|


 |
| ORIGINAL ARTICLE |
|
| Year : 2012 | Volume
: 4
| Issue : 2 | Page : 86-88 |
|
|
Patient Satisfaction Following Minimally Invasive Repair of Pectus Excavatum: Single Surgeon Experience
Anupama Barua1, Vinay P Rao2, Biplab Barua3, Andrzej Majewski2
1 Department of Cardiac Surgery, Leeds General Infirmary, Leeds, United Kingdom
2 Department of Thoracic Surgery, Nottingham City Hospital, Nottingham, United Kingdom
3 Department of General Surgery, Royal Shrewsbury Hospital, Shrewsbury, United Kingdom
| Date of Web Publication | 8-Apr-2013 |
Correspondence Address:
Anupama Barua
Department of Cardiac Surgery, Leeds General Infirmary, Great George Street, Leeds, LG13EX
United Kingdom
 Source of Support: None, Conflict of Interest: None  | 2 |
DOI: 10.4103/2006-8808.110253

 Abstract Abstract | | |
Background: Pectus excavatum (PE) is the most common chest wall deformity in adolescent life. Nuss procedure is a well-established technique for the repair of PE. The indication for correction is mainly medical aesthetic. Advantages of Nuss over conventional methods include reduced length of hospital stay, smaller incisions, and absence of need for osteochondrectomies. Here, we describe our experience with this procedure. Materials and Methods: This was a retrospective study of patients who underwent Nuss procedure by a single surgeon between 2006 and 2010 in a regional center. Indications for surgery included the following: Progressive deformity and psychological stress. All patients underwent chest X-ray and pulmonary function testing. A standard Nuss procedure was performed using a single bar. Patients' satisfaction was assessed by a questionnaire and follow-up clinic letters. Satisfaction with body image was scored on a scale of 1-10. Results: Eleven patients with PE underwent correction by Nuss procedure. Mean age of the patient was 19 years (range: 15-30). The average hospital stay was 7 days (range: 4-23 days). There was no mortality and no episodes of wound infection. In the immediate post-operative period, three patients (12.5%) were noted to have poor pain control. The post-operative course was uneventful in all cases except one patient who developed lung collapse, pleural effusion, and bar dislocation. Hundred percent of patients were satisfied with the scar. Seven patients scored 7 out of 10 on satisfaction with body image and two patients scored 6 or less. None of the patients complained of chronic pain. Conclusion: Nuss procedure is an effective method for the correction of PE. Most patients were satisfied with the outcome and none experienced chronic pain. Keywords: Nuss procedure, patient satisfaction, pectus excavatum
How to cite this article:
Barua A, Rao VP, Barua B, Majewski A. Patient Satisfaction Following Minimally Invasive Repair of Pectus Excavatum: Single Surgeon Experience. J Surg Tech Case Report 2012;4:86-8 |
How to cite this URL:
Barua A, Rao VP, Barua B, Majewski A. Patient Satisfaction Following Minimally Invasive Repair of Pectus Excavatum: Single Surgeon Experience. J Surg Tech Case Report [serial online] 2012 [cited 2016 Jun 10];4:86-8. Available from: http://www.jstcr.org/text.asp?2012/4/2/86/110253 |
| Introduction | |  |
One of the most common thoracic deformities in childhood and adolescent life is pectus excavatum (PE). The prevalence of this disease is 1 in 400 with a male preponderance. [1] This can be expressed as symmetrical and asymmetrical deformities. It may be associated with Marfan's syndrome and Ehlers-Danlos syndrome. This deformity is more pronounced during puberty as the thoracic circumference increases upto 50% during the growth period of puberty.
The most common reason for seeking medical attention is deformity. On very few occasions, PE causes exercise intolerance due to impaired activity of important thoracic organs such as lung and heart. There is variable evidence of cardiopulmonary performance in PE patients in literature. Malek et al. [2] suggested that impaired cardiovascular performance is more important than limitation of ventilation for poor exercise tolerance in PE. One standard way for evaluation of the severity of PE is Heller's cardiothoracic index. This measures the ratio between the transverse and anterior-posterior diameters of the thoracic cavity at the point of most pronounced deformity.
The classical treatment for PE described by Ravitch in 1977 [3] involves multiple osteotomies of the sternum and costal cartilages to facilitate adequate lifting and stabilization of the anterior chest wall. The most significant disadvantage in patients' outcome is scar in anterior chest wall.
Donald Nuss, a pediatric surgeon, described a minimally invasive procedure to raise the sternum by inserting a retrosternal bar under thoracoscopic guidance. [4] This bar helps to correct and reduce the deformity by refashioning the contour of the growing thorax. This procedure produces little scarring and more or less pain-free post-operative period and fewer post-operative complications in comparison to classical Ravitch procedure. The advantage of Nuss over an open procedure is avoidance of osteotomies to encourage normal skeletal growth in the thorax.
Here, we present this retrospective study with continuous series of 11 patients who were who were treated with placement of retrosternal bar as described by Nuss. [4]
| Materials and Methods | | |
From 2006 to 2010, 11 patients underwent correction of PE by Nuss procedure. All patients complained of an unacceptable body image and presented with deformity of the chest wall. All patients were subjected to baseline lung function tests and chest radiography. Computed tomography scans of the thorax were not carried out in any patient.
A single surgeon in the Department of Thoracic Surgery, Nottingham, UK operated on all patients from 2006 to 2010. All of them were male with a mean age of 19 years (range: 15-30). Ten patients have symmetric PE and one presented with asymmetric PE.
The operation was performed in a supine position under general anesthesia, endotracheal intubation, and appropriate muscle relaxation. At first bilateral thoracic, small incisions were made along the axillary lines and tunnels created under pectoral muscles. Right thoracoscopy facilitated visualization of the space and the passage of the bar between the sternum and the pericardium. The pre-shaped bar was then drawn through the chest with the convex side down. After satisfactory placement, polydioxanone sutures were used to stabilize the bar.
Chest X-ray was performed in the recovery room and on the second post-operative day (POD). Epidural anesthetics were administered until the second or third POD according to analgesic need. Patients were asked to sleep in the supine position for the first 2 weeks. Patients were discharged from hospital after ensuring adequate analgesia and independent mobility with the length of hospital stay ranging from 4 to 23 days (median = 7 days).
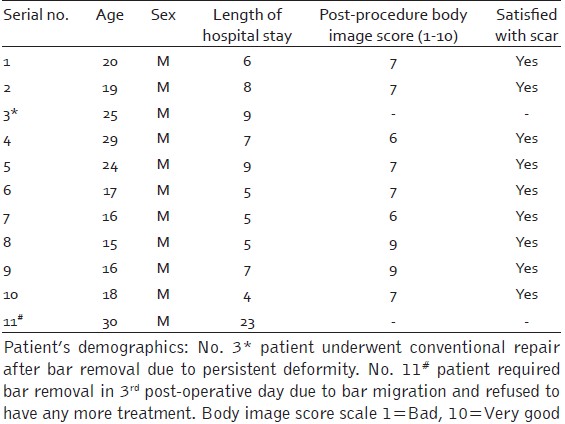
Post-operative complications were determined from the hospital database. Patients' satisfaction over the body image was confirmed by telephone questionnaires and follow-up clinic letters. The patients' demographics and satisfaction scores are illustrated in [Table 1].
| Results | | |
Of the 11 patients who underwent Nuss procedure, 10 patients underwent repair in a minimally invasive fashion. Blood loss was minimal in all patients and none of them required a blood transfusion. All of them were extubated in theater and were admitted to the ward with epidural analgesia.
Early major complications such as respiratory failure, atelectasis, and bar migration were observed in one patient. On the third POD, bar was removed due to migration of the bar, other options were offered, but patient refused to have any other treatment. Three patients complained of initial poor pain control in the immediate post-operative period. This was addressed with additional oral analgesia to the patients' satisfaction.
Patients were followed up at 6 weeks following surgery and at 3-monthly intervals in the 1 st year and 6-monthly intervals in the 2 nd year. Excellent surgical outcome was observed in nine patients at the 6-week follow-up appointment. One patient had persistent chest wall deformity and underwent Ravitch repair after bar removal. In the follow-up clinic, the remaining nine patients were satisfied with the scar and pain control. Seven patients scored more than 7 on satisfaction with body image and two patients scored less than 7.
The Nuss bar was removed in five patients after 18-24 months of bar application. No complications were observed during or after bar removal.
| Discussion | | |
Recently, more patients are treated with minimal invasive techniques to correct PE. The results are satisfactory with low complication rates, minimal scarring, and high patients' satisfaction. Nuss performed this procedure in the 3-6 years age group to maximize chest wall pliability. [4] It is also suggested that after puberty, chest is less malleable and operative outcomes are relatively poor. [5],[6],[7] But in our study, the patient's average age was 18.9 years (range: 15-30). However, 63% of the patients showed satisfactory results. Our evaluation of post-operative cosmetic results was based on telephone questionnaires to patients and revealed good results with body image and pain control. According to the data provided by other authors, cardiac function is significantly improved and patients' well-being is improved, [8] but there was no evidence of an objective improvement in pulmonary function. [9] Our study adds to the evidence that Nuss procedure results in patients' satisfaction over their body image. This is consistent with the results of Lawsen et al. who reported positive physical and psychological well-being in the child following repair of PE. [10]
According to some authors, the rates of surgical complications with Nuss have been high (10.1% early and 14% late). [4],[11],[12] These complications include pleural effusion, poor post-operative pain control, wound infection, bar infection, bar displacement, allergic reactions, pneumonia, cardiac arrhythmia, pericardial effusion, and secondary pneumothorax. In our study, one patient was noted to have bar dislocation, lung collapse, and respiratory failure.
Nuss et al. noted that the long-term results after bar removal were excellent in 71% of cases, good in 21% of cases, and recurrences noted in 7.8% of patients. In our study, five patients have undergone bar removal. No post-operative complications were observed after removal of bar. An adequate contour of the anterior chest wall was maintained 6 weeks after bar removal. Long-term follow-up is required to draw conclusions regarding long-term outcomes.
A persistent chest wall deformity is common in patients undergoing operations at a later age. [13] Gilbert et al. have reported a 60% recurrence in patients over 12 years of age at the time of operation. [14] In our study, none of them required re-operation; one patient aged 26 years required an open procedure after an attempted initial Nuss procedure resulted in a persistent and significant chest wall asymmetry.
Our study emphasizes the effectiveness of Nuss procedure for cosmetic improvement of PE. Moreover, the relatively uneventful post-operative recovery in comparison to conventional techniques is encouraging.
| Conclusion | | |
Our limited study demonstrated that Nuss procedure for PE results in patients' satisfaction. The post-operative complication rates are low and these can be managed without admission to intensive therapeutic unit (ITU). Good surgical outcomes and better cosmetic results encourage us to continue offering this procedure to adolescent patients.
| References | | |
| 1. | Huddleston CB. Pectus excavatum. Semin Thorac Cardiovasc Surg 2004;16:225-32. 
|
| 2. | Malek MH, Fonkalsrud EW, Cooper CB. Ventilatory and cardiovascular responses to exercise in patients with pectus excavatum. Chest 2003;124:870-82.
|
| 3. | Ravitch MM. Repair of pectus excavatum in children under 3 years of age: A twelve-year experience. Ann Thorac Surg 1977;23:301.
|
| 4. | Nuss D, Kelly RE Jr, Croitoru DP, Katz ME. A 10-year review of a minimally invasive technique for the correction of pectus excavatum. J Pediatr Surg 1998;33:545-52.
|
| 5. | Nuss D, Croitoru DP, Kelly RE Jr, Goretsky MJ, Nuss KJ, Gustin TS. Review and discussion of the complications of minimally invasive pectus excavatum repair. Eur J Pediatr Surg 2002;12:230-4.
|
| 6. | Croitoru DP, Kelly RE Jr, Goretsky MJ, Lawson ML, Swoveland B, Nuss D. Experience and modification update for the minimally invasive Nuss technique for pectus excavatum repair in 303 patients. J Pediatr Surg 2002;37:437-45.
|
| 7. | Engum S, Rescorla F, West K, Rouse T, Scherer LR, Grosfeld J. Is the grass greener? Early results of the Nuss procedure. J Pediatr Surg 2000;35:246-51.
|
| 8. | Sigalet DL, Montgomery M, Harder J, Wong V, Kravarusic D, Alassiri A. Long term cardiopulmonary effects of closed repair of pectus excavatum. Pediatr Surg Int 2007;23:493-7.
|
| 9. | Kubiak R, Habelt S, Hammer J, Häcker FM, Mayr J, Bielek J. Pulmonary function following completion of minimally invasive repair for pectus excavatum (mirpe). Eur J Pediatr Surg 2007;17:255-60.
|
| 10. | Lawson ML, Cash TF, Akers R, Vasser E, Burke B, Tabangin M, et al. A pilot study of the impact of surgical repair on disease-specific quality of life among patients with pectus excavatum. J Pediatr Surg 2003;38:916-8.
|
| 11. | Nuss D. Minimally invasive surgical repair of pectus excavatum. Semin Pediatr Surg 2008;17:209-17.
|
| 12. | Hosie S, Sitkiewicz T, Petersen C, Göbel P, Schaarschmidt K, Till H, et al. Minimally invasive repair of pectus excavatum - The Nuss procedure. A european multicentre experience. Eur J Pediatr Surg 2002;12:235-8.
|
| 13. | Backer OG, Brunner S, Larsen V. The surgical treatment of funnel chest. Initial and follow-up results. Acta Chir Scand 1961;121:253-61.
|
| 14. | Gilbert JC, Zwiren GT. Repair of pectus excavatum using a substernal metal strut within a marlex envelope. South Med J 1989;82:1240-4.
|
[Table 1]
|