It avoids the complications related to spinal, epidural or general anesthesia as well as the patients' fear about the stated procedures.
The feasibility of open appendicectomy under local anesthesia was already established by Sharma et al.[7] They found it to be cost-effective, and it also carried little morbidity and could be safely used for all age groups. Diagnostic laparoscopies were tried successfully under the local anesthesia with sedation technique. We performed LAA under the MAC technique, where local anesthesia was combined with sedation and analgesia. [9] Local anesthesia was used for inserting the trocars, and sedation analgesia for creating pneumoperitoneum and excision of the appendix. MAC required less anesthesia time and avoided the related complications and cost burden of spinal or general anesthesia.
LAA has already established its safety. [10],[11] It requires less postoperative analgesia and is associated with faster recovery leading to shortened postoperative hospital stay when compared with the open technique. [12],[13] It is associated with lower postoperative complications including wound infection, and better cosmetic effect than the open technique. [13] We did not find wound infection in any case. However, other studies where the LAA technique was adopted, reported a varied number of wound infection rates. LAA was more economical and technically easier than LA. [12],[14] However, it was more expensive than the open technique. [12] Performing LAA under local anesthesia with the sedation analgesia technique made it even cheaper. Due to its short surgical time and also shortened time requirement for administration of anesthesia (MAC), its overall OT engagement duration was less, which allowed more number of operations to be taken up within the stipulated time limit. One important advantage of the laparoscopic proceeding was the outstanding overview of the abdominal cavity with the possibility of more accurate diagnosis and proper decision-making.
Two-port LAA is a safe and effective alternative for the management of uncomplicated appendicitis. However, the results cannot be generalized to overweight patients. [15] When compared with the three port technique the overall cost is less with two-port LAA and it produces an even better cosmetic effect, due to the lesser number of punctures involved.
| Conclusion | | |
The two port technique under local anesthesia is safe in uncomplicated appendicitis among low BMI patients and should now be rigorously evaluated in a randomized controlled trial, to investigate any potential advantage of this method over the conventional LAA techniques. It can be employed as the preferred technique where resources are limited.
| References | | |
| 1. | Semm K. Endoscopic appendectomy. Endoscopy 1983;15:59-64. 
[PUBMED] [FULLTEXT] |
| 2. | Li X, Zhang J, Sang L, Zhang W, Chu Z, Li X, et al. Laparoscopic versus conventional appendectomy--a meta-analysis of randomized controlled trials. BMC Gastroenterol 2010;10:129.
[PUBMED] [FULLTEXT] |
| 3. | Dennison A, Oakley N, Appleton D, Paraskevopoulos J, Kerrigan D, Cole J, et al. Local anesthesia for major general surgical procedures. A review of 116 cases over 12 years. Postgrad Med J 1996;72:105-8.
[PUBMED] [FULLTEXT] |
| 4. | Sharma LB, Agarwal M, Rastogi AN, Gupta C, Shukla VK. Cholecystectomy under local anesthesia. Indian J Surg 1999;61:33-5.
|
| 5. | Snyder SK, Roberson CR, Cummings CC, Rajab MH. Local Anesthesia With Monitored Anesthesia Care vs General Anesthesia in Thyroidectomy: A Randomized Study. Arch Surg 2006;141:167-73.
[PUBMED] [FULLTEXT] |
| 6. | Shukla VK, Narayan S, Chauhan VS, Singh DK. Thyroid surgery under local anesthesia: An alternative to general anesthesia. Indian J Surg 2005;67:316-9.
|
| 7. | Sharma LB, Agarwal M, Chaudhary L, Shukla VK. Appendicectomy under local anesthesia. Eur J Surg 1999;165:1091-2.
[PUBMED] |
| 8. | Jebbin NJ. Local anesthesia for appendicectomy: One surgeon's experience. Niger J Med 2007;16:31-3.
[PUBMED] |
| 9. | Ghisi D, Fanelli A, Tosi M, Nuzzi M, Fanelli G. Monitored anesthesia care. Minerva Anestesiol 2005;71:533-8.
[PUBMED] [FULLTEXT] |
| 10. | Tekin A, Kurtoðlu HC. Video-assisted extracorporeal appendectomy. J Laparoendosc Adv Surg Tech A 2002;12:57-60.
|
| 11. | Koontz CS, Smith LA, Burkholder HC, Higdon K, Aderhold R, Carr M. Video-assisted transumbilical appendectomy in children. J Pediatr Surg 2006;41:710-2.
[PUBMED] [FULLTEXT] |
| 12. | Nicholson T, Tiruchelvam V. Comparison of laparoscopic-assisted appendectomy with intracorporal laparoscopic appendectomy and open appendectomy. JSLS 2001;5:47-51.
[PUBMED] [FULLTEXT] |
| 13. | Malik AM, Talpur AH, Laghari AA. Video-assisted laparoscopic extracorporeal appendectomy versus open appendectomy. J Laparoendosc Adv Surg Tech A 2009;19:355-9.
[PUBMED] [FULLTEXT] |
| 14. | Fazili FM, Al-Bouq Y, El-Hassan OM, Gaffar HF. Laparoscope-assisted appendectomy in adults: The two-trocar technique. Ann Saudi Med 2006;26:100-4.
[PUBMED]  |
| 15. | Konstadoulakis MM, Gomatos IP, Antonakis PT, Manouras A, Albanopoulos K, Nikiteas N, et al. Two-trocar laparoscopic-assisted appendectomy versus conventional laparoscopic appendectomy in patients with acute appendicitis. J Laparoendosc Adv Surg Tech A 2006;16:27-32.
[PUBMED] [FULLTEXT] |
[Table 1]
|