|


 |
| CASE REPORT |
|
| Year : 2011 | Volume
: 3
| Issue : 2 | Page : 99-101 |
|
|
Squamous cell carcinoma arising in a testicular teratoma and presenting as sister Mary Joseph Nodule
Kalyan Khan1, Dibakar Bagchi2
1 Department of Pathology, North Bengal Medical College, Sushrutanagar, Darjeeling, India
2 Department of General Surgery, North Bengal Medical College, Sushrutanagar, Darjeeling, India
| Date of Web Publication | 11-Feb-2012 |
Correspondence Address:
Kalyan Khan
Flat No. 11, 'Bela' Apartment, Netaji Subhas Road, Subhaspally, Siliguri, Darjeeling - 734 001
India
 Source of Support: None, Conflict of Interest: None
DOI: 10.4103/2006-8808.92804

 Abstract Abstract | | |
The most common somatic type malignancy arising in patients with testicular germ cell tumors (GCTs) is sarcoma. Development of carcinomas, especially squamous cell carcinoma is an extremely rare event. Most cases of metastatic umbilical nodules (Sister Mary Joseph nodule) develop from adenocarcinomas. Fifteen percent of such cases have unknown origin; but development from a testicular squamous cell carcinoma has not yet been reported in the literature. We report a rare case of somatic type squamous cell carcinoma arising in a testicular teratoma. It is also possibly the first reported case of its kind which presented with a metastatic umbilical nodule. This possibility should be kept in mind while evaluating metastatic umbilical nodules in young male patients. Keywords: Sister Mary Joseph nodule, squamous cell carcinoma, teratoma, testicular germ cell tumors
How to cite this article:
Khan K, Bagchi D. Squamous cell carcinoma arising in a testicular teratoma and presenting as sister Mary Joseph Nodule. J Surg Tech Case Report 2011;3:99-101 |
How to cite this URL:
Khan K, Bagchi D. Squamous cell carcinoma arising in a testicular teratoma and presenting as sister Mary Joseph Nodule. J Surg Tech Case Report [serial online] 2011 [cited 2016 Jun 12];3:99-101. Available from: http://www.jstcr.org/text.asp?2011/3/2/99/92804 |
| Introduction | |  |
The most common somatic type malignancy arising in patients with testicular germ cell tumors (GCTs) is sarcoma. [1] Development of carcinomas, especially squamous cell carcinoma is an extremely rare event. [1],[2] Most cases of metastatic umbilical nodules (Sister Mary Joseph nodule) develop from adenocarcinomas. [3] Fifteen percent of such cases have unknown origin [4] but development from a testicular squamous cell carcinoma has not yet been reported in the literature. We report a rare case of somatic type squamous cell carcinoma arising in a testicular teratoma. It is also possibly the first reported case of its kind which presented with a metastatic umbilical nodule.
| Case Report | | |
A 22-year-old male patient presented with diffuse abdominal pain and anorexia for last two months and a painless umbilical nodule of one-month duration which had recently ulcerated. On examination a solid, firm, nontender, irregular right testicular swelling was palpable. Mild hepatomegaly was also detected. A superficial umbilical nodule measuring 3.9 × 2.3 cm [Figure 1] with surface ulceration was detected. Whole abdominal ultrasonography revealed an 8 × 3 cm heterogeneous space-occupying lesion (SOL) of the right testis with multiple small nodules in the right tunica vaginalis [Figure 2] and bilateral vaginal hydrocele. Two hypoechoic masses measuring 9.4 × 8 cm and 2.8 × 2.5 cm, the former with central cystic degeneration were seen in the right lobe of the liver. A superficial SOL with similar echogenecity was noted at the umbilicus. All the masses appeared neoplastic on imaging and multiple metastases with adhesions were detected in the periaortic region along with mild left hydronephrosis and hydroureter. Moderate elevations of serum beta human chorionic gonadotrophin (HCG) (11.02 mIU/ml) and lactate dehydrogenase (LDH) (683.7 IU/L) levels were found but serum alpha fetoprotein (AFP) level was within normal limits (4.91 ng/ml). Complete blood count showed microcytic hypochromic anemia and raised Erythrocyte Sedimentation Rate (ESR). Chest X-ray revealed no abnormality.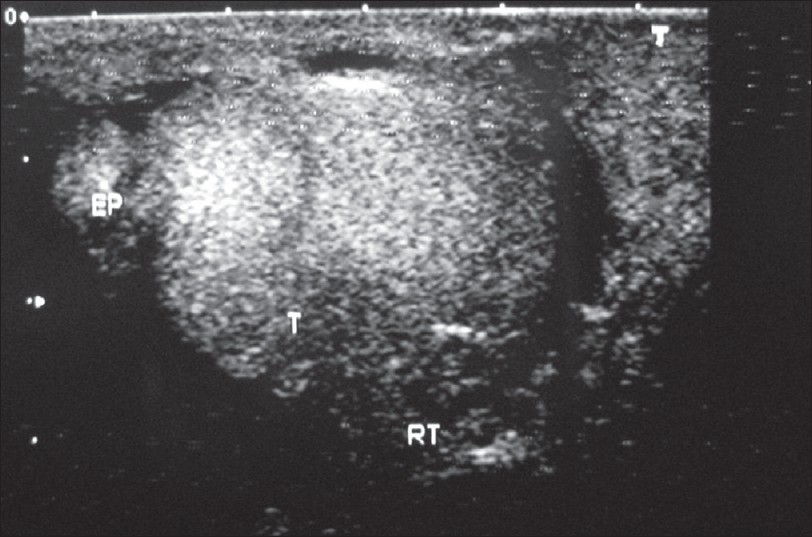 | Figure 2: Ultrasonogram of heterogeneous SOL of the right testis with multiple small nodules in the tunica vaginalis and vaginal hydrocele
Click here to view |
Fine needle aspiration cytology (FNAC) performed from both the umbilical nodule and the hepatic lesions revealed metastatic deposits of squamous cell carcinoma [Figure 3]. Ill-defined granulomas were additionally detected in the umbilical aspirates.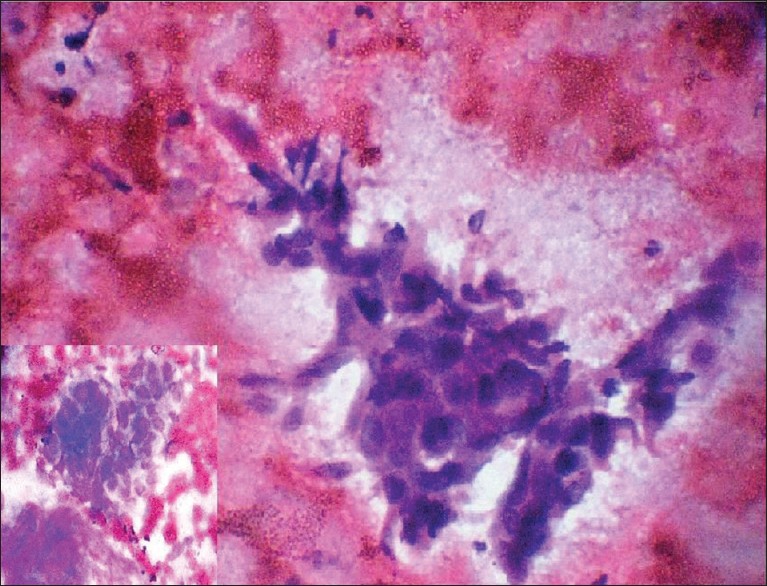 | Figure 3: FNAC from hepatic SOL showing metastatic squamous cell carcinoma (Pap; × 400). Inset - FNAC from umbilical nodule showing metastatic deposits of squamous cell carcinoma (Leishman; × 400)
Click here to view |
Right-sided high inguinal orchiectomy was done. No inguinal lymph nodes were detected and scrotum was found to be free peroperatively. On cut section twothirds of the testicular tissue was found to be replaced by a whitish inhomogeneous fleshy mass with similar nodular deposits on the surface.
Histopathology revealed well-differentiated (keratinizing) squamous cell carcinoma with plenty of keratin pearl formation invading the testicular tissue [Figure 4]. Elsewhere, foci of teratoma were detected and the existing seminiferous tubules showed gross suppression of spermatogenesis. No IGCNU (intratubular germ cell neoplasia unspecified) or other "in situ" lesions were found after careful histopathological examination.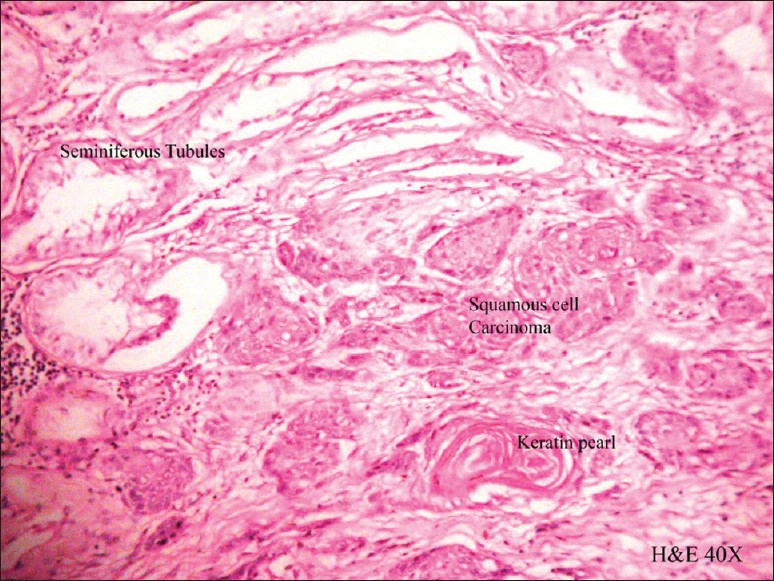 | Figure 4: Well-differentiated squamous cell carcinoma invading the testicular tissue; the seminiferous tubules show gross suppression of spermatogenesis (H and E; × 100)
Click here to view |
The patient showed no response to three pulses of first-line postoperative chemotherapy with Cisplatin and 5 Fluorouracil (5FU). Institution of second-line chemotherapy was being planned but before that the patient died of disseminated carcinoma and multiorgan failure 25 weeks after initial presentation.
| Discussion | | |
Testicular germ cell neoplasia, a disease predominantly of young men, is, for unknown reasons, increasing in incidence. [5] The World Health Organization (WHO) has defined teratoma with somatic type malignancy (ICDO code 9084/3) as a teratoma containing a malignant component of a type typically encountered in other organs and tissues, e.g. sarcomas and carcinomas. [6] Carcinomas are less often associated with GCTs. When uncommon somatic type malignancies (usually squamous cell carcinoma) occur in mature cystic teratomas of the ovary, this is a de novo form of malignant transformation; similar tumors in the testis, a very rare event, represent overgrowth of teratomatous elements that originated from malignant, non-teratomatous germ cell tumors and, therefore, had previously undergone malignant transformation. [2]
Tumors that metastasize to the testis are extremely rare. Among them, the lung is the most common primary site. [7]
Lymphatic spread from nonseminomatous testicular tumors is usually localized in retroperitoneal lymph nodes including aortic, common iliac and caval nodes. [8]
In metastatic sites, the somatic-type malignancies have a poor prognosis. They do not respond to germ cell tumor chemotherapy; surgical resection is the treatment of choice. [9]
An umbilical metastatic lesion is called 'Sister Mary Joseph's nodule'. It is an uncommon clinical or radiographic finding, and it is rare as the first sign of a malignant disease. [10] A review of all 407 cases of umbilical metastatic lesion published during the period 1966 to 1997 showed the most common origin to be gastrointestinal (52%). [4] Even after a diligent search of the published literature not a single reported case was found in which squamous cell carcinoma arising in the testis was detected as the origin of an umbilical metastasis.
How exactly the metastases reach the umbilicus remains largely unknown. Proposed mechanisms for the spread of cancer cells to the umbilicus include direct transperitoneal spread, via the lymphatics which run alongside the obliterated umbilical vein, hematogenous spread, or via remnant structures such as the falciform ligament, median umbilical ligament, or a remnant of the vitelline duct. [11]
The reported case is extremely rare as somatic type squamous cell carcinoma arises sparingly in a testicular teratoma. Above that, it is also possibly the first reported case of its kind which presented with a metastatic umbilical nodule. This possibility should be kept in mind while evaluating metastatic umbilical nodules in young male patients.
| Acknowledgment | | |
Dr. Narayan Pandit, Assistant Professor, Department of Radiodiagnosis, North Bengal Medical College. Dr. Rajat Bandyopadhyay, Assistant Professor, Department of Radiotherapy, North Bengal Medical College.
| References | | |
| 1. | Ulbright TM, Loehrer PJ, Roth LM, Einhorn LH, Williams SD, Clark SA. The development of non-germ cell malignancies within germ cell tumors. A clinicopathologic study of 11 cases. Cancer 1984;54:1824-33. 
[PUBMED] |
| 2. | Ulbright TM. Germ cell tumors of the gonads: A selective review emphasizing problems in differential diagnosis, newly appreciated, and controversial issues. Mod Pathol 2005;18 Suppl 2:S61-79.
[PUBMED] [FULLTEXT] |
| 3. | Majmudar B, Wiskind AK, Croft BN, Dudley AG. The Sister (Mary) Joseph nodule: Its significance in gynecology. Gynecol Oncol 1991;40:152-9.
[PUBMED] |
| 4. | Galvan VG. Sister Mary Joseph's nodule. Ann Intern Med 1998;128:410.
|
| 5. | Ulbright TM. Germ cell neoplasms of the testis. Am J Surg Pathol 1993;17:1075-91.
[PUBMED] |
| 6. | Eble JN, Sauter G, Epstein JI, Sesterhenn IA. World Health Organization Classification of Tumours. Pathology and Genetics of Tumours of the Urinary System and Male Genital Organs. Lyon: IARC Press; 2004. p. 212-3.
|
| 7. | Nistal M, Gonzalez-Peramato P, Paniagua R. Secondary testicular tumors. Eur Urol 1989;16:185-8.
|
| 8. | Weissbach L, Boedefeld EA. Localization of solitary and multiple metastases in stage II nonseminomatous testis tumor as basis for a modified staging lymph node dissection in stage I. J Urol 1987;138:77-82.
[PUBMED] |
| 9. | Loehrer PJ Sr, Hui S, Clark S, Seal M, Einhorn LH, Williams SD, et al. Teratoma following cisplatin-based combination chemotherapy for nonseminomatous germ cell tumors: A clinicopathological correlation. J Urol 1986;135:1183-9.
[PUBMED] |
| 10. | Larentzakis A, Theodorou D, Fili K, Manataki A, Bizimi V, Tibishrani M, et al. Sister Mary Joseph's nodule: Three case reports. Cases J 2008;1:182.
[PUBMED] [FULLTEXT] |
| 11. | Cohen DC. A man with an umbilical ulcer. Medscape J Med 2008;10:11.
[PUBMED] [FULLTEXT] |
[Figure 1], [Figure 2], [Figure 3], [Figure 4]
|
















